
Government of the District of Columbia
Department of Health
Health Regulation and Licensing Administration
BOARD OF MEDICINE
APPLICATION INSTRUCTIONS AND FORMS FOR A LICENSE
TO PRACTICE MEDICINE AND OSTEOPATHY IN THE DISTRICT OF COLUMBIA
This package contains the forms to apply for a license to practice medicine (allopathic or osteopathic) in the District
of Columbia. If you are applying by examination or re-examination (United States Medical Licensing Examination
(USMLE) - Step 3), you should also have an examination registration packet for the exam in addition to this
package. All forms required to apply for licensure are included in this package.
THE APPLICATION PROCESS
Phase 1- Processing: Your application, photos and fees, made payable to DC Treasurer, must be submitted, and all
supporting documents required must be received by the processing department within 120 calendar days of
submission of your application. Please note that if any supporting documents are received before your application
is received, they will be discarded. Notifications regarding missing documentation will be sent to you at the 30,
60, and 90-day mark. Once all of your documents have been received, your application will have successfully
completed the processing phase and will be referred to the Health Licensing Specialist (HLS) for analysis.
Phase 2- Analysis: The HLS will conduct a more detailed review of all the documents you have provided. If
necessary, further information may be requested from you by the HLS to complete the analysis phase. Once phase 2
is completed, your application is marked as pending board approval and referred to the Board of Medicine (the
Board) for review.
Phase 3- Decision: All applicants for licensure are thoroughly reviewed by the Board. The full Board meets on the
last Wednesday of each month, except for the month of August. Once your application has been reviewed by the
Board, and if found to be in accordance with the statutes and regulations for licensure approval, a license certificate
will be mailed to you within one week.
If the Board determines that your application does not completely comply with any of the statutory or regulatory
criteria for licensure, the Board may ask you for additional information, or ask that you come before them to answer
further questions relevant to determining licensure approval. If the Board finds that you do not meet the
requirements for licensure or that there is a legal or practice issue that bears upon your fitness for licensure, they
may formally request that you withdraw your application or notify you that they intend to deny your request for
licensure. If the Board elects to initiate a formal action to deny your application for licensure, you will be provided
with notice of the Board’s intent and an opportunity to request a hearing.
Once Phase 1 of your application has been satisfied, notification of a decision is usually provided within two to
four weeks.
Please note that application and processing fees, once submitted, are non-refundable after 120 business days.

2 | P a g e
Updated 10/03/11
WHERE TO FILE
All new license applications and documents should be sent to the following address:
Department of Health
Health Professional Licensing Administration (“HPLA”)
Board of Medicine 899 North Capitol Street, NE
First Floor
Washington, DC 20002
Checks or money orders for application and license fees should be made payable to DC Treasurer and submitted
along with your application. Checks or money orders for examination fees should be made payable to “USMLE” at
the address shown on the examination fee form. Do not send cash.
As a candidate, you must apply to the Board of Medicine for licensure at the same time you apply to take the
examination. Once your are approved to take the examination, you will be contacted by the Federation of State
Medical Boards of the United States, Inc. (FSMB) to schedule your examination.
If you have any questions, call HPLA’s Customer Service line at 1-877-672-2174 between 8:15 a.m. and 4:40 p.m.
EST Monday through Friday. Please read these instructions carefully to facilitate prompt processing of your
application. Illegible applications and applications submitted without required signatures or with incorrect fees will
be returned in their entirety, including fees. Please print or type all information except signatures.
METHODS OF LICENSURE AND QUALIFICATIONS
There are five basic methods for becoming licensed to practice medicine in the District of Columbia. These
methods include:
Examination: First attempt in D.C. to pass USMLE, Step 3.
Re-examination: Second or subsequent attempt in D.C. to pass USMLE, Step 3. Note: after 3 failures in any
jurisdiction of USMLE, Step 3, applicants are required to complete an additional year of
ACGME or AOA approved postgraduate training.
