Journal
of
Neurology,
Neurosurgery,
and
Psychiatry,
1974,
37,
900-906
An
analysis
of
myotonia
in
paramyotonia
congenital
DAVID
BURKE,
NEVELL
F.
SKUSE,
AND
A.
KEITH
LETHLEAN
From
the
Unit
of
Clinical
Neurophysiology,
Division
of
Neurology,
Prince
Henry
Hospital,
Little
Bay,
N.S.
W.
2036,
Australia
SYNOPSIS
In
two
subjects
with
paramyotonia
congenita
myotonic
delay
in
muscle
relaxation,
recorded
electromyographically
and
with
a
displacement
transducer,
was
found
to
increase
with
repeated
forceful
contractions.
Myotonia
was
elicited
readily
in
warm
temperatures,
was
initially
aggravated
by
cooling,
but
was
invariably
lost
as
muscle
fatigue
developed.
The
EMG
evidence
of
myotonia
usually
subsided
before
complete
muscle
relaxation
had
occurred,
suggesting
that
a
defect
of
the
contractile
mechanism
was
present
over
and
above
any
defect
at
membrane
level.
The
non-dystrophic
forms
of
myotonia
may
be
distinguished
one
from
the
other
on
the
basis
of
heredity
and
the
patterns
of
myotonia
and
of
weakness.
Paramyotonia
congenita
is
said
to
be
characterized
by
'paradoxical'
myotonia
which
is
accentuated
by
repetitive
muscle
contraction,
and
by
extreme
sensitivity
to
cooling,
which
aggravates
the
myotonia
and
the
muscle
weak-
ness.
But
paradoxical
myotonia
has
not
been
a
uniform
finding
in
all
patients
with
otherwise
classical
paramyotonia,
and
it
has
even
been
reported
to
be
present
in
some
but
absent
in
other
members
of
the
same
family.
While
these
discrepancies
may
arise
in
part
from
differing
degrees
of
severity
in
different
patients
examined
under
different
circumstances,
this
explanation
is
unsatisfactory
if
the
paradoxical
nature
of
the
myotonia
is
to
be
used
as
a
feature
distinguishing
paramyotonia
congenita
from
the
dominant
and
recessive
forms
of
myotonia
congenita.
This
paper
analyses
aspects
of
myotonia
in
two
subjects
with
paramyotonia
congenita
with
particular
reference
to
the
responses
to
repeated
muscle
contraction
and
to
muscle
cooling.
Muscular
weakness
has
been
analysed
in
a
companion
paper
(Burke
et
al.,
1974b).
METHODS
Data
were
obtained
from
13
experimental
sessions
in
a
25
year
old
subject
with
classical
paramyotonia
congenita
and
were
confirmed
in
a
further
experi-
1
Some
of
these
findings
were
reported
to
the
1974
meeting
of
the
Australian
Association
of
Neurologists.
mental
session
in
a
similarly
afflicted
19
year
old
brother.
These
sessions
provided
data
for
this
paper
and
a
companion
paper
on
muscular
weakness
(Burke
et
al.,
1974b).
Clinically
the
myotonia
in
both
subjects
was
'paradoxical'.
Most
experiments
were
performed
on
the
abductor
digiti
minimi
muscle
(ADM)
but
one
experimental
session
was
devoted
to
the
triceps
surae,
from
which
similar
data
were
obtained.
In
these
two
muscles,
voluntary
and
electrically-induced
contractions
were
studied
under
isometric
and
isotonic
conditions.
In
four
experiments
voluntary
contractions
of
the
flexor
digitorum
profundus
(FDP)
were
studied
under
iso-
tonic
conditions.
Isometric
contractions
of
ADM
and
of
triceps
surae
were
elicited
as
described
by
Burke
et
al.
(1974a,
b).
The
displacement
produced
by
iso-
tonic
contractions
was
recorded
by
a
Burdick
FM.
1
Photomotograph,
positioned
so
that
the
resulting
movement
interrupted
the
light
beam
from
a
photo-
electric
cell.
For
ADM
the
hand
was
fixed
in
a
frame
with
a
horizontal
bar
which
prevented
finger
flexion.
The
fifth
finger
fitted
into
a
retaining
ring
which
could
move
freely
in
the
horizontal
plane
so
that
abduction
movements
were
not
impeded.
A
light-
weight
spring
of
low
tensile
strength
was
attached
to
the
retaining
ring
to
return
the
abducted
finger
to
the
control
position
once
contraction
had
subsided.
For
triceps
surae
the
patient
lay
prone
so
that
the
plantar
flexion
movement
was
performed
against
gravity
which
returned
the
foot
to
the
control
position
as
the
contraction
subsided.
For
FDP
finger
flexion
was
opposed
by
a
light-weight
spring
which
was
adjusted
so
that
it
was
capable
of
extending
the
fingers
when
they
were
completely
relaxed.
The
electromyogram
(EMG)
was
recorded
by
sur-
face
electrodes
taped
to
the
bellies
of
the
muscles.
00

An
analysis
of
myotonia
in
paramyotonia
congenita
For
FDP
and
for
some
experiments
on
ADM
intra-
muscular
EMG
was
recorded
using
a
concentric
needle
electrode
(Disa
9013KO512).
Experiments
were
carried
out
in
a
warm
air-conditioned
labora-
tory.
