
Downloaded from http://journals.lww.com/anesthesia-analgesia by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8KKGKV0Ymy+78= on 11/28/2021
Downloaded from http://journals.lww.com/anesthesia-analgesia by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8KKGKV0Ymy+78= on 11/28/2021
Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
68 www.anesthesia-analgesia.org July 2021
•
Volume 133
•
Number 1
Trauma
Vasopressors in Trauma: A Never Event?
Justin E. Richards, MD,* Tim Harris, MD,†‡ Martin W. Dünser, MD,§ Pierre Bouzat, MD, PhD,‖
and Tobias Gauss, MD¶
Vasopressor use in severely injured trauma patients is discouraged due to concerns that vasocon-
striction will worsen organ perfusion and result in increased mortality and organ failure in hypotensive
trauma patients. Hypotensive resuscitation is advocated based on limited data that lower systolic
blood pressure and mean arterial pressure will result in improved mortality. It is classically taught that
hypotension and hypovolemia in trauma are associated with peripheral vasoconstriction. However, the
pathophysiology of traumatic shock is complex and involves multiple neurohormonal interactions that
are ultimately manifested by an initial sympathoexcitatory phase that attempts to compensate for
acute blood loss and is characterized by vasoconstriction, tachycardia, and preserved mean arterial
blood pressure. The subsequent hypotension observed in hemorrhagic shock reects a sympatho-
inhibitory vasodilation phase. The objectives of hemodynamic resuscitation in hypotensive trauma
patients are restoring adequate intravascular volume with a balanced ratio of blood products, correcting
pathologic coagulopathy, and maintaining organ perfusion. Persistent hypotension and hypoperfusion
are associated with worse coagulopathy and organ function. The practice of hypotensive resuscitation
would appear counterintuitive to the goals of traumatic shock resuscitation and is not supported by
consistent clinical data. In addition, excessive volume resuscitation is associated with adverse clinical
outcomes. Therefore, in the resuscitation of traumatic shock, it is necessary to target an appropriate
balance with intravascular volume and vascular tone. It would appear logical that vasopressors may be
useful in traumatic shock resuscitation to counteract vasodilation in hemorrhage as well as other clini-
cal conditions such as traumatic brain injury, spinal cord injury, multiple organ dysfunction syndrome,
and vasodilation of general anesthetics. The purpose of this article is to discuss the controversy of
vasopressors in hypotensive trauma patients and advocate for a nuanced approach to vasopressor
administration in the resuscitation of traumatic shock. (Anesth Analg 2021;133:68–79)
GLOSSARY
Ang II = angiotensin II; AVP = arginine vasopressin; BP = blood pressure; CPP = cerebral per-
fusion pressure; DAMPs = damage associated molecular patterns; EPI = epinephrine; HR =
heart rate; K
ATP
= adenosine-triphosphate sensitive potassium channels; MAP = mean arterial
pressure; MODS = multiple organ dysfunction syndrome; mRNA = messenger ribonucleic acid;
NOREPI = norepinephrine; RAS = renin-angiotensin system; RCT = randomized controlled trial;
SBP = systolic blood pressure; SCI = spinal cord injury; TBI = traumatic brain injury; TXA =
tranexamic acid; SVR = systemic vascular resistance
T
rauma is the leading cause of death in adults
<40 years old and uncontrolled blood loss is the
most common cause of preventable fatalities.
1
Traumatic hemorrhagic shock is responsible for an
estimated 49,000 deaths in the United States and 1.4
million patients worldwide each year.
1,2
By denition,
shock is the inadequate delivery of oxygen necessary
to maintain appropriate physiologic organ function.
1,3
The immediate goals in hemorrhagic shock are control
of mechanical bleeding, treatment of trauma-induced
coagulopathy, and restoration of intravascular vol-
ume. If hemorrhage cannot be controlled immediately,
management goals are to minimize further blood loss
until hemorrhage control can be achieved.
2,4,5
Recent advances in hemorrhagic shock resus-
citation are the early targeted administration of
tranexamic acid (TXA)
5–8
and the individualization of
blood product transfusion based on viscoelastic test-
ing.
9
Strategies of permissive hypotension
10,11
and con-
cerns of adverse effects have discouraged the use of
vasopressors as part of the resuscitation strategy. The
use of vasopressors in patients sustaining traumatic
injuries was considered deleterious and thought to
From the *Department of Anesthesiology, University of Maryland School
of Medicine, Divisions of Trauma Anesthesiology and Critical Care
Medicine, R Adams Cowley Shock Trauma Center, Baltimore, Maryland;
†The Bizard Institute, Queen Mary University, London, United Kingdom;
‡Department of Emergency Medicine, Hamad Medical Corporation, Doha,
Qatar; §Department of Anesthesiology and Critical Care Medicine, Kepler
University Hospital and Johannes Kepler University, Linz, Austria; ‖Pôle
Anesthésie Réanimation, Centre Hospitalier Universitaire Grenoble Alpes,
Grenoble Institut des Neurosciences, Grenoble Alpes University, Grenoble,
France; and ¶Anesthesia and Critical Care-Réanimation, Hôpital Beaujon,
Université de Paris, Paris, France.
Accepted for publication March 10, 2021.
Funding: None.
The authors declare no conicts of interest.
Reprints will not be available from the authors.
Address correspondence to Justin E. Richards, MD, Department of
Anesthesiology, University of Maryland School of Medicine, Divisions of
Trauma Anesthesiology and Critical Care Medicine, R Adams Cowley Shock
Trauma Center, 22 S Greene St, T1R77, Baltimore, MD. Address e-mail to jus-
Copyright © 2021 International Anesthesia Research Society
DOI: 10.1213/ANE.0000000000005552
LWW
E NARRATIVE REVIEW ARTICLE

Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
E
NARRATIVE REVIEW ARTICLE
July 2021
•
Volume 133
•
Number 1 www.anesthesia-analgesia.org 69
worsen clinical outcomes.
12
Vasopressor use is cur-
rently reserved for the postresuscitation period in
selected pathologies, such as maintaining cerebral
perfusion pressure (CPP) in patients with central ner-
vous system injury
13
or septic shock.
14
The administra-
tion of vasopressors to patients in hemorrhagic shock
is included in recent European guidelines
15
; however,
this was not commonly recommended in the United
Kingdom and United States.
In this narrative review, we describe the impact of
arterial hypotension and different forms of shock in
the acute resuscitation phase after traumatic injury
and discuss the controversy of vasopressor use in
trauma patients. There were no systematic a priori
inclusion criteria and no meta-analysis. To offer a bal-
anced overview for a diverse topic including a sum-
mary of the pathophysiology of shock, each author
performed their own literature search and papers
discussed were included by consensus. We did not
set out to formally appraise, score, and quality assess
included papers. Specically, for the selection of stud-
ies included in the Clinical Data on Vasopressors in
Trauma section, a single PubMed search was per-
formed for “vasopressors” and “trauma.” There were
284 results, of which 23 were peer-reviewed, clinical
studies evaluating the administration of vasopressors
involving human subjects with traumatic injuries.
These were reviewed and included in the discussion
on vasopressor use in acutely injured trauma patients.
Based on the ndings, we also specically address the
impact of norepinephrine (NOREPI) and arginine
vasopressin (AVP) in the trauma population.