License by Exam: Successful completion of USMLE (Steps 1, 2 & 3); NBME or NBOME (Parts 1, 2 & 3), or
FLEX (Components 1 & 2; or Components 1, 2 & 3 in a single sitting for pre-1985
examinees); the licensing examination that is administered by the Licentiate of the Medical
Council of Canada; combinations of FLEX, NBME, and USMLE as specified in section 17
DCMR 4605.1-14 of the Medical regulations; or passing a state constructed examination
that is judged by the Board to be substantially equivalent to the requirements of the license
law prior to June 30, 1979, and meet other requirements.
Eminence 1* A foreign trained physician, who is of recognized eminence and standing in a field of
medicine or medical research in the international community and meets additional
requirements as outlined in 4608.1; has practiced for at least ten (10) years, has
successfully completed a two-year clinical training program in the United States; possesses

3 | P a g e
Updated 10/03/11
a valid ECFMG certificate and a foreign license in good standing, may demonstrate
eminence to the satisfaction of the Board and meet other requirements.
Eminence 2** A foreign trained physician who has practiced at least ten (10) years, who is nominated by
the Dean of an accredited school of medicine in District of Columbia, the Director of the
National Institutes of Health or the Director of an accredited and licensed hospital in the
District of Columbia, and meets other requirements. License is limited to practice of a
specialty at the nominating institution.
* See DC Municipal Regulations (DCMR) Title 17, § 4608.
GENERAL REQUIREMENTS FOR ALL APPLICANTS
All applicants for a license to practice medicine in the District of Columbia shall meet the following requirements:
1. Applicant must be at least 18 years of age; and
2. Applicant must not have been convicted of a crime of moral turpitude, which bears
directly on the applicant's fitness to be licensed.
All applicants must submit the following in order to be considered for licensure:
3. A complete and signed application, including required supporting documents; and
4. two (2) identical, recent passport-size photographs (2x2 inches in size) on a plain
background, which are front-view and fade-proof. The photos must be original photos and
cannot be computer-generated copies or paper copies. Please be sure to mail in your two photos and
write on the back of the photos your full name and Social Security Number. Photos will be placed on
the pocket license.
5. You will also need to submit one (1) clear photocopy of a government issued photo ID,
such as your valid driver’s license, as proof of identity.
EDUCATION AND EXPERIENCE REQUIREMENTS FOR APPLICANT EDUCATED IN THE UNITED
STATES AND CANADA
A. An applicant educated in the United States or Canada shall furnish proof satisfactory to the Board
that the applicant has successfully completed the following education and training:
1. Two Years of premedical studies at an accredited institution;
2. The equivalent of 4 years of instruction and training at a school which is legally chartered or
organized in the United States or Canada and was accredited at the time of the applicant's graduation
by the Liaison Committee on Medical Education (LCME) of the American Medical Association
(AMA), the American Osteopathic Association (AOA), or the Committee on the Accreditation of
Canadian Medical Schools. Applicants must be in receipt of the degree of Doctor of Medicine or
Doctor of Osteopathy; and

4 | P a g e
Updated 10/03/11
3. One (1) year of postgraduate clinical training, except those applicants who graduated prior
to January 1, 1990, and applicants using Step 3 of the United States Medical Licensing Examination
as part of their examination requirement, shall only be required to have one (1) year of postgraduate
clinical training. All postgraduate clinical training must be at a hospital or health care facility
licensed in the United States in a program accredited by the Accreditation Council for
Graduate Medical Education (ACGME) or the American Osteopathic Association (AOA) or in
Canada accredited by the LMCC.
B. Applicants shall arrange for a certified transcript of the applicant's premedical and medical
education to be sent directly to the applicant in a sealed envelope from the institution so that the transcript in a
sealed envelope can be submitted with the application.