The
skin
temperature
over
ADM,
triceps
surae,
and
FDP
was
measured
by
an
Ellab
electronic
thermometer
and
was
maintained
at
34-35°C.
The
hand
and
arm
were
cooled
by
packing
a
plastic
bag
containing
ice
around
the
limb.
A
I
come
this
involuntary
stiffness
was
less
than
that
required
if
the
muscle
had
been
allowed
to
shorten
in
an
isotonic
contraction.
ADM,
FDP,
and
abductor
pollicis
brevis
were
sampled
with
concentric
needle
electrodes.
In-
creased
insertional
activity
was
recorded,
with
spontaneous
activity
of
fibrillation
or
positive
sharp
wave
form.
Recurring
volleys
of
sharp
waves
were
seen
to
occur
apparently
spon-
A
B
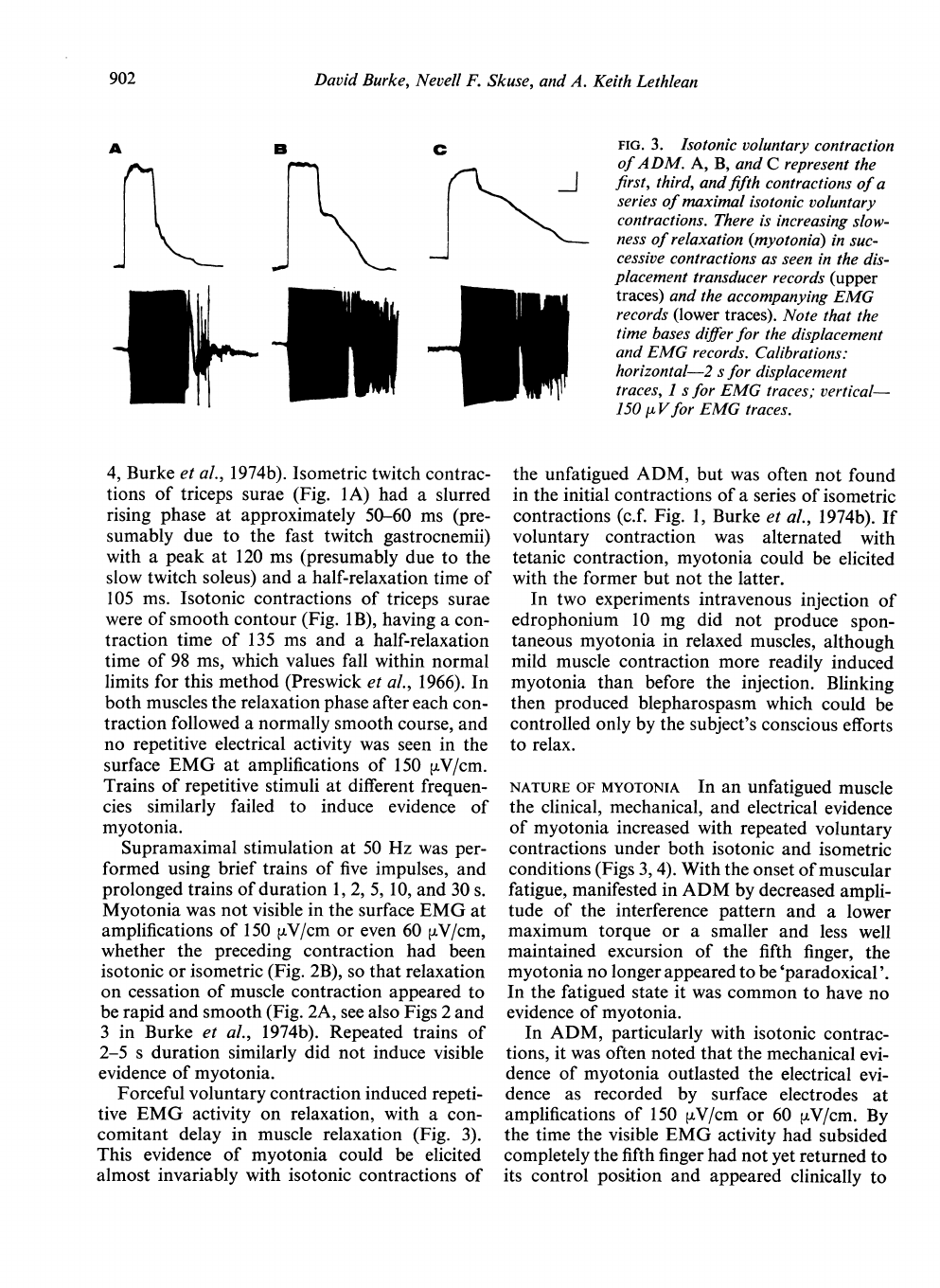
FIG.
1.
Twitch
contractions
of
triceps
surae.
A:
isometric
contraction
of
right
triceps
surae.
B:
isotonic
contraction
of
left
triceps
surae.
Note
the
small
H
wave,
indicated
in
B
by
the
arrow.
Calibrations:
horizontal-50
ms
for
A
and
B;
vertical-9
32
x
10-
3
Nm
for
A,
6
mVfor
A
and
B.
I
FIG.
2.
Isotonic
contraction
of
ADM
induced
by
tetanic
stimulation
at
50
Hz.
A:
time
course
of
con-
traction.