PATHOPHYSIOLOGY OF HEMORRHAGE AND
SHOCK IN TRAUMA
Sympathoexcitatory Response to Hemorrhagic
Shock
Hemorrhage is the most common cause of prevent-
able death after traumatic injury and is characterized
by acute blood loss, coagulopathy, and arterial hypo-
tension.
1
Perhaps most intriguing from a pathophysi-
ologic standpoint is the impact of cardiovascular
mechanisms involved in patients with hypovolemia
due to hemorrhage. Comprehensive discussion of
the pathophysiology of hemorrhagic shock is beyond
the scope of this review and has previously been
described.
16
Signs of hemorrhagic shock are classi-
cally taught as initial increasing heart rate, decreas-
ing pulse pressure, and increasing respiratory rate
with a later (monophasic) decrease in systolic blood
pressure (SBP) and mean arterial pressure (MAP).
Early MAP and cardiac output are maintained by
tachycardia compensating for reduced stroke volume
due to decreased venous return. However, hemor-
rhagic shock presents with variable changes in arte-
rial blood pressure. Even in stages III and IV of shock
(ie, >30%–40% circulating volume lost), observational
data suggest that some patients may still maintain
SBP >90 mm Hg.
17
Schadt and Ludbrook
16
summarize the pathophysi-
ology of acute blood loss in conscious mammals in 2
phases: (1) initial vasoconstriction (sympathoexcit-
atory) phase and (2) later vasodilatory (sympatho-
inhibitory) phase. During the sympathoexcitatory
phase, arterial blood pressure is maintained by an
increase in systemic vascular resistance (SVR). It is
also during this nonhypotensive phase that heart rate
increases, in part due to loss of resting cardiac vagal
stimulation and an increased cardiac sympathetic
drive.
18
The early response is largely driven by the
sympathetic nervous system (Figure 1). The endo-
crine response to the early phase of acute hypovole-
mia includes an increase in plasma concentrations of
angiotensin-II as a consequence of the renin-angio-
tensin system (RAS) and a lesser relative increase in
AVP, epinephrine (EPI), and NOREPI.
18
In summary,
the sympathoexcitatory phase represents a classic
description of the signs and symptoms of early hem-
orrhagic shock and vasoconstriction.
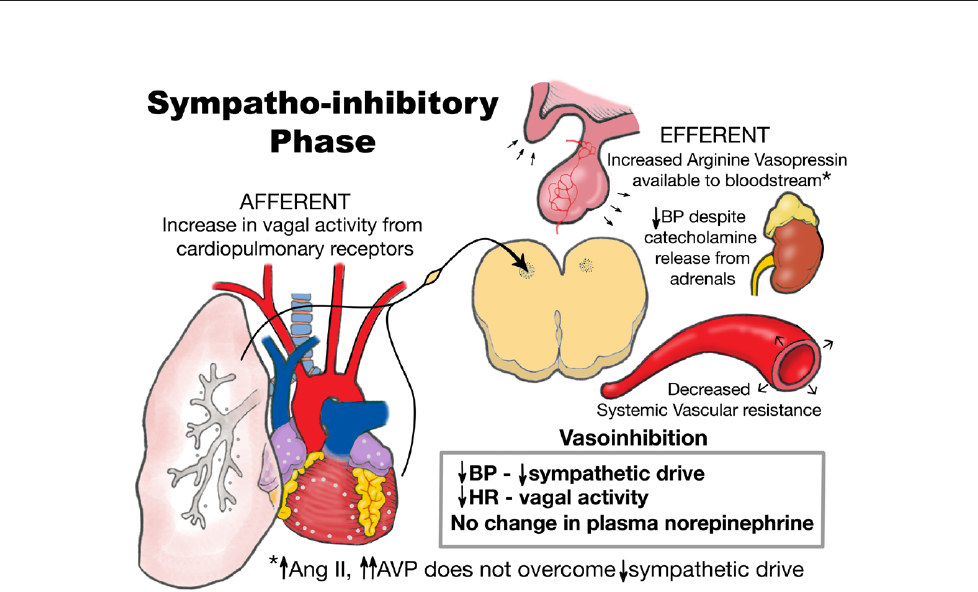
Sympathoinhibitory Response to Hemorrhagic
Shock
The initial vasoconstrictive and sympathoexcitatory
response to acute blood loss evolves into a sympa-
thoinhibitory phase characterized by distributive
shock as a consequence of vascular hyporeactivity
(Figure 2). Studies in animals and human subjects
demonstrate that the occurrence of late arterial hypo-
tension after hypovolemia is the result of a decrease in
sympathetic nervous system activity and subsequent
arterial vasodilation and bradycardia.
16,18,19
The exact
mechanistic input from the autonomic nervous sys-
tem that contributes to the sympathoinhibitory phase
is incompletely understood in humans; however, it
is theorized to involve cardiopulmonary vagal nerve
reexes.
16
During the later phases of hemorrhage, the adrenal
medulla increases production of both EPI and NOREPI
in response to hypotension; however, this does not
appear to offset the vasodilation of the sympathoin-
hibitory phase.
18
The physiologic effect of these neu-
rohormones during this phase is not clear, and the
hemodynamic response to blood loss is not altered
by adrenal denervation in animal studies.
16
There are
also contributions from other neurohormones dur-
ing the sympathoinhibitory phase of hemorrhage.
Angiotensin II and AVP both increase in response to
ongoing blood loss and are involved in the restora-
tion of arterial blood pressure after hemorrhage.
18
However, if blood loss continues precipitously, there
is a physiologic exhaustion of these neurohormones,
even to subphysiologic levels.
20
The depletion of AVP

Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
70 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Vasopressors and Trauma
stores (and likely NOREPI) contributes to a deciency
syndrome characterized by a loss of vascular tone.
In the decompensated sympathoinhibition phase,
even blood transfusion may not restore arterial blood
pressure.
21
Shock-Induced Endotheliopathy
Endothelial dysfunction after injury is recognized as a
signicant contributing factor to the pathophysiology
of posttraumatic hemorrhagic shock.
22,23
Representing
one of the largest organs in the body, the endothelium
is composed of the inner cellular lining of blood and
lymphatic vessels.
24
The intact endothelium maintains
vascular patency, regulates uid permeability, and
controls vasomotor tone. In addition, the endothelium
participates in natural anticoagulation via hepari-
noids and antithrombin in the endothelial glycocalyx
that allows the passage of oxygen and nutrients car-
rying blood through the vasculature.
24
Damage to the
endothelium via either direct tissue injury or subse-
quent inammatory products compromises both the
mechanical and chemical integrities of the endothelial
layer. Traumatic shock results in endothelial glycoca-
lyx damage that contributes to trauma-induced coag-
ulopathy, microvascular dysfunction, and multiple
organ dysfunction syndrome (MODS).
22
A feature of
posttraumatic endotheliopathy is the increase in vas-
cular permeability, tissue edema, and loss of vascu-
lar vasomotor tone.
23,25
The ensuing vasodilatation
appears similar in homology to that of septic shock.
22
The relationships among endothelial damage, injury
severity, coagulopathy, and organ dysfunction are an
association, and therapeutic targets have not yet been
proven.
Pathophysiology of TBI and SCI
Traumatic brain injury (TBI) is the most common
cause of death and disability after injury.
26,27
The 2
components of TBI are as follows: primary (ie, at
the time of impact) injury and secondary injury for
derangements that follow (ie, hypoxia, arterial hypo-
tension, hyperthermia, etc).