EDUCATION AND EXPERIENCE REQUIREMENTS FOR APPLICANT EDUCATED OUTSIDE THE
UNITED STATES AND CANADA
A. Applicant's educated in a foreign country shall furnish proof satisfactory to the Board that the applicant's
education and training are substantially equivalent to the requirements for US and Canadian graduates by
submitting:
1. Proof satisfactory to the Board that the applicant has received the equivalent of two
academic years of instruction at the post-secondary level, including courses in following
subject:
a. Biology,
b. Inorganic Chemistry,
c. Organic Chemistry; and
d. Physics
Please note that, the curricula at some foreign universities do not specifically identify on the
transcript the individual courses listed above. If your transcript does not show these specific courses,
you are required to submit a notarized statement that you have taken the equivalent of these courses.
2. Proof satisfactory to the Board that the applicant has completed all educational and training
requirements to practice medicine in the foreign country where the medical education
was undertaken:
3. Documentation of completion of three (3) years of postgraduate clinical training in a
program accredited by the ACGME, the LMCC or the AOA; and
4. A notarized, valid certificate from the Educational Commission for Foreign Medical
Graduates (ECFMG).
B. Applicants shall arrange for a certified transcript of the applicant's premedical and medical education to be
sent directly to the applicant so that the transcript can be submitted with the application in a sealed
envelope unless the transcript is in a language other than English.

5 | P a g e
Updated 10/03/11
C. If any document is in a language other than English, the applicant shall arrange for its translation into
English before submission by a translation service acceptable to the Board and shall submit a notarized
translation signed by the translator attesting to its accuracy.
FIFTH PATHWAY PROGRAM APPLICANTS
A. An applicant educated in the Fifth Pathway Program shall furnish proof satisfactory to the Board that the
applicant:
1. Was a resident of the United States during the period of enrollment in the foreign medical
school;
2. Has successfully completed the didactic curriculum of a foreign medical school listed in the
directory of medical schools published by the World Health Organization;
3. Has attained a passing grade on Foreign Medical Graduate Examination in Medical
Sciences (FMGEMS);
4. Has completed one year of individually supervised clinical training, if the applicant
graduated prior to January 1, 1990, or has completed two years of individually supervised clinical
training, if applicant graduated after January 1, 1990, under the direction of a medical school
accredited by the LCME at a level satisfactory to the Board; and
5. Possesses a Fifth Pathway Program Certificate.
B. Applicants shall arrange for a certified transcript of the applicant's premedical and medical education to be
sent directly to the applicant in a sealed envelope, so the transcript can be submitted with the application.
C. If any document is in a language other than English, the applicant shall arrange for its translation into
English before submission by a translation service acceptable to the Board and shall submit a notarized
translation signed by the translator attesting to its accuracy.
EXAMINATION REQUIREMENTS
A. An applicant taking step 3 of the USMLE shall furnish proof satisfactory to the Board that the applicant:
1. Has passed steps 1 and 2 of the USMLE; and
2. Has successfully completed one year in a program of postgraduate clinical training in a
program accredited by ACGME, LMCC or AOA.
B. An applicant who has not attained a passing score on Step 3 of the USMLE after three (3) attempts shall
complete one (1) additional year of accredited postgraduate clinical training before being eligible to take
step 3 again.
C. An applicant who has not attained a passing score on all three parts of the USMLE within a seven (7) year
period, beginning with passing either Step 1 or Step 2, may not be eligible for licensure in the District of
Columbia; however, this period may be extended at the discretion of the Board of Medicine.

6 | P a g e
Updated 10/03/11
D. An applicant who is enrolled in a dual degree program (e.g., MD/PhD, MD/MPH, or MD/MBA) or
engaged in other continuous educational or research training with a board certification in an ABMS
specialty, shall satisfactorily complete all parts of the USMLE examination (1, 2, and 3) within ten (10)
years after passing Step 1 or 2 of the examination. This period may be extended at the discretion of the
Board of Medicine.
E. Applicants applying for licensure by examination may rely on any of the examination combinations shown
below, provided that an acceptable combination is completed prior to January 1, 2000.