There
is
no
delay
in
relaxation
on
cessation
of
stimulation.
B:
EMG
during
and
after
stimulation.
The
EMG
sweep
was
started
after
tetanization
had
been
in
progress
for
1
s.
No
myotonic
activity
is
seen.
Calibrations:
horizontal-I
s
for
A
and
B;
vertical-
150
puV
for
B.
RESULTS
Clinically,
myotonia
in
the
form
of
a
persistent
failure
of
muscle
relaxation
could
be
readily
elicited
at
surface
temperatures
of
34-35°C.
In
unfatigued
muscle
this
myotonia
became
more
prominent
with
repeated
voluntary
contraction
of
muscle.
Voluntary
isotonic
contraction
appeared
to
induce
myotonia
more
readily
than
voluntary
isometric
contraction
in
which
the
contracting
muscle
was
prevented
from
shorten-
ing.
After
vigorous
isometric
contraction,
re-
moval
of
the
restraint
often
resulted
in
an
abduc-
tion
movement
of
the
fifth
finger
(with
ADM)
or
flexion
of
the
fingers
(with
FDP),
thus
shortening
the
appropriate
muscle.
However
clinically
it
appeared
that
the
force
then
necessary
to
over-
taneously
or
to
be
evoked
by
electrode
move-
ment
or
voluntary
contraction.
Motor
unit
action
potentials
were
within
normal
limits
but
the
interference
pattern
fatigued
rapidly
on
sus-
tained
effort.
Cessation
of
voluntary
contraction
was
followed
by
continued
electrical
activity
in
the
form
of
motor
unit
potentials,
fibrillation
potentials
and
positive
sharp
waves.
ADEQUATE
STIMULUS
FOR
MYOTONIA
Electrically-
induced
contractions
failed
to
provoke
myotonia
in
ADM
and
in
triceps
surae.
In
ADM,
iso-
metric
and
isotonic
twitch
contractions
had
similar
time
courses
contraction
time
63-70
ms,
and
half-relaxation
time
68-80
ms
(c.f.
Fig.
901
David
Burke,
Nevell
F.
Skuse,
and
A.
Keith
Lethlean
A
B
re
m~~~~-
C
I
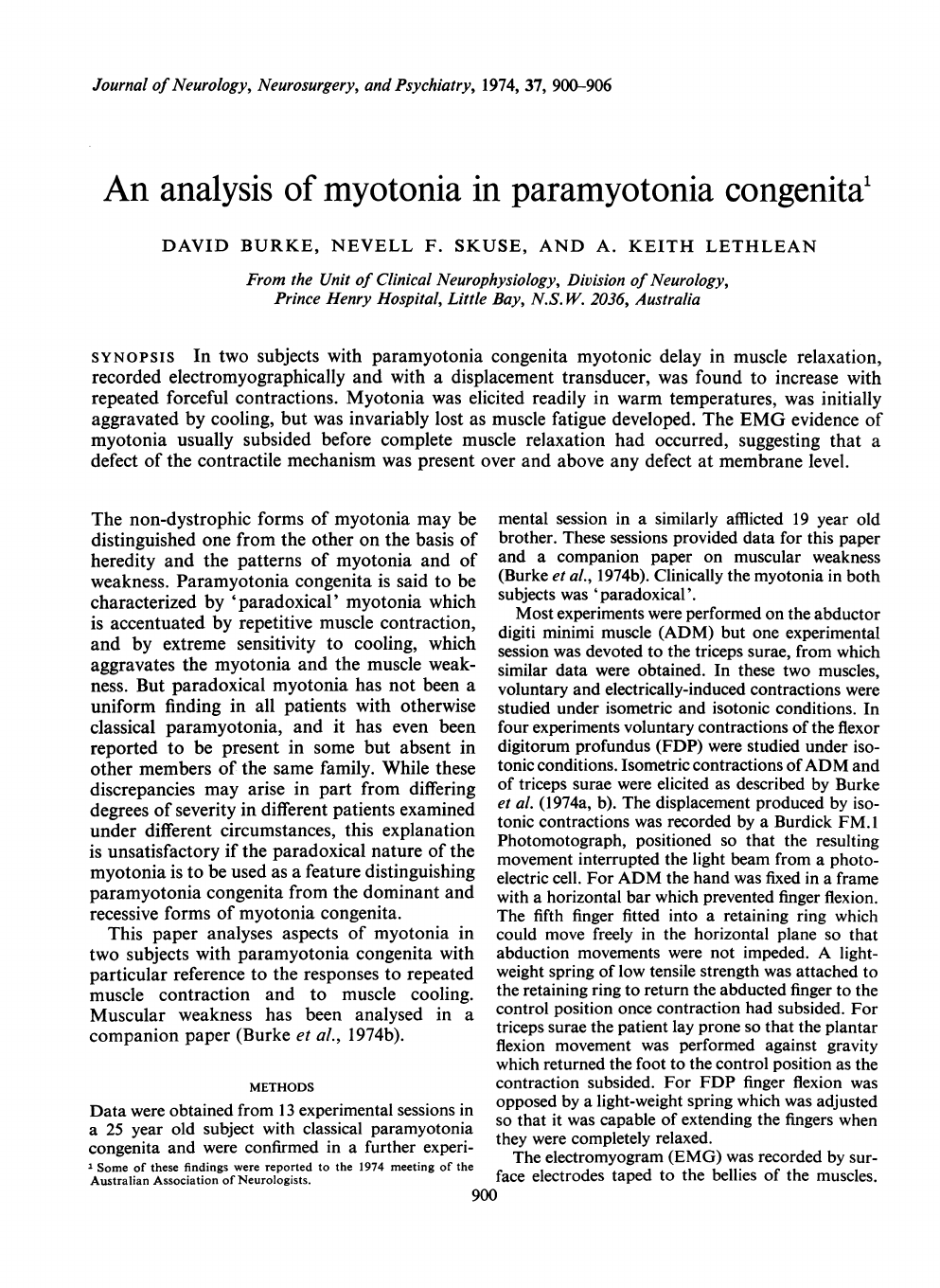
FIG.