27
Therapies can, therefore,
impact only the latter. After TBI, the cerebrovascular
tone becomes more sensitive to changes in acid-base
balance and cerebral blood ow attempts to meet the
demands of the cerebral metabolic rate even at the
expense of increasing intracranial pressure.
27
Cerebral
autoregulation becomes impaired such that the brain
is unable to maintain constant cerebral perfusion over
a range of MAPs. Consequently, arterial hypotension
may cause cerebral hypoxia and observational studies
have associated arterial hypotension with increased
mortality in TBI patients.
28,29
Similar to TBI, spinal cord injury (SCI) is associated
with signicant morbidity and health-related costs in
survivors.
13
Injuries to the cervical and upper thoracic
spinal column are at particular risk of cardiovascular
decompensation due to loss of sympathetic tone and
unopposed vagal stimulation below the level of injury
resulting in vasodilatation, bradycardia, and impaired
Figure 1. Sympathoexcitatory
phase of hemorrhagic shock.
Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
E
NARRATIVE REVIEW ARTICLE
July 2021
•
Volume 133
•
Number 1 www.anesthesia-analgesia.org 71
cardiac pump function, all leading to tissue hypoperfu-
sion and shock (ie, neurogenic shock). Cardiovascular
complications represent one of the leading causes of
mortality in patients with SCI.
30
Arterial hypotension
has been associated with worse functional outcomes,
likely attributed to inadequate spinal cord perfusion.
31,32
Recent guidelines from the American Association of
Neurological Surgeons and the Congress of Neurological
Surgeons’ Guidelines for the Management of Acute
Cervical Spine and Spinal Cord Injuries recommend an
MAP of 85 to 90 mm Hg after traumatic SCI.
33
Pathophysiology of Multiple Organ Dysfunction
Syndrome
Historically MODS was noted to occur in nearly 50%
of severely injured patients.
34
However, these originate
from an era of large volume crystalloid administration
and uneven ratios of red blood cells, plasma, and plate-
let transfusion. Both trauma-associated mortality and
the incidence of posttraumatic MODS have decreased
during the past 20 years.
35
Increasing injury severity,
shock severity, large volume blood product resuscita-
tion, and arterial hypotension are all independently
associated with posttraumatic MODS.
36
In addition,
vasodilatory complications associated with endo-
theliopathy and the inammatory response further
contribute to hypotension, hypoperfusion, and the
development of MODS in the trauma population.
22,37
The pathophysiologic mechanisms underlying
the development of MODS after traumatic injury are
related to the immunologic response to tissue injury
and blood loss, dysregulation of coagulation, hemo-
stasis, and endothelial function, neuroinammation,
endocrine dysfunction, and baseline demographic
differences, such as age, sex, and premorbid medical
conditions.
37
Tissue injury results in the release of bio-
molecular mitochondrial deoxyribonucleic acid and
damage-associated molecular patterns from necrotic
cells that stimulate the production of complement and
activity of immunologic cells, such as monocytes and
T-cells.
37,38
Acute hemorrhage contributes to hypo-
tension, hypoperfusion, and acidemia which lead to
further cell death. In addition, severe hemorrhage
is associated with an acute traumatic coagulopathy
that contributes to further blood loss and inability to
achieve adequate hemostasis. Tissue injury and blood
loss also impact the function and integrity of the vas-
cular endothelium.
22,23
Despite initial robust produc-
tivity, endocrine functions are dramatically altered,
as demonstrated by changes in cortisol, insulin, and
vasopressin levels. Finally, older age is signicantly
associated with increased risk of organ dysfunction
and multiple organ failure after traumatic injury,
potentially due to age-related changes in the postin-
jury inammatory response.
36,37
Similar to septic shock, a solidifying theme in post-
traumatic MODS is the relationship of prolonged
hypotension and hypoperfusion that is associated
with clinical shock, vascular dysfunction, and vasodi-
lation.
14
The patterns of tissue damage, hypotension,
Figure 2. Sympathoinhibitory phase of hemorrhagic shock. Ang II indicates angiotensin II; AVP, arginine vasopressin; BP, blood pressure; HR,
heart rate.

Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
72 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Vasopressors and Trauma
hypoperfusion, cellular dysfunction, and death are
repeated with ongoing hemorrhage after signi-
cant injury.
22
Certain resuscitation measures, such as
administration of large intravascular volume, further
exacerbate organ dysfunction and increase the risk of
MODS.
36
Additionally, the immunologic ramications
of organ failure contribute to greater susceptibility to
infectious pathogens, development of septic shock,
vasodilation, and further organ dysfunction.
37
Blunt Versus Penetrating Trauma
The mechanism of traumatic injury along with the
transfer and dispersal of energy is associated with
patterns of tissue damage and inammation. For
example, trauma patients with a high-energy blunt
mechanism often sustain multisystem injuries,
including TBI and pelvic or long-bone fractures. The
degree of soft tissue injury is associated with systemic
inammation and organ dysfunction in severely
injured blunt trauma patients.
39
Quantication of the
volume of clinical shock is valuable in predicting the
response to severe injury and subsequent MODS.
40
However, the systemic and microcirculatory effects of
severe clinical shock are likely different and, in part,
based on the underlying mechanism of injury.
41,42
Recent evidence from 2 a priori harmonized,
prospective randomized controlled trial (RCTs)
demonstrate the benet of a targeted prehospi-
tal resuscitation therapy in blunt trauma patients,
whereas a signicant difference in mortality was not
observed among patients with a penetrating injury.
41
Possible explanations for these observations among
blunt and penetrating mechanisms are related to basic
characteristics of the injured population and nature of
the injuries. In addition, literature suggests that blunt
mechanisms of injury, such as that occur after motor-
vehicle and motorcycle collisions, are associated with
overall longer prehospital transport times compared
to penetrating injuries that tend to occur in urban
environments.
41,43,44
Finally, the volume of shock after
severe injury, along with subsequent alterations and
derangements in coagulation, is associated with clini-
cal outcomes, such as organ failure
36,40,45
and mortal-
ity,
3
and likely inuenced by mechanism of injury.
Vasodilation
Vasodilation is a common manifestation in the vari-
ous forms of shock after traumatic injury. While
initial vasoconstriction is an early characteristic of
hemorrhage (ie, sympathoexcitatory phase), contin-
ued blood loss with subsequent hypotension reects
a state of vasodilation. Both neurogenic and septic
shock are also characterized by a decrease in SVR and
resultant hypotension.
13,46
Vasodilatory shock is the
most common form of shock and represents the nal
common pathway for severe shock from any cause.
47
Persistent hypotension and hypoperfusion contribute
to further vascular dysfunction from which resusci-
tation does not contribute to the recovery of vascu-
lar tone.
47
Therefore, ongoing shock results in organ
dysfunction and exacerbates persistent vascular and
hematologic failure.
3
The pathophysiologic mechanisms behind vasodi-
lation are related to vascular smooth muscle relaxation
via the adenosine triphosphate-sensitive potassium
(K
ATP
) channels,
47
synthesis of nitric oxide,
48
and vaso-
pressin deciency.