Examination Sequence Acceptable Combinations
_____________________________________________________________________________________
NBME (or NBOME)
Part I NBME Part I or USMLE Step 1
plus plus
Part II NBME Part II or USMLE Step 2
plus plus
Part III NBME Part III or USMLE Step
Examination Sequence Acceptable Combinations
_____________________________________________________________________________________
FLEX Component 1 FLEX Component 1
plus plus
FLEX Component 2 USMLE Step 3
or
NBME Part 1 or USMLE Step 1
plus
NBME Part II or USMLE Step 2
plus
FLEX Component 2
Examination Sequence Acceptable Combinations
_____________________________________________________________________________________
USMLE Step 1
plus
USMLE Step 2
plus
USMLE Step 3

7 | P a g e
Updated 10/03/11
WAIVER OF EXAMINATION
The Board shall waive the examination requirement for an applicant who has passed:
A. The FLEX examination prior to 1985 in a single sitting and in less than seven attempts; or
B. The FLEX examination in 1985 or later in less than seven attempts; or
C. Examination of the Licentiate of the Medical Council of Canada; or
D. The National Board Examination and is a diplomate of the National Board of Medical Examiners; or
E. The National Osteopathic Board Examination and is diplomate of the National Board of Osteopathic
Examiners; or
F. A State certified examination prior to June 30, 1979 and holds a license in good standing in a
jurisdiction of the United States with requirements substantially equivalent to the requirements for
licensure in the District of Columbia.
INFORMATION ON SUBMISSION AND REQUIREMENTS
A. DC New License Application for Medical Doctors and Osteopaths
This is the primary document in your application. Follow instructions on the form and complete all sections. If
you require more space for work experience or need to provide explanations for screening questions, attach
typed responses to the form. Note that you are to request verification of licensure from states where you have
held a license to be sent directly to the DC Board of Medicine at the address on page 1. You should contact the
applicable boards of medicine by phone before sending them a request by mail. Almost every state charges a
fee for verifying licensure, and you should determine the fee and include the appropriate fee with your request
for verification to the state of licensure in order to expedite the process.
B. Character Reference Form
The character reference form must be submitted in a sealed envelope along with your application. A form
must be completed by each employer/training program within the past five (5) years. A physician (MD/DO)
with whom you worked or trained with must complete the form. Character reference forms may be
downloaded at www.hpla.doh.dc.gov/bomed.
C. Documentation of post-graduate experience (internships, residencies, and fellowships)
D. AMA Physician Profile
All applicants must request an AMA profile from the American Medical Association. It does not matter
whether the applicant is a member of the AMA. The AMA may be contacted by phone at (312) 464-5195. An
application is attached. Applicants should request that the AMA profile be sent to the Board of Medicine at
the address shown on page 1. You can also request an AMA Profile online at http://www.ama-
assn.org/AMAPhysicianProfiles. Osteopathic applicants may submit an AOA Profile.

8 | P a g e
Updated 10/03/11
E. Verification of Licensure
See A above. Note: If you were previously licensed in D.C. and that license expired more than five years ago,
you should list your D.C. license in section 5C, but it is not necessary to get verification. If you had a D.C.
license that expired less than five years ago, you should complete the reinstatement application.
F. Examination Scores
You must request your prior certified examination scores from the appropriate authority, if you are applying by
examination or waiver of examination. If you are applying by examination, you must request your examination
score(s) for those sections of the examination that you have passed. If you are applying by waiver of
examination, you must request all of your examination scores. These scores must come to The Office of
Professional Licensing at address directly from the responsible organization. Key examinations and phone
numbers for the appropriate organizations are as follows:
1. FLEX or USMLE: Contact the Federation of State Medical Boards of the United States, Inc. at (817) 868-
4000.