3.
Isotonic
voluntary
contraction
of
ADM.
A,
B,
and
C
represent
the
first,
third,
and
fifth
contractions
of
a
series
of
maximal
isotonic
voluntary
contractions.
There
is
increasing
slow-
ness
of
relaxation
(myotonia)
in
suc-
cessive
contractions
as
seen
in
the
dis-
placement
transducer
records
(upper
traces)
and
the
accompanying
EMG
records
(lower
traces).
Note
that
the
time
bases
differ
for
the
displacement
and
EMG
records.
Calibrations:
horizontal-2
s
for
displacement
traces,
1
s
for
EMG
traces;
vertical-
150
,u
Vfor
EMG
traces.
4,
Burke
et
al.,
1974b).
Isometric
twitch
contrac-
tions
of
triceps
surae
(Fig.
lA)
had
a
slurred
rising
phase
at
approximately
50-60
ms
(pre-
sumably
due
to
the
fast
twitch
gastrocnemii)
with
a
peak
at
120
ms
(presumably
due
to
the
slow
twitch
soleus)
and
a
half-relaxation
time
of
105
ms.
Isotonic
contractions
of
triceps
surae
were
of
smooth
contour
(Fig.
1
B),
having
a
con-
traction
time
of
135
ms
and
a
half-relaxation
time
of
98
ms,
which
values
fall
within
normal
limits
for
this
method
(Preswick
et
al.,
1966).
In
both
muscles
the
relaxation
phase
after
each
con-
traction
followed
a
normally
smooth
course,
and
no
repetitive
electrical
activity
was
seen
in
the
surface
EMG
at
amplifications
of
150
,uV/cm.
Trains
of
repetitive
stimuli
at
different
frequen-
cies
similarly
failed
to
induce
evidence
of
myotonia.
Supramaximal
stimulation
at
50
Hz
was
per-
formed
using
brief
trains
of
five
impulses,
and
prolonged
trains
of
duration
1,
2,
5,
10,
and
30
s.
Myotonia
was
not
visible
in
the
surface
EMG
at
amplifications
of
150
,V/cm
or
even
60
,V/cm,
whether
the
preceding
contraction
had
been
isotonic
or
isometric
(Fig.
2B),
so
that
relaxation
on
cessation
of
muscle
contraction
appeared
to
be
rapid
and
smooth
(Fig.
2A,
see
also
Figs
2
and
3
in
Burke
et
al.,
1974b).
Repeated
trains
of
2-5
s
duration
similarly
did
not
induce
visible
evidence
of
myotonia.
Forceful
voluntary
contraction
induced
repeti-
tive
EMG
activity
on
relaxation,
with
a
con-
comitant
delay
in
muscle
relaxation
(Fig.
3).
This
evidence
of
myotonia
could
be
elicited
almost
invariably
with
isotonic
contractions
of
the
unfatigued
ADM,
but
was
often
not
found
in
the
initial
contractions
of
a
series
of
isometric
contractions
(c.f.
Fig.
1,
Burke
et
al.,
1974b).
If
voluntary
contraction
was
alternated
with
tetanic
contraction,
myotonia
could
be
elicited
with
the
former
but
not
the
latter.
In
two
experiments
intravenous
injection
of
edrophonium
10
mg
did
not
produce
spon-
taneous
myotonia
in
relaxed
muscles,
although
mild
muscle
contraction
more
readily
induced
myotonia
than
before
the
injection.
Blinking
then
produced
blepharospasm
which
could
be
controlled
only
by
the
subject's
conscious
efforts
to
relax.
NATURE
OF
MYOTONIA
In
an
unfatigued
muscle
the
clinical,
mechanical,
and
electrical
evidence
of
myotonia
increased
with
repeated
voluntary
contractions
under
both
isotonic
and
isometric
conditions
(Figs
3,
4).
With
the
onset
of
muscular
fatigue,
manifested
in
ADM
by
decreased
ampli-
tude
of
the
interference
pattern
and
a
lower
maximum
torque
or
a
smaller
and
less
well
maintained
excursion
of
the
fifth
finger,
the
myotonia
no
longer
appeared
to
be
'paradoxical'.
In
the
fatigued
state
it
was
common
to
have
no
evidence
of
myotonia.
In
ADM,
particularly
with
isotonic
contrac-
tions,
it
was
often
noted
that
the
mechanical
evi-
dence
of
myotonia
outlasted
the
electrical
evi-
dence
as
recorded
by
surface
electrodes
at
amplifications
of
150
MV/cm
or
60
,uV/cm.