16,49
Activation of the K
ATP
channels
results in cellular hyperpolarization, which prevents
the inux of calcium ions and inhibits cycling of actin-
myosin cross-linkages. Increased production of nitric
oxide occurs in vascular smooth muscle cells as well
as the vascular endothelium. Nitric oxide is a vaso-
dilator that functions through activation of myosin
light-chain phosphatase as well as potassium-sensi-
tive calcium channels. Under physiologic conditions,
activation of these channels limits the activity of vaso-
constrictive agents.
47
However, a vasodilatory state is
expressed after pathologic stimulation through nitric
oxide. Finally, vasodilation is also represented by a
vasopressin deciency, which is well documented in
septic shock,
50
postcardiopulmonary bypass,
51
and
hemorrhagic shock.
20
CLINICAL DATA ON VASOPRESSORS IN TRAUMA
Despite vasodilation representing the nal common
and unifying pathway in different forms of shock
after traumatic injury, clinical studies have demon-
strated the disadvantages of vasoconstrictive agents
in the trauma population. The concerns about vaso-
pressor use in trauma patients include rapid increases
in arterial blood pressure, increased cardiac afterload,
arrhythmias, and reduced tissue perfusion with sub-
sequent organ dysfunction.
12,52
Initial clinical reports were that early vasopres-
sor use (ie, phenylephrine, NOREPI, or AVP), within
the rst 12 hours after injury, was associated with
increased mortality even after adjusting for the vol-
ume of crystalloid resuscitation.
12
In a retrospective
study, Collier et al
53
reported an increased risk of mor-
tality in trauma patients who received AVP within 72
hours of hospital admission. Another retrospective
investigation compared 1349 trauma patients from a
single center exposed to any vasoactive drug within
24 hours of admission and showed mortality rates of
43.6% vs 4.2%.
54
Further single-center, retrospective
studies demonstrated similar ndings.
55–57
A system-
atic review on vasopressor use in trauma patients
identied a signicant association between vaso-
pressor use and increased short-term mortality,
52
and
administration of vasopressors after initial damage
control laparotomy quadrupled the rate of anastomo-
sis failure.
58
A more recent Japanese database study

Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
E
NARRATIVE REVIEW ARTICLE
July 2021
•
Volume 133
•
Number 1 www.anesthesia-analgesia.org 73
included 298 patients who received vasopressors and
were propensity score-matched to subjects who did
not receive vasopressors.
59
Vasopressor use within 24
hours after hospital admission was associated with
greater inhospital mortality. These ndings are simi-
lar to a retrospective study of 40 patients with hem-
orrhagic shock who were administered dopamine or
NOREPI within 1 hour of hospital admission.
60
Specically, in patients with acute SCI, vasopressor
administration, reported most commonly in the form
of dopamine and phenylephrine, was associated with
an increased risk of complications, such as tachyar-
rhythmias and troponin elevation.
61
These results
were corroborated in a retrospective investigation of
556 patients with TBI.
62
Another investigation evalu-
ated the Nationwide Inpatient Sample for patients
who received a craniotomy for signicant trauma.
Patients who received vasopressors had an increased
risk of death; however, the results were not adjusted
for injury severity, admission Glasgow Coma Scale,
or metabolic markers associated with secondary
brain injury.
63
Ultimately, vasopressors are associated
with higher MAP and CPP but also an increased risk
of complications.
64
A previous retrospective study
reported in patients with central cord syndrome
reported an association with improved neurologic
function and exposure to any vasopressor.
65
A more
recent investigation of traumatic SCI observed that
patients who achieved more frequent MAP measure-
ments ≥85 mm Hg were more commonly exposed to
vasopressors and were signicantly more likely to
have an improvement in neurologic outcome.
32
Based
on the available human clinical data in nonrandom-
ized studies, there are limited high-quality data dem-
onstrating an association with improved survival or
neurologic outcome and vasopressor administration
in patients with neurologic injury,
66–68
which is an
important consideration when administering vaso-
pressors to patients with severe TBI or SCI.
The optimal arterial blood pressure target for resusci-
tation of patients with hemorrhagic shock is unknown.
Prolonged hypotension and hypoperfusion are asso-
ciated with an increased risk of organ failure and
death. Registry data suggest an association between
arterial blood pressures <110 mm Hg and mortality.
69
However, this nding does not necessarily imply that
normalizing arterial blood pressure improves out-
comes or organ perfusion. A clinical concern is the
reported harm of vasopressors when administered
with the goal to increase blood pressure. Ultimately, an
important clinical question is “Does early vasopressor
administration increase mortality and complications in
severely injured trauma patients?”
A retrospective, propensity score–matched cohort
study observed no signicant increase with inhos-
pital mortality in patients who received prehospital
NOREPI.
70
In addition, a retrospective study of
746 trauma patients requiring emergent operations
observed no signicant increase in mortality in
patients who received vasopressors, exclusive of EPI.
71
In the study that found AVP use was associated with
increased mortality risk, when patients were stratied
by whether they received only AVP or AVP in combi-
nation with another vasoactive, there was no differ-
ence in the risk of mortality in patients who received
only AVP.
53
A further investigation noted that severely
injured patients with TBI were signicantly more
likely to receive vasopressors. Although no difference
was found in the volume of crystalloid or blood prod-
uct transfusion, clinical outcome data with regard to
vasopressors were not specically reported.
56
Two RCTs suggest that AVP administration may
improve blood pressure while not worsening blood
loss or increasing mortality in patients with hemor-
rhagic shock.
72,73
A prospective randomized trial of
early infusion of low-dose AVP (ie, 2.4 IU/h for 5
hours on arrival at the emergency department) ver-
sus placebo in trauma patients resulted in the lower
requirement of total uids at 24 hours.
72
The study
was underpowered to show a signicant difference
in death. Among the AVP and control groups, respec-
tively, there was no difference in mortality at 24 hours
(13% vs 23%, P =.28), 5 days (13% vs 25%, P = .19),
or the primary outcome of 30-day mortality (34% vs
28%, P = .52). Most recently, a single-center, prospec-
tive RCT demonstrated that a continuous AVP infu-
sion did not increase mortality but was associated
with a lower need for blood product transfusion in
trauma patients who required massive transfusion.
Included patients were at risk for hemorrhagic shock
and received 6 units of blood product within 12 hours
of admission.
73
The authors hypothesized that an
exogenous supply of AVP may not only increase vas-
cular tone but also support hemostasis. Further stud-
ies in patients with TBI demonstrate that AVP was
associated with less administration of hyperosmolar
therapy and is a potential option and alternative to
catecholamines for CPP management.
74,75
PHARMACODYNAMICS OF NOREPI AND ARGININE
VASOPRESSIN
Numerous retrospective studies in the trauma lit-
erature have investigated multiple vasopressors (ie,
NOREPI, phenylephrine, dopamine, and AVP).
12,52,54,59
This discussion focuses on the 2 most common and
clinically important vasopressors in this population:
NOREPI and AVP (Table). Administration of EPI to
patients in hemorrhagic shock has been studied in
the setting of prehospital cardiac arrest
76
but it has
not been specically examined as a vasopressor in
isolation with trauma patients. NOREPI is a neuro-
hormone released from sympathetic, postganglionic

Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
74 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Vasopressors and Trauma
nerve bers and is a product of the decarboxylation
of dopamine. It is stored in presynaptic granules that
release their content in the synaptic space on depo-
larization. After release, NOREPI acts on postsynaptic
α- and (to a lesser extent) β-receptors.