2. NBME: Contact the National Board of Medical Examiners at (215) 590-9500.
3. State examinations: Contact the medical board of the examining state.
4. NBOME: Contact the National Board of Osteopathic Medical Examiners at (703) 635- 9955.
5. LMCC: Contact the Medical Council of Canada at (613) 521- 6012.
G. Undergraduate and Medical School Transcripts
Certified transcripts must be from the appropriate educational institution. Transcripts may be sent directly to
the Board or submitted with your application in a sealed envelope from the institution. Note that if you
transcript or any other document submitted in support of your application is in a language other than English,
you must provide a certified translation. Foreign transcripts do not need to be in sealed envelopes.
H. District of Columbia Computer-Based Testing USMLE Step III Candidate Examination Fee
Form
Send this form with the examination fee (See FSMB application.) at the address shown on the form. The
check should be made payable to USMLE per the instructions on the form.
I. Applications and License Fees
You must pay the application and license fee by a single check or money order. It is recommended that you
pay by check, so that you have ready proof of payment. Checks should be made payable to "DC Treasurer" Do
NOT send cash. Please print your name on your check, if it is not preprinted. The application portion of the fee
is NOT refundable. The license fee portion of the payment is refundable in the event of final denial of a license
or a request from the applicant to close the application. In the latter event, you will have to file all documents
again, should you subsequently decide to apply for licensure. It will take approximately six (6) weeks after
denial or withdrawal for you to receive your refund. For your information, the application and license fee
portions of each application method are listed below:

9 | P a g e
Updated 10/03/11
Total Fee
Examination $288.00
Re-examination $85.00
Licensed by Exam $805.00
Eminence 1 $805.00
Eminence 2 $2000.00
DC Medical licenses expire on December 31 of even numbered years. Your initial license will be valid for the
balance of the current renewal cycle. You will be mailed a renewal notice (to your address of record)
approximately three (3) months before the expiration of your license. Upon completion of the renewal
questionnaire and payment of the renewal fee, your license will be renewed for a two-year period. You should
know that you are required by regulation to report all changes of your business or residence address to the
Board within thirty days of moving. The Board will update the address change in your database record.
Requests for address change should be made via letter. Send the letter to the Board at the address on page 1.
Without an updated address, you will not receive your renewal notice.
J. ECFMG Certificate
Educational Council for Foreign Medical Graduate Certificates may be requested by calling the
Council by phone at (215) 386-5900 and by fax at (215) 386-9196.
K. Fifth Pathway Program Certificates/ FMGEMS Certificates
Fifth Pathway Program Certificates and Foreign Medical Graduate Examination in Medical Science
certificates may be requested from the Education Council for Medical Graduates. They may be reached at the
number shown above.
COMPLETING THE LICENSE APPLICATION
SECTION 1A. TYPE OF LICENSE
a. There are two types of licenses of which may apply. Check the box next to the license description.
SECTION 1B. BASIS OF APPLICATION
a. Check the box next to the basis by which you are applying. To make sure that you select the correct basis of
application, please Review “Methods of Licensure and Qualifications” listed on page 2. It is recommended that
you pay by check, so that you have ready proof of payment. Checks or money orders should be made payable to
DC Treasurer and submitted with your application packet. Do NOT send cash. Please print your name on your
check, if it is not pre-printed. Please note that application and processing fees, once submitted, are non-
refundable after 120 business days.
The license fee portion of the payment may be refundable in the event of final denial of a license or a request from
an applicant to close the application request. In the latter event, you will have to file all documents again, should
you subsequently decide to apply for licensure. It will take approximately six (6) weeks after denial or withdrawal
for you to receive your refund. For your information, the application and license fee total are listed on the
application.

10 | P a g e
Updated 10/03/11
b. *The Total Due amount is the fee that must be paid for your DC license to be processed. Your new license
application fee includes one new license print showing the new effective date and expiration date. A charge of
$65.00 will be imposed for dishonored checks (Public Law 89-208).