By
the
time
the
visible
EMG
activity
had
subsided
completely
the
fifth
finger
had
not
yet
returned
to
its
control
position
and
appeared
clinically
to
902

An
analysis
of
myotonia
in
paramyotonia
congeniita
A
B
FIG.
4.
Isotonic
voluntary
contraction
of
ADM.
Six
successive
isotonic
contractions
have
been
super-
imposed,
the
oscilloscope
trace
being
retriggered
immediately
after
cessation
of
the
previous
sweep.
The
increasing
failure
of
relaxation
is
seen
as
increasing
inability
of
the
trace
to
return
to
base-line
at
the
end
of
voluntary
contraction,
so
that
the
next
contraction
starts
from
an
increasingly
less
relaxed
position.
The
duration
of
maximal
voluntary
contraction
is
6
s,
as
indicated
by
the
bar.
retain
some
stiffness.
Absence
of
EMG
activity
was
confirmed
in
one
experiment
on
ADM
using
a
concentric
needle
electrode.
That
membrane
irritability
as
reflected
in
myotonic
EMG
activity
does
not
fully
explain
the
mechanical
failure
of
relaxation
was
investigated
in
FDP
in
four
experimental
sessions,
using
both
surface
and
needle
electrodes.
With
the
fingers
prevented
from
flexing,
vigorous
(isometric)
contraction
of
FDP
was
followed
by
typical
myotonic
EMG
activity.
Once
the
EMG
activity
(as
recorded
by
the
concentric
needle)
had
subsided,
the
restraint
was
removed
and
immediate
finger
flexion
resulted.
Re-extension
of
the
fingers
under
the
influence
of
the
soft
steel
spring
occurred
slowly
after
some
delay,
even
though
the
spring
had
been
capable
of
extending
the
fingers
prior
to
contraction.
Alternatively,
restraint
was
re-
moved
on
cessation
of
voluntary
contraction,
with
resultant
finger
flexion
which
was
main-
tained
long
after
the
EMG
activity
had
subsided.
The
findings
were
essentially
similar
with
isotonic
contractions
of
FDP,
finger
flexion
being
main-
tained
by
the
myotonic
contraction
on
cessation
FIG.
5.
Isotonic
contraction
of
FDP.
A:
displace-
ment
record.
Initially
the
fingers
are
maintained
in
an
extended
position
by
the
mild
steel
spring
but
are
then
flexed
in
a
maximal
voluntary
contraction
of
FDP
which
is
maintained
for
S
s,
ending
at
the
arrow.
On
cessation
of
voluntary
contraction
the
fingers
remain
flexed,
extending
only
partially
and
then
very
slowly
under
the
influence
of
the
spring.
The
oscilloscope
trace
was
retriggered
twice
to
show
the
persistent
failure
of
relaxation.
B:
EMG
recorded
with
a
con-
centric
needle
electrode
during
the
second
of
the
above
oscilloscope
sweeps
showing
only
very
low
voltage
EMG
activity
(less
than
40
,uV,
mostly
of
positive
sharp
wave
form).
Failure
of
relaxation
out-
lasts
significant
EMG
activity.
Calibrations:
horizon-
tal-S
s
for
A,
I
s
for
B;
vertical-150
,u
Vfor
B.
of
voluntary
contraction,
and
re-extension
occur-
ring
slowly
under
the
influence
of
the
spring
long
after
the
subsidence
of
significant
EMG
activity
(as
recorded
by
the
needle
electrode).
Figure
5
illustrates
this
phenomenon.
Isotonic
voluntary
contraction
starts
from
a
relaxed
position
and
ceases
after
5
s
at
the
arrow.
Myotonic
EMG
activity
decreased
over
the
succeeding
12
s,
and
thereafter
only
an
occasional
potential
of
very
low
voltage
was
recorded
(Fig.
5B).
The
fingers
remain
partially
flexed
for
more
than
100
s,
flexion
being
maintained
against
a
spring
which
originally
had
been
capable
of
holding
the
fingers
at
the
starting
position.
During
this
phase
of
'non-electrical'
muscle
stiffness
the
fingers
could
be
passively
re-extended
by
the
examiner.
Following
partial
extension
the
fingers
were
capable
of
maintaining
the
new
position
to
which
they
had
been
moved
for
some
time,
per-
903
l

David
Burke,
Nevell
F.
Skuse,
and
A.
Keith
Lethlean
haps
flexing
up
slightly
or
extending
slightly
with
the
passage
of
time.
If
the
fingers
were
extended
to
the
control
position
and
immediately
released
they
commonly
flexed
again
without
significant
audible
or
visible
EMG
activity.
The
distinction
between
the
electrical
and
mechanical
components
of
myotonia
could
be
appreciated
in
the
fatigued
state.
Clinical
myo-
tonia
decreased
during
muscle
fatigue,
at
times
even
disappearing,
but
the
EMG
evidence
of
myotonia
appeared
to
be
more
affected
than
the
mechanical
delay
in
relaxation.
On
a
number
of
occasions
the
fatigued
muscle
demonstrated
what
appeared
clinically
to
be
myotonia
but
this
was
not
accompanied
by
EMG
activity.
Studies
with
the
needle
electrode
indicated
that
as
the
muscle
fatigued
the
EMG
signs
of
hyperexcit-
ability
became
less
prominent
and
ultimately
disappeared.