46,77
The effects
on both receptors are dose-dependent; with increas-
ing doses, the α-receptor effect dominates. This
results in: (1) contraction of smooth muscles bers in
venous and arterial vessels inducing venoconstriction
and an increase in venous return (ie, recruitment of
unstressed volume) as well as arteriolar vasoconstric-
tion and (2) myocardial inotropic and chronotropic
stimulation.
77–79
The physiology of AVP has been described in
detail.
49,80
AVP is a neuroendocrine nonapeptide,
produced in the neurons of the paraventricular and
supraoptic nuclei in the posterior hypothalamus.
46
AVP acts on multiple G-protein–coupled recep-
tors and uses the phosphatidylinositol pathway to
increase Ca
2+
inux.
49
AVP-1 receptors are densely
situated on vascular smooth muscles of the systemic,
splanchnic, renal, and coronary circulation; their
stimulation leads to potent vasoconstriction,
49
con-
comitant increase in cardiac output, and centraliza-
tion of blood volume.
81
In renal efferent arterioles, this
vasoconstriction increases glomerular ltration rate.
In the pulmonary vasculature, AVP induces less vaso-
constriction than NOREPI.
46,77
Platelet AVP-1 recep-
tor stimulation facilitates thrombocyte aggregation.
82
AVP-2 receptors located in the renal collecting system
induce antidiuresis by shuttling aquaporin-2 con-
taining vesicles to the cell surface and stimulation of
synthesis of aquaporin-2 messenger ribonucleic acid
(mRNA). There is also a complex physiologic inter-
action of AVP on oxytocin and purinergic receptors.
Purinergic receptors on the cardiac endothelium seem
to exert a positive inotropic effect without associated
positive chronotropy and without a resultant increase
in oxygen demand.
83
In some vascular beds, such as
the lung, AVP binding to oxytocin receptors leads to
pulmonary vasodilation.
77
CURRENT GUIDELINES FOR HEMORRHAGIC
SHOCK AND GAPS IN CLINICAL KNOWLEDGE
The current paradigm for trauma resuscitation bal-
ances restoring organ perfusion, providing hemo-
static resuscitation,
84
and minimizing coagulopathy.
4
Therapy components include blood products,
85
a
period of permissive hypotension, rapid imaging,
and damage control surgical techniques.
86
Multiple
organizational guidelines exist for the management of
hemorrhagic shock, such as the European Guideline
on Management of Major Bleeding and Coagulopathy
Following Trauma,
15
Advanced Resuscitative Care
in Tactical Combat Casualty Care,
8
and the Eastern
Association for the Surgery of Trauma Clinical
Practice Guidelines for Damage Control Resuscitation
in Patients with Severe Traumatic Hemorrhage.
5
Common principal themes in each guideline are the
minimization of crystalloid administration, early
transfusion of blood products in prespecied ratios,
and administration of hemostasis adjuncts, such as
TXA. Aggressive resuscitation with excessive crys-
talloid volumes is associated with increased rates of
MODS and mortality.
36
In addition, limited prehospital
crystalloid resulted in decreased mortality in patients
with penetrating torso trauma.
87
Furthermore, devel-
opment of resuscitation protocols and established
ratios of blood product administration is associated
with improved clinical outcomes.
4,85
Early plasma-
based resuscitation contributes a signicant mortality
benet in trauma patients.
43,44
Administration of TXA
within 3 hours of injury has also demonstrated a sig-
nicant improvement in mortality for trauma patients
at risk for blood product transfusion
6
; however, more
recent evidence from mature and developed trauma
systems is generating continued controversy on this
topic.
88–90
The practice of permissive hypotension is
also advocated by some organizations
5
; however,
vasopressor administration is only recommended in
the European guidelines.
15
Resuscitation with permissive hypotension has long
been a component of early hemorrhagic shock resus-
citation. This strategy aims to tolerate lower arterial
blood pressures to minimize further blood loss from
the bleeding site due to lower hydrostatic pressures
and reduce resuscitation volumes, most importantly
crystalloid uid administration.
10
Multiple RCTs
87,91–
93
and a meta-analysis
11
advocate that permissive
hypotension is associated with decreased mortality.
However, there are numerous methodologic prob-
lems. In the recent meta-analysis, the included studies
were of poor to moderate quality due to lack of blind-
ing and incomplete protocol reporting.
11
In addition,
Table. Common Vasopressors Administered in Traumatic Shock
Vasopressor Mechanism Physiologic response
Norepinephrine
α-1-receptor agonist with modest β-1-agonist
activity
Augment venous return and central systemic vascular volume increase coronary
perfusion via α-1 and support cardiac contractility through β-1 activity
Vasopressin V
1
, V
2
receptors Activation of V
1
receptors and increasing vascular tone with vasoconstriction
via multiple G-proteins and regulation of intravascular volume resorption
via V
2
receptors in collecting tubules

Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
E
NARRATIVE REVIEW ARTICLE
July 2021
•
Volume 133
•
Number 1 www.anesthesia-analgesia.org 75
individual RCTs report heterogeneous SBP and MAP
targets with inconsistent effects. A majority of studies
also excluded patients with TBI. Furthermore, despite
tolerating lower blood pressures, the MAPs were nor-
mal and there were no statistical differences in the end
point blood pressures between intervention and control
groups in several clinical trials
91–93
that raise the ques-
tion on whether permissive hypotension was achieved.
The only RCT in the meta-analysis, which dem-
onstrated a primary difference in mortality and con-
tributed >50% of patients to the meta-analysis, was
performed in patients with penetrating torso trauma
who were randomized to either a restrictive or a lib-
eral crystalloid resuscitation strategy.
87
The SBP in the
restrictive group was lower than in the liberal crystal-
loid group (72 vs 79 mm Hg, P = .02); however, the
clinical implications of this difference are likely mini-
mal. The role of permissive hypotension in the era of
whole blood resuscitation is also unexplored and the
period of organ hypoperfusion may contribute to sub-
sequent MODS. Prolonged periods of arterial hypo-
tension and hypoperfusion in nontrauma surgery are
associated with increased rates of myocardial injury,
94
acute kidney injury,
94,95
and severe coagulopathy.
3,96
A
review of the literature would seemingly advocate for
permissive hypotension in bleeding trauma patients.
Although this lower level of evidence appears to sup-
port use of lower arterial blood pressure, avoidance
of vasopressors in trauma patients to achieve permis-
sive hypotension represents a signicant gap in clini-
cal knowledge and practice.
RECOMMENDATIONS FOR A NUANCED APPROACH
TO HEMORRHAGIC SHOCK AND VASOPRESSORS
Acute hemorrhage is a common cause of hemo-
dynamic decompensation and death
85,97
; however,
trauma patients and their injury proles are often het-
erogeneous.
98
Moreover, circulatory instability after
hemorrhage in trauma patients may occur at different
temporal periods and have several, often overlapping
causes (Figure3). Different injury patterns and dis-
ease processes contribute to multiple causes of post-
traumatic shock. TBI may induce persistent shock,
99
and TBI patients seem to be at particular risk for pro-
longed arterial hypotension.
29
Prior studies that deter-
mined vasopressors are associated with increased
mortality in trauma patients excluding patients with
TBI. Therefore, the full impact of hypotension and
vasopressor administration in a large portion of the
trauma population is not dened.
Vasopressors have a sound mechanism to improve
oxygen delivery by decreasing venous system compli-
ance, augmenting the mean systemic lling pressure,
and thereby increasing the stressed blood volume
and cardiac output within the circulation.