SECTIONS 2A. APPLICANT NAME/DEMOGRAPHIC INFORMATION
Enter your legal name exactly as it should appear on the license. The Child Support and Welfare Reform
Compliance Act of 2000, Act 13-559, requires that the Department of Health now collect and maintain social
security numbers for all licensees. Your social security number will not be made available to the public, but if not
provided; your application will be returned to you for completion. All applicants must be at least 18 years of age.
If your name has changed at any point since you first attended college or university, you must provide a copy of a
legal name change document for EACH time that is has changed. Acceptable documents are marriage certificates,
divorce decrees or court orders.
SECTIONS 2B. OTHER NAMES USED
If your name has changed at any point since you first registered with the American Medical Association, taken any
exams or attended a college/university, please note below in order for us to correctly file your supplemental
documents with your application.
SECTION 3A. PREFERRED MAILING ADDRESS
Place an “X” in the appropriate box to indicate your preferred mailing address. This will be the address to which
all future licensing documents will be mailed. A P.O. Box may not be used for an address. Please provide a
street address.
SECTIONS 3B &C. HOME ADDRESS/BUSINESS ADDRESS
Include both your home and business addresses in the sections provided. A P.O. Box may not be used for an
address. Please provide a street address.
SECTION 4A. PROFESSIONAL SCHOOLS ATTENDED
List post secondary schools attended, prior to and including medical/professional schools. List schools that you
have attended in reverse chronological order, beginning with the most recent at the top.
All applicants: Certified transcripts must be from the appropriate educational institution. Transcripts may be sent
directly to the Board or submitted with your application in a sealed envelope from the institution. Note that if your
transcript or any other document submitted in support of your application is in a language other than English, you
must provide a certified translation. Foreign transcripts do not need to be in sealed envelopes.
SECTION 4B. MEDICAL TRAINING AND MEDICAL PRACTICE
List experience covering the five (5) year period prior to the submission of the application and all internship,
residency, and fellowship training. Include letters from employing facilities and training programs on letter head,
including your start and end date. List experience in reverse chronological order, beginning with the most recent at
the top. Note: If "OTHER" description is selected, please attach a typed explanation to this form. If you were
11 | P a g e
Updated 10/03/11
unemployed or self-employed for any period of three months or more please include a statement to that effect on a
separate sheet of paper.
SECTION 4C. MEDICAL LICENSES IN OTHER STATES/JURISDICTIONS
List all states and jurisdictions in which you have ever held a medical license. You must request verification of
licensure for all of these licenses, past and/or present. It is not necessary to get verifications of training licenses.
SECTION 5A. PRACTICE TIME IN THE DISTRICT
Please indicate if you practice in the District and list the type of medical practice. List the amount of time you
spend practicing in the District and if you plan on practicing in Maryland or Virginia.
SECTION 5B. SPECIALTIES
If your practice is limited to a specialty, please indicate the code from the specialty list below. If you are certified
by the “American Board of” any specialty, please indicate the code form the specialty list below.