EFFECT
OF
COOLING
Muscle
cooling
did
not
provoke
spontaneous
EMG
activity
and
did
not
produce
a
spontaneous
muscle
contraction.
In
four
experiments
in
the
two
subjects
cooling
resulted in
a
profound
prolongation
of
the
isometric
twitch
times
of
ADM,
the
changes
being
more
prominent
for
the
half-relaxation
time
than
for
the
contraction
time
(Fig.
6;
com-
pare
with
Fig.
4,
Burke
et
al.,
1974b).
Surface
temperature
decreased
from
34-35°
to
between
21°C
and
28°C
in
different
experiments.
The
rate
of
increase
of
half-relaxation
time,
20-28,/
(mean
23.5%)
for
each
°C
fall
in
temperature,
greatly
exceeded
that
of
the
contraction
time,
l
l%-12.5%
(mean
115%)
per
°C
fall
in
tem-
FIG.
6.
Effect
of
cooling
on
isometric
twitch
times
of
A
DM.
Surface
temperature
measured
over
A
DM
was
decreased
to
21°C,
resulting
in
prolongation
of
the
contraction
time
to
150
ms
and
of
the
half-relaxation
time
to
270
ms
(compare
with
Fig.
5,
Burke
et
al.,
1974b).
Calibrations:
horizontal-100
ms;
vertical-
466x
lO5
Nm.
perature,
so
that
the
ratio
of
half-relaxation
time
to
contraction
time
increased
to
1
9
at
21°C.
Since
changes
in
skin
temperature
probably
exceed
changes
in
muscle
temperature,
these
figures
probably
underestimate
the
effects
of
cooling.
The
evoked
muscle
action
potential
remained
a
discrete
potential.
There
was
no
evi-
dence
of
repetitive
EMG
activity
with
surface
electrodes
at
gains
of
150
MV/cm,
so
that
the
marked
prolongation
of
half-relaxation
time
cannot
be
attributed
to
electrical
myotonia.
During
cooling,
repetitive
electrical
activa-
tion,
even
tetanization,
of
ADM
failed
to
pro-
voke
mechanical
or
EMG
evidence
of
myo-
tonia.
With
voluntary
contraction,
muscle
cool-
ing
appeared
initially
to
aggravate
both
the
electrical
and
the
mechanical
evidence
of
myo-
tonia
but,
since
it
also
aggravated
the
fatigue
process,
this
effect
could
not
be
assessed
ade-
quately.
However,
as
the
fatiguing
process
became
dominant
the
EMG
evidence
of
hyper-
excitability
disappeared,
so
that
it
was
again
possible
to
record
a
greatly
delayed
relaxation
of
the
cooled
fatigued
ADM
in
the
absence
of
electrical
activity.
DISCUSSION
In
the
two
subjects
with
paramyotonia
congenita,
the
adequate
stimulus
for
myotonia
appears
to
be
vigorous
voluntary
contraction,
preferably
repeated
voluntary
contraction,
and
isotonic
rather
than
isometric
voluntary
contraction.
That
myotonia
could
not
be
demonstrated
after
electrically
induced
contraction
was
unexpected
and
cannot
be
adequately
explained.
Possibly
the
synchronized
contraction
of
motor
units
in
a
tetanus
is
a
less
effective
stimulus
than
the
asynchronous
discharge
of
motor
units
produced
by
voluntary
contraction.
Although
systematic
observations
were
not
made,
voluntary
contraction
of
ADM
produced
in
both
control
and
experimental
subjects
a
greater
torque
than
tetanic
contraction,
a
finding
at
variance
with
that
of
Merton
(1954)
who
studied
adductor
pollicis.
The
torque
produced
by
voluntary
abduction
of
digit
5
depends
not
only
on
ADM
but
also
on
the
flexor
carpi
ulnaris
which
stabilizes
the
pisiform
bone,
thus
contributing
indirectly
to
the
recorded
torque.
Differences
in
the
strength
of
voluntary
and
904

An
anialysis
of
myotonia
in
paramyotonia
congenita
tetanic
contraction
therefore
do
not
explain
the
greater
efficacy
of
voluntary
contraction
in
pro-
ducing
myotonia
in
ADM.
Certainly
myotonia
became
more
difficult
to
elicit
as
the
muscle
fatigued:
perhaps
this
explains
why
some
authors
have
reported
that
myotonia
is
not
para-
doxical
in
some
patients
with
paramyotonia.
In
any
event,
the
force
produced
by
muscle
con-
traction
cannot
be
the
major
determinant
of
myotonia
because
contractile
force
increases
as
muscle
length
increases
(Joyce
et
al.,
1969),
so
that
isometric
contraction
should
have
produced
myotonia
more
readily
than
isotonic
contraction.
During
maximal
voluntary
contraction
motor
units
commonly
discharge
at
frequencies
of
60-
80/s,
and
some
exceed
100/s
(Marsden
et
al.,
1971),
although
such
rates
cannot
be
sustained
(Tanji
and
Kato,
1972;
Hannerz,
1973).
Pre-
sumably,
synchronized
firing
of
motor
units
at
50/s
as
in
a
tetanus
is
a
relatively
ineffective
stimulus
for
myotonia.
In
both
experimental
subjects
the
delayed
muscular
relaxation
which
produces
clinical
myotonia
appeared
to
have
two
components.