79,100,101
Regardless of whether vasopressors contribute to
an improvement in the repayment of oxygen debt
after hemorrhagic shock in humans must be criti-
cally examined by further clinical studies. The use
of vasopressors in hemorrhagic shock is supported
by European guidelines,
15
and an argument for the
therapeutic use of NOREPI or AVP in traumatic shock
resuscitation is to augment the body’s physiological
response and maintain homeostasis.
80
To date, AVP is
the only agent evaluated in trauma patients via RCTs,
albeit small population size.
There are certain clinical scenarios in which early
vasopressor use with NOREPI or AVP would be rec-
ommended in trauma patients
102
(Figure3). For exam-
ple, severe brain injury is frequently encountered after
blunt mechanisms of injury.
103
Guidelines from the
Brain Trauma Foundation suggest achieving specic
blood pressure targets to achieve a CPP of 60 to 70 mm
Hg, with vasoactive agents as necessary, to minimize
the insult of secondary injury. The detrimental effects
of permissive hypotension in severely injured patients
with TBI are a signicant concern.
104,105
Administration
of NOREPI or AVP has been successfully utilized in
this population to maintain CPP and without increases
in morbidity.
32,71,74
Moreover, in acute, massive
Figure 3. Pathophysiology, temporal evolution, and patterns of traumatic hemorrhagic shock. DAMPs indicates damage associated molecular
patterns.

Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
76 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Vasopressors and Trauma
exsanguination, there is decreased venous return,
consequent reduced cardiac output, loss of coronary
perfusion pressure, and ultimately prehospital car-
diac arrest. Vasopressin or NOREPI administration
maintain venous return, cardiac output, and coro-
nary perfusion pressure until surgical hemorrhagic
control.
106,107
In addition, persistent hemorrhage and
arterial hypotension unresponsive to continued blood
product transfusion would benet from vasopressor
administration to maintain organ perfusion. It is likely
that this situation may already be encountered in the
operating room when the sympathoinhibitory phase
of hemorrhagic shock occurs before hemorrhage con-
trol.
16,102,108
In addition, vasopressors may be necessary
due to effects of intravenous and inhalational anes-
thetic agents that blunt the physiologic, sympathetic
vasoconstrictive response and further enhance vaso-
dilatation.
108
Persistent and prolonged shock with
severe tissue damage and release of proinammatory
mediators also aggravates vasodilation and neces-
sitates vasopressor administration even after deni-
tive hemorrhage control.
37,102
Finally, NOREPI may be
benecial after hemorrhage control (ie, in the intensive
care unit) in patients demonstrating early organ dys-
function as a result of persistent inammation, vaso-
dilation, and MODS in the postresuscitation period
78
(Figure3), as determined by bedside echocardiogra-
phy
109–111
or invasive hemodynamic indices.
The administration of vasopressors to patients in
hemorrhagic shock appears counterintuitive to the
paradigm practice of hypotensive resuscitation and
permissive hypotension. However, limited high-qual-
ity evidence supports permissive hypotension, par-
ticularly in the era of balanced blood product-based
resuscitation and the reemergence of whole blood
transfusion.
112
Furthermore, the pathophysiologic
stages of hemorrhage demonstrate that vasodilation
likely occurs in a proportion of hypotensive patients
with acute blood loss.
16,102
In these clinical situations,
we advocate for vasopressor therapy with NOREPI or
AVP. This is consistent with European guidelines on
the management of blood loss after traumatic injury.
15
However, vasopressor administration in the bleeding
trauma patient must be exercised with caution and in
concert with appropriate intravascular resuscitation
(ie, early blood product transfusion). The decision to
decrease vasopressor support must also be made in
the clinical context of an improving metabolic acid-
base status
113–116
and appropriate echocardiographic
parameters and cardiac function.
109–111
Further inves-
tigations are necessary to more clearly delineate the
temporal course of vasodilation and vascular dysfunc-
tion after hemorrhagic shock. Additional work is also
necessary to determine optimal blood pressure tar-
gets and organ perfusion markers in specic trauma
populations, such as blunt mechanisms of injury and
TBI, and in patients resuscitated with whole blood.
CONCLUSIONS
The use of vasopressors is traditionally cautioned
against in the management of traumatic hemorrhagic
shock. However, the pathophysiology of shock in
trauma patients is complex. Multiple clinical scenarios
exist, which may warrant early administration of AVP
or NOREPI, along with appropriately titrated volume
administration and resuscitation. Further scientic
work is necessary to better dene specic vasopressor
medications, optimal arterial blood pressure goals,
and resuscitation strategies that are most benecial
to the critically injured trauma patient. Based on the
current literature, we conclude that clinical equipoise
exists and will only be solved by adequately powered,
multicenter, prospectively randomized trials.
E
ACKNOWLEDGMENTS
The authors acknowledge and are grateful to Mark J.
Wieber, MA, BSN, for the illustrations in Figures 1 and 2.
DISCLOSURES
Name: Justin E. Richards, MD.
Contribution: This author helped with manuscript concept,
design, content, and revision.
Name: Tim Harris, MD.
Contribution: This author helped with manuscript concept,
design, content, and revision.
Name: Martin W. Dünser, MD.
Contribution: This author helped with manuscript concept,
design, content, and revision.
Name: Pierre Bouzat, MD, PhD.
Contribution: This author helped with manuscript concept,
design, content, and revision.
Name: Tobias Gauss, MD.
Contribution: This author helped with manuscript concept,
design, content, and revision.
This manuscript was handled by: Richard P. Dutton, MD.
REFERENCES
1. Cannon JW. Hemorrhagic shock. N Engl J Med.
2018;378:1852–1853.
2. Brohi K, Gruen RL, Holcomb JB. Why are bleeding trauma
patients still dying? Intensive Care Med. 2019;45:709–711.
3. Bjerkvig CK, Strandenes G, Eliassen HS, et al. “Blood fail-
ure” time to view blood as an organ: how oxygen debt
contributes to blood failure and its implications for remote
damage control resuscitation. Transfusion. 2016;56(suppl
2):S182–S189.
4. Holcomb JB, Jenkins D, Rhee P, et al. Damage control resus-
citation: directly addressing the early coagulopathy of
trauma. J Trauma. 2007;62:307–310.
5. Cannon JW, Khan MA, Raja AS, et al. Damage control
resuscitation in patients with severe traumatic hemor-
rhage: a practice management guideline from the Eastern
Association for the Surgery of Trauma. J Trauma Acute Care
Surg. 2017;82:605–617.
6. Shakur H, Roberts I, Bautista R, et al; CRASH-2 trial col-
laborators. Effects of tranexamic acid on death, vascular
occlusive events, and blood transfusion in trauma patients

Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
E
NARRATIVE REVIEW ARTICLE
July 2021
•
Volume 133
•
Number 1 www.anesthesia-analgesia.org 77
with signicant haemorrhage (CRASH-2): a randomised,
placebo-controlled trial. Lancet. 2010;376:23–32.
7. Morrison JJ, Dubose JJ, Rasmussen TE, Midwinter
MJ. Military application of tranexamic acid in trauma
emergency resuscitation (MATTERs) study. Arch Surg.
2012;147:113–119.