SPECIALTY CODE
AC Academic Medicine
ADM Administrative Medicine
AI Allergy & Immunology
AN Anesthesiology
DE Dermatology
EM Emergency Medicine
FM Family Medicine
IN Internal Medicine (General)
IN Internal Medicine
IN/CA Cardiology
IN/EN Endocrinology
IN/GI Gastroenterology
IN/HEM Hematology
IN/ID Infectious Disease
IN/NEP Nephrology
IN/NEU Neurology
IN/ONC Oncology
IN/PCC Pulmonary Critical
Care
IN/PUD Pulmonary Disease
IN/RH Rheumatology
MG Medical Genetics
NU Nuclear Medicine
OB Obstetrics & Gynecology
OC Occupational Health
OP Ophthalmology
OMT Osteopathic Manipulative
Treatment
ENT Otolaryngology
PA Pathology
PED Pediatrics (General)
PED Pediatrics
PED/AD Adolescent Medicine
PED/CA Cardiology
PED/EN Endocrinology
PED/GI Gastroenterology
PED/HEM Hematology
PED/NEO Neonatology
PED/NEP Nephrology
PED/NEU Neurology
PED/ONC Oncology
PED/PCC Pulmonary Critical
Care
PED/PUD Pulmonary Disease
PED/RH Rheumatology
PMR Physical Medicine &
Rehabilitation
PR Preventive Medicine/ Public Health
PSY Psychiatry
RA Radiology
REM Research Medicine
SU Surgery (General)
SU Surgery
SU/BT Burn/Trauma
SU/CS Cardiac Surgery
SU/CO Colon & Rectal Surgery
SU/GE General Surgery
SU/NE Neurological Surgery
SU/OR Orthopedic Surgery
SU/PL Plastic Surgery
SU/TH Thoracic Surgery
SU/TP Transplant
SU/UR Urology
SU/VA Vascular
Other:________

12 | P a g e
Updated 10/03/11
SECTION 5C. SCREENING QUESTIONS
If you answer “Yes” to questions A through O, then please provide a complete explanation on a separate sheet of
paper. If more space is required to fully answer questions, attach additional sheets with typed responses. False or
misleading statements will be cause for disciplinary action and could be cause for criminal prosecution pursuant to
DC Code 22-2514.
SECTION 7B. LICENSEE AFFIDAVIT
By signing the application you are attesting under penalty of perjury that all information and attached documents
are true to the best of your knowledge.
ADDITIONAL APPLICATION FORMS
If you need additional copies of this application package you may visit HPLA’s website at
http://www.hpla.doh.dc.gov/bomed or call HPLA’s Customer Service number at 1-877-672-2174.
The forms that make up this package are:
Medicine & Osteopathy, New License Application
Medicine & Osteopathy, New License Application
Chapter 46 Medicine, Municipal Regulations
Examination and Board Action History Report (EBAHR)