The
EMG
signs
of
myotonia
are
similar
to
those
found
in
other
myotonic
disorders.
A
membrane
phenomenon
has
been
implicated
as
the
cause
of
this
'electrical
myotonia'
and,
indeed,
experi-
mental
myotonia
can
be
produced
by
agents
which
interfere
with
muscle
cell
membrane
stability-for
example,
20,
25-diazacholesterol
(Bryant,
1973).
In
paramyotonia
muscle
fatigue
appears
to
arise
from
a
progressive
decrease
in
excitability
of
the
muscle
cell
membrane
(Burke
et
al.,
1974b),
and,
not
surprisingly
therefore,
the
EMG
signs
of
myotonia
decrease
as
fatigue
pro-
gresses.
The
loss
of
'electrical
myotonia'
with
fatigue
of
muscle
explains
the
EMG
silence
found
in
paramyotonia
after
cooling
because
cooling
greatly
aggravates
the
fatiguing
process
(Burke
et
al.,
1974b).
That
the
inability
to
relax
after
a
vigorous
contraction
outlasts
the
classical
EMG
signs
of
myotonia
suggests
that,
while
there
may
be
a
membrane
defect,
an
additional
mechanical
factor
contributes
to
clinical
myo-
tonia.
A
primary
defect
of
the
ability
to
relax
of
the
contractile
mechanism
within
the
muscle
cell
is
therefore
suggested.
A
similar
conclusion
was
reached
by
Haynes
and
Thrush
(1972)
based
on
in
vitro
studies
of
membrane
phenomena:
the
myotonia
itself
is
possibly
a
direct
effect
of
the
disease
upon
the
contractile
elements
of
the
muscle'.
If
clinical
myotonia
has
two
components,
electrical
and
mechanical,
due
to
two
defects,
membrane
and
contractile,
an
hypothesis
can
be
advanced
to
explain
why
isotonic
contractions
appear
to
produce
clinical
myotonia
more
readily
than
isometric
contractions.
With
iso-
metric
contraction
realignment
of
contractile
filaments
would
be
limited,
but
when
significant
shortening
occurs,
as
in
an
isotonic
contraction,
complete
realignment
of
contractile
filaments
must
take
place.
As
a
result,
the
mechanical
component
of
myotonia,
that
due
to
a
defect
in
the
ability
of
contractile
elements
to
'relax',
would
be
more
prominent
in
isotonic
contrac-
tions.
The
effect
of
muscle
cooling
on
the
twitch
times
of
ADM
provides
additional
support
for
the
presence
of
a
mechanical
factor
in
myo-
tonia.
There
are
few
observations
on
the
effect
of
cooling
on
twitch
characteristics
of
human
muscle.
In
excised
human
muscle
at
20°C
Brust
and
Cosla
(1967)
reported
contraction
times
of
188-3
ms
and
3812
ms
and
half
relaxation
times
of
252-2
ms
and
597
4
ms
for
groups
of
muscles
classified
respectively
as
fast
and
slow.
Buchthal
and
Schmalbruch
(1970)
found
in
intact
human
muscle
that
contraction
times
of
fast
fibres
in-
creased
by
up
to
10%
per
°C
and
of
slow
fibres
by
up
to
700
per
'C.
It
is
difficult
to
compare
these
data
with
those
of
the
present
study,
since
the
latter
were
obtained
using
surface
tempera-
ture
measurements
and
therefore
probably
underestimate
the
rate
of
increase
in
twitch
times.
Nevertheless,
the
rate
of
increase
in
con-
traction
time
was
of
a
similar
order
of
magnitude
to
that
reported
by
Buchthal
and
Schmalbruch
(1970),
who
unfortunately
did
not
report
values
for
the
half-relaxation
time.
From
the
data
of
Brust
and
Cosla
(1967)
the
ratio
of
half-relaxa-
tion
time
to
contraction
time
at
20°C
is
1-34
for
fast
muscles
and
1
57
for
slow
muscles,
figures
which
are
significantly
less
than
the
ratio
of
1.9
found
in
the
present
study,
even
though
the
effective
temperature
was
probably
significantly
higher
in
the
present
study.
These
data
suggest
that,
although
the
changes
in
contraction
time
induced
by
cooling
may
be
acceptable
as
within
normal
limits,
the
increase
in
half-relaxation
time
is
probably
excessive.
The
findings
are
905

David
Burke,
Nevell
F.
Skuse,
and
A.
Keith
Lethlean
therefore
consistent
with
a
defect
of
the
contrac-
tile
mechanism
within
the
muscle
cell,
a
defect
demonstrable
at
room
temperature
only
after
vigorous
voluntary
contraction,
but
more
readily
demonstrated
in
cooler
circumstances.
As
with
the
fatiguing
process
(Burke
et
al.,
1974b),
cooling
appears
to
lower
the
threshold
for
the
demonstration
of
the
muscular
defect-it
does
not
appear
to
play
a
primary
pathogenic
role.
The
suggestion
that
the
myotonia
of
para-
myotonia
congenita
has
two
components,
a
membrane
('electrical')
component
and
an
internal
contractile
('mechanical')
component,
raises
therapeutic
implications.
It
is
not
sur-
prising
that
drugs
which
stabilize
cell
membrane
function
often
prove
disappointing
clinically
in
the
treatment
of
paramyotonia,
since
such
agents
would
prove
beneficial
only
if
membrane
phenomena
contribute
significantly
to
the
failure
of
relaxation.