8. Butler FK Jr, Holcomb JB, Shackelford S, et al. Advanced
resuscitative care in tactical combat casualty care: TCCC
guidelines change 18-01:14 October 2018. J Spec Oper Med.
2018;18:37–55.
9. Inaba K, Rizoli S, Veigas PV, et al; Viscoelastic Testing in
Trauma Consensus Panel. 2014 Consensus conference on
viscoelastic test-based transfusion guidelines for early
trauma resuscitation: report of the panel. J Trauma Acute
Care Surg. 2015;78:1220–1229.
10. Smith JB, Pittet JF, Pierce A. Hypotensive resuscitation. Curr
Anesthesiol Rep. 2014;4:209–215.
11. Tran A, Yates J, Lau A, Lampron J, Matar M. Permissive
hypotension versus conventional resuscitation strategies in
adult trauma patients with hemorrhagic shock: a systematic
review and meta-analysis of randomized controlled trials. J
Trauma Acute Care Surg. 2018;84:802–808.
12. Sperry JL, Minei JP, Frankel HL, et al. Early use of vaso-
pressors after injury: caution before constriction. J Trauma.
2008;64:9–14.
13. Stein DM, Knight WA 4th. Emergency neurological life sup-
port: traumatic spine injury. Neurocrit Care. 2017;27:170–180.
14. Angus DC, van der Poll T. Severe sepsis and septic shock. N
Engl J Med. 2013;369:840–851.
15. Spahn DR, Bouillon B, Cerny V, et al. The European guide-
line on management of major bleeding and coagulopathy
following trauma: fth edition. Crit Care. 2019;23:98.
16. Schadt JC, Ludbrook J. Hemodynamic and neurohumoral
responses to acute hypovolemia in conscious mammals. Am
J Physiol. 1991;260:H305–H318.
17. Guly HR, Bouamra O, Little R, et al. Testing the validity of
the ATLS classication of hypovolaemic shock. Resuscitation.
2010;81:1142–1147.
18. Sander-Jensen K, Mehlsen J, Stadeager C, et al. Increase
in vagal activity during hypotensive lower-body negative
pressure in humans. Am J Physiol. 1988;255:R149–R156.
19. Remington JW, Hamilton WF, Caddell HM, Boyd GH Jr,
Hamilton WF Jr. Some circulatory responses to hemorrhage
in the dog. Am J Physiol. 1950;161:106–115.
20. Sims CA, Guan Y, Bergey M, et al. Arginine vasopressin,
copeptin, and the development of relative AVP deciency
in hemorrhagic shock. Am J Surg. 2017;214:589–595.
21. Thiemermann C, Szabó C, Mitchell JA, Vane JR. Vascular
hyporeactivity to vasoconstrictor agents and hemodynamic
decompensation in hemorrhagic shock is mediated by nitric
oxide. Proc Natl Acad Sci U S A. 1993;90:267–271.
22. Johansson PI, Stensballe J, Ostrowski SR. Shock induced
endotheliopathy (SHINE) in acute critical illness: a unify-
ing pathophysiologic mechanism. Crit Care. 2017;21:25.
23. Johansson PI, Henriksen HH, Stensballe J, et al. Traumatic
endotheliopathy: a prospective observational study of 424
severely injured patients. Ann Surg. 2017;265:597–603.
24. Aird WC. Endothelium in health and disease. Pharmacol
Rep. 2008;60:139–143.
25. Kozar RA, Peng Z, Zhang R, et al. Plasma restoration of
endothelial glycocalyx in a rodent model of hemorrhagic
shock. Anesth Analg. 2011;112:1289–1295.
26. Marehbian J, Muehlschlegel S, Edlow BL, Hinson HE,
Hwang DY. Medical management of the severe traumatic
brain injury patient. Neurocrit Care. 2017;27:430–446.
27. Werner C, Engelhard K. Pathophysiology of traumatic brain
injury. Br J Anaesth. 2007;99:4–9.
28. Chesnut RM, Marshall LF, Klauber MR, et al. The role of
secondary brain injury in determining outcome from severe
head injury. J Trauma. 1993;34:216–222.
29. Spaite DW, Hu C, Bobrow BJ, et al. Association of out-of-
hospital hypotension depth and duration with traumatic
brain injury mortality. Ann Emerg Med. 2017;70:522–530.e1.
30. Furlan JC, Fehlings MG. Cardiovascular complications after
acute spinal cord injury: pathophysiology, diagnosis, and
management. Neurosurg Focus. 2008;25:E13.
31. Hawryluk G, Whetstone W, Saigal R, et al. Mean arterial
blood pressure correlates with neurological recovery after
human spinal cord injury: analysis of high frequency physi-
ologic data. J Neurotrauma. 2015;32:1958–1967.
32. Weinberg JA, Farber SH, Kalamchi LD, et al. Mean arte-
rial pressure maintenance following spinal cord injury:
does meeting the target matter? J Trauma Acute Care Surg.
2021;90:97–106.
33. Ryken TC, Hurlbert RJ, Hadley MN, et al. The acute car-
diopulmonary management of patients with cervical spinal
cord injuries. Neurosurgery. 2013;72(suppl 2):84–92.
34. Sauaia A, Moore EE, Johnson JL, Ciesla DJ, Bif WL,
Banerjee A. Validation of postinjury multiple organ failure
scores. Shock. 2009;31:438–447.
35. Sauaia A, Moore EE, Johnson JL, et al. Temporal trends
of postinjury multiple-organ failure: still resource inten-
sive, morbid, and lethal. J Trauma Acute Care Surg.
2014;76:582–592.
36. Minei JP, Cuschieri J, Sperry J, et al; Inammation and the
Host Response to Injury Collaborative Research Program.
The changing pattern and implications of multiple organ
failure after blunt injury with hemorrhagic shock. Crit Care
Med. 2012;40:1129–1135.
37. Lord JM, Midwinter MJ, Chen YF, et al. The systemic
immune response to trauma: an overview of pathophysiol-
ogy and treatment. Lancet. 2014;384:1455–1465.
38. Zhang Q, Raoof M, Chen Y, et al. Circulating mitochondrial
DAMPs cause inammatory responses to injury. Nature.
2010;464:104–107.
39. Frantz TL, Steenburg SD, Gaski GE, et al. Tissue damage
volume predicts organ dysfunction and inammation after
injury. J Surg Res. 2016;202:188–195.
40. McKinley TO, McCarroll T, Gaski GE, et al. Shock volume:
a patient-specic index that predicts transfusion require-
ments and organ dysfunction in multiply injured patients.
Shock. 2016;45:126–132.
41. Reitz KM, Moore HB, Guyette FX, et al. Prehospital plasma
in injured patients is associated with survival principally
in blunt injury: results from two randomized prehospital
plasma trials. J Trauma Acute Care Surg. 2020;88:33–41.
42. Moore HB, Moore EE, Neal MD, et al. Fibrinolysis shut-
down in trauma: historical review and clinical implications.
Anesth Analg. 2019;129:762–773.
43. Sperry JL, Guyette FX, Brown JB, et al; PAMPer Study
Group. Prehospital plasma during air medical transport in
trauma patients at risk for hemorrhagic shock. N Engl J Med.
2018;379:315–326.
44. Moore HB, Moore EE, Chapman MP, et al. Plasma-rst
resuscitation to treat haemorrhagic shock during emergency
ground transportation in an urban area: a randomised trial.
Lancet. 2018;392:283–291.