Character Reference Form
American Medical Association (AMA) Physician Profile Form
Computer-Based Testing USMLE Step III Candidate Examination Fee Form /
Application and Instructions
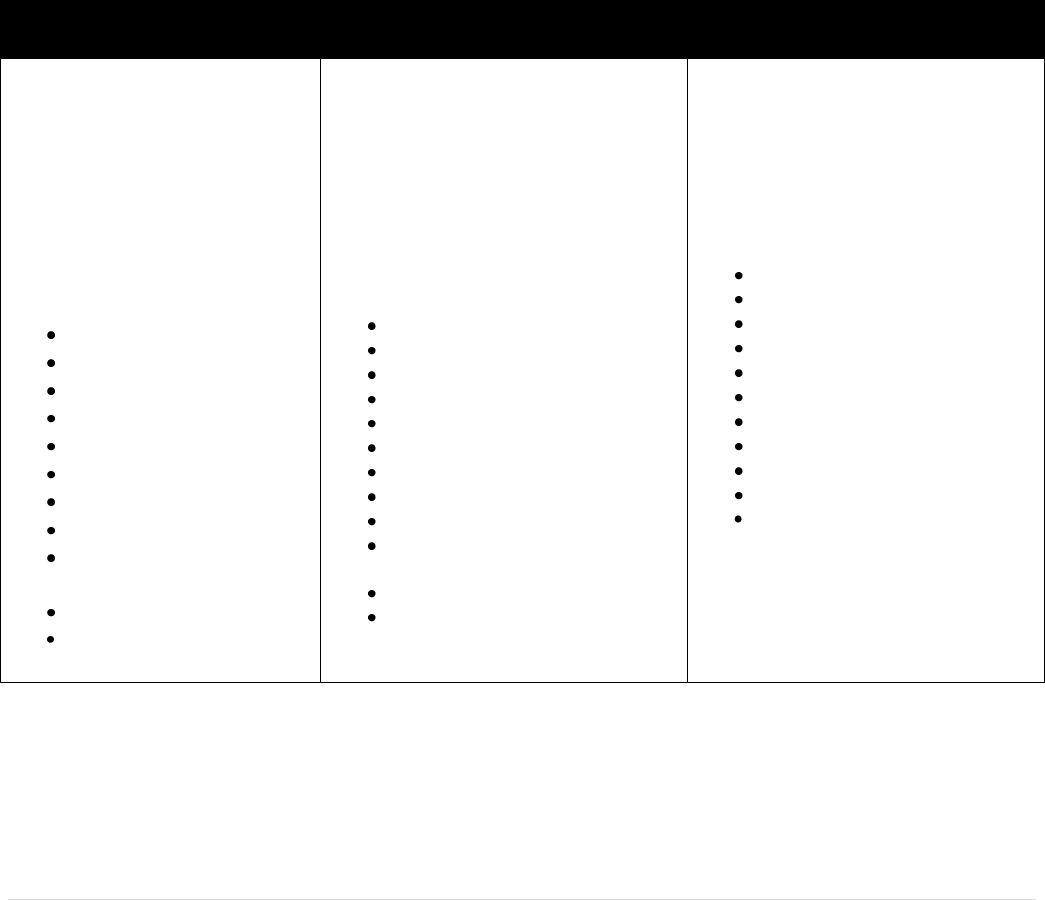
SUMMARY OF LICENSURE REQUIREMENTS
The following chart shows the licensure submission requirements for all application methods. The law
governing medicine licensure in the District of Columbia is D. C. Law 6-99, the Health Occupations
Revision Act of 1985.The regulations governing medicine are included in DC Municipal Regulations
Title 17, Chapters 46. Any conflict between these instructions and the law and regulations is inadvertent.
The law and the regulations take precedence in the event of any inadvertent conflict. Please contact the
Department of Health/Board of Medicine if you have any questions regarding the interpretation of these
laws as they pertain to your particular situation.

13 | P a g e
Updated 10/03/11
DC BOARD OF MEDICINE APPLICATION SUBMISSION REQUIREMENTS
X = Required
O = Not Required
* Subject to change; payable to FSMB - see FSMB application for fees.
Note: All applicants must document name changes if applicable. Check or money order MUST be made payable to
DC Treasurer.
EXAMINATION
RE-EXAM
WAIVER OF EXAMINATION
EMINENCE 1
EMINENCE 2
DOCUMENTS
(USMLE)
(USMLE)
USMLE/FLEX/NBME/NBOME/
LMCC/State Constructed
(DCMR 17 Sec. 4608.1)
DC Act 11-26
LTD. LIC.
Application for DC License
X
X
X
X
X
Two (2) Passport Type
Photos
X
O
X
X
X
Character Reference Form(s)
X
O
X
X
X
Documentation of all training
and past 5 year work
experience
X
O
X
X
X
AMA Profile
X
O
X
X
X
Verification of Licensure
O
O
X
X
X
Examination Scores
(Steps 1 & 2)
O
X
O
O
Undergraduate Transcript
X
O
X
X
X
Medical School Transcript
X
O
X
X
x
CBT USMLE Step III
Examination Fee Form
X
X
O
O
O
Application and License Fees
$288
$85
$805
$805
$2000
Examination Fee
*
*
O
O
O
Foreign Trained Physicians
add: ECFMG Certificate
X
O
X
X
X
Fifth Pathway Applicants
add: Fifth Pathway Program
Certificate
X
O
X
X
X
FMGEMS Certificate
X
O
X
X
X
Eminence Applicants only
add: Curriculum Vitae
O
O
O
X
X
List of Publications
O
O
O
X
X
List of Honors and Awards
O
O
O
X
X
Letter of Recommendation
from Institution Head
O
O
O
O
X
HI Visa Status Certificate
O
O
O
O
X
5 Letters from Renowned
American Specialist in Field
O
O
O
O
X
Letter of Acceptance from
Sponsoring Institution
O
O
O
O
X