Indeed,
it
is
quite
conceivable
that,
as
far
as
the
myotonia
is
concerned,
the
electrical
phenomena
are
of
little
clinical
relevance
apart
from
providing
an
important
diagnostic
sign
for
the
electromyographer.
SUMMARY
Myotonia
was
studied
in
two
brothers
with
paramyotonia
congenita.
In
non-fatigued
muscle,
myotonia
could
be
elicited
at
room
temperature
by
vigorous
voluntary
contraction,
more
readily
under
isotonic
than
isometric
con-
ditions.
With
repeated
voluntary
contractions
the
myotonia
increased
in
successive
contractions
('paradoxical
myotonia')
until
the
development
of
muscle
fatigue
resulted
in
its
disappearance.
Electrical
stimulation,
including
tetanization
at
50
Hz,
failed
to
elicit
myotonia.
It
was
frequently
noted
that
the
EMG
evidence
of
myotonia
subsided
before
the
contracting
muscle
had
relaxed
completely.
Muscle
cooling
appeared
initially
to
aggravate
the
myotonia
but,
since
it
also
aggravated
the
fatigue
process,
evidence
of
myotonia
sub-
sequently
disappeared.
Isometric
twitch
times
of
the
abductor
digiti
minimi
were
prolonged
by
muscle
cooling,
the
half-relaxation
time
being
affected
more
than
the
contraction
time.
No
repetitive
EMG
activity
accompanied
these
changes.
These
results
are
best
explained
by
postulat-
ing
that
in
paramyotonia
congenita
the
myotonic
failure
of
relaxation
has
two
components-
excessive
irritability
of
the
muscle
cell
membrane
which
produces
the
classical
EMG
features
of
myotonia,
and
a
defect
of
the
ability
of
the
contractile
mechanism
within
the
muscle
cell
to
relax
after
contraction.
This
conclusion
explains
the
limited
therapeutic
efficacy
of
drugs
which
act
by
stabilizing
membranes.
The
authors
are
grateful
to
Mr
Peter
van
Megen
and
A.C.I.,
Ltd,
without
whose
generous
assistance
these
studies
could
not
have
been
performed,
and
to
Professor
J.
W.
Lance
for
advice
in
the
preparation
of
this
report.
Illustrations
were
photographed
by
the
Department
of
Medical
Illustration,
University
of
N.S.W.
REFERENCES
Brust,
M.,
and
Cosla,
H.
W.
(1967).
Contractility
of
isolated
human
skeletal
muscle.
Archives
of
Physical
Medicine
and
Rehabilitation,
48,
543-555.
Bryant,
S.
H.
(1973).
The
electrophysiology
of
myotonia,
with
a
review
of
congenital
myotonia
of
goats.
In
New
Developments
in
Electromyography
and
Clinical
Neuro-
physiology,
vol.
1,
pp.
420-450.
Edited
by
J.
E.
Desmedt.
Karger:
Basel.
Buchthal,
F.,
and
Schmalbruch,
H.
(1970).
Contraction
times
and
fibre
types
in
intact
human
muscle.
Acta
Physiologica
Scandinavica,
79,
435-452.
Burke,
D.,
Skuse,
N.
F.,
and
Lethlean,
A.
K.
(1974a).
Isometric
contraction
of
the
abductor
digiti
minimi
muscle
in
man.
Journal
of
Neurology,
Neurosurgery,
and
Psychiatry.
(In
press.)
Burke,
D.,
Skuse,
N.
F.,
and
Lethlean,
A.
K.
(1974b).
The
contractile
properties
of
the
abductor
digiti
minimi
muscle
in
paramyotonia
congenita.
Journal
of
Neurology,
Neurosurgery,
and
Psychiatry,
37,
894-899.
Hannerz,
J.
(1973).
Discharge
properties
of
motor
units
in
man.
Experientia,
29,
4546.
Haynes,
J.,
and
Thrush,
D.
C.
(1972).
Paramyotonia
con-
genita:
an
electrophysiological
study.
Brain,
95,
553-558.
Joyce,
G
C.,
Rack,
P.
M.
H.,
and
Westbury,
D.
R.
(1969).
The
mechanical
properties
of
cat
soleus
muscle
during
controlled
lengthening
and
shortening
movements.
Journal
of
Physiology,
204,
461474.
Marsden,
C.
D.,
Meadows,
J.
C.,
and
Merton,
P.
A.
(1971).
Isolated
single
motor
units
in
human
muscle
and
their
rate
of
discharge
during
maximal
voluntary
effort.
Journal
of
Physiology,
217,
12-13P.
Merton,
P.
A.
(1954).
Voluntary
strength
and
fatigue.
Journal
of
Physiology,
123,
553-564.
Preswick,
G,
Stewart,
R.
D.
H.,
O'Hara,
P.,
and
Murray,
I.
P.
C.
(1966).
The
value
of
muscle
twitch
and
Achilles
reflex
recordings
in
thyroid
disorders.
Medical
Journal
of
Australia,
1,
473477.
Tanji,
J.,
and
Kato,
M.
(1972).
Discharges
of
single
motor
units
at
voluntary
contraction
of
abductor
digiti
minimi
muscle
in
man.
Brain
Research,
45,
590-593.
906