45. Gaski GE, Metzger C, McCarroll T, et al. Early immuno-
logic response in multiply injured patients with orthopae-
dic injuries is associated with organ dysfunction. J Orthop
Trauma. 2019;33:220–228.
46. Chow JH, Abuelkasem E, Sankova S, Henderson RA,
Mazzef MA, Tanaka KA. Reversal of vasodilatory shock:
current perspectives on conventional, rescue, and emerging

Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
78 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Vasopressors and Trauma
vasoactive agents for the treatment of shock. Anesth Analg.
2020;130:15–30.
47. Landry DW, Oliver JA. The pathogenesis of vasodilatory
shock. N Engl J Med. 2001;345:588–595.
48. Liu LM, Ward JA, Dubick MA. Hemorrhage-induced vascu-
lar hyporeactivity to norepinephrine in select vasculatures
of rats and the roles of nitric oxide and endothelin. Shock.
2003;19:208–214.
49. Holmes CL, Landry DW, Granton JT. Science review: vaso-
pressin and the cardiovascular system part 1–receptor
physiology. Crit Care. 2003;7:427–434.
50. Barrett LK, Singer M, Clapp LH. Vasopressin: mechanisms
of action on the vasculature in health and in septic shock.
Crit Care Med. 2007;35:33–40.
51. Colson PH, Bernard C, Struck J, Morgenthaler NG, Albat
B, Guillon G. Post cardiac surgery vasoplegia is associated
with high preoperative copeptin plasma concentration. Crit
Care. 2011;15:R255.
52. Hylands M, Toma A, Beaudoin N, et al. Early vasopressor
use following traumatic injury: a systematic review. BMJ
Open. 2017;7:e017559.
53. Collier B, Dossett L, Mann M, et al. Vasopressin use is asso-
ciated with death in acute trauma patients with shock. J Crit
Care. 2010;25:173.e9–173.14.
54. Plurad DS, Talving P, Lam L, Inaba K, Green D, Demetriades
D. Early vasopressor use in critical injury is associated
with mortality independent from volume status. J Trauma.
2011;71:565–570.
55. Fisher AD, April MD, Cunningham C, Schauer SG.
Prehospital vasopressor use is associated with worse
mortality in combat wounded. Prehosp Emerg Care.
2021;25:268–273.
56. Hylands M, Godbout MP, Mayer SK, et al. Vasopressor use
following traumatic injury—a single center retrospective
study. PLoS One. 2017;12:e0176587.
57. Barmparas G, Dhillon NK, Smith EJ, et al. Patterns of vaso-
pressor utilization during the resuscitation of massively
transfused trauma patients. Injury. 2018;49:8–14.
58. Fischer PE, Nunn AM, Wormer BA, et al. Vasopressor use
after initial damage control laparotomy increases risk for
anastomotic disruption in the management of destructive
colon injuries. Am J Surg. 2013;206:900–903.
59. Aoki M, Abe T, Saitoh D, Hagiwara S, Oshima K. Use of
vasopressor increases the risk of mortality in traumatic
hemorrhagic shock: a nationwide cohort study in Japan.
Crit Care Med. 2018;46:e1145–e1151.
60. Uchida K, Nishimura T, Hagawa N, et al. The impact of
early administration of vasopressor agents for the resusci-
tation of severe hemorrhagic shock following blunt trauma.
BMC Emerg Med. 2020;20:26.
61. Inoue T, Manley GT, Patel N, Whetstone WD. Medical and
surgical management after spinal cord injury: vasopressor
usage, early surgerys, and complications. J Neurotrauma.
2014;31:284–291.
62. Dhillon NK, Huang R, Mason R, et al. Vasopressors in trau-
matic brain injury: quantifying their effect on mortality. Am
J Surg. 2020;220:1498–1502.
63. Dharia A, Lacci JV, Gupte N, Sei A. Multiple signicant
trauma with craniotomy: what impacts mortality? Clin
Neurol Neurosurg. 2019;186:105448.
64. Sookplung P, Siriussawakul A, Malakouti A, et al.
Vasopressor use and effect on blood pressure after severe
adult traumatic brain injury. Neurocrit Care. 2011;15:46–54.
65. Readdy WJ, Whetstone WD, Ferguson AR, et al.
Complications and outcomes of vasopressor usage in
acute traumatic central cord syndrome. J Neurosurg Spine.
2015;23:574–580.
66. Ploumis A, Yadlapalli N, Fehlings MG, Kwon BK, Vaccaro
AR. A systematic review of the evidence supporting a
role for vasopressor support in acute SCI. Spinal Cord.
2010;48:356–362.
67. Martin ND, Kepler C, Zubair M, Sayadipour A, Cohen M,
Weinstein M. Increased mean arterial pressure goals after
spinal cord injury and functional outcome. J Emerg Trauma
Shock. 2015;8:94–98.
68. Lloyd-Donald P, Spencer W, Cheng J, et al. In adult patients
with severe traumatic brain injury, does the use of nor-
epinephrine for augmenting cerebral perfusion pressure
improve neurological outcome? A systematic review. Injury.
2020;51:2129–2134.
69. Eastridge BJ, Salinas J, McManus JG, et al. Hypotension
begins at 110 mm Hg: redening “hypotension” with data.
J Trauma. 2007;63:291–297.
70. Gauss T, Gayat E, Harrois A, et al; TraumaBase
Group; Prehospital Traumabase Group Ile de France,
SAMU=Service d’Aide Médicale Urgente. Effect of early
use of noradrenaline on in-hospital mortality in haemor-
rhagic shock after major trauma: a propensity-score analy-
sis. Br J Anaesth. 2018;120:1237–1244.
71. Van Haren RM, Thorson CM, Valle EJ, et al. Vasopressor
use during emergency trauma surgery. Am Surg.
2014;80:472–478.
72. Cohn SM, McCarthy J, Stewart RM, Jonas RB, Dent DL,
Michalek JE. Impact of low-dose vasopressin on trauma
outcome: prospective randomized study. World J Surg.
2011;35:430–439.
73. Sims CA, Holena D, Kim P, et al. Effect of low-dose sup-
plementation of arginine vasopressin on need for blood
product transfusions in patients with trauma and hem-
orrhagic shock: a randomized clinical trial. JAMA Surg.
2019;154:994–1003.
74. Van Haren RM, Thorson CM, Ogilvie MP, et al. Vasopressin
for cerebral perfusion pressure management in patients
with severe traumatic brain injury: preliminary results of
a randomized controlled trial. J Trauma Acute Care Surg.
2013;75:1024–1030.
75. Allen CJ, Subhawong TK, Hanna MM, et al. Does vasopres-
sin exacerbate cerebral edema in patients with severe trau-
matic brain injury? Am Surg. 2018;84:43–50.
76. Yamamoto R, Suzuki M, Hayashida K, et al; SOS-KANTO
2012 Study Group. Epinephrine during resuscitation of
traumatic cardiac arrest and increased mortality: a post hoc
analysis of prospective observational study. Scand J Trauma
Resusc Emerg Med. 2019;27:74.
77. Annane D, Ouanes-Besbes L, de Backer D, et al. A global
perspective on vasoactive agents in shock. Intensive Care
Med. 2018;44:833–846.
78. De Backer D, Pinsky M. Norepinephrine improves car-
diac function during septic shock, but why? Br J Anaesth.
2018;120:421–424.
79. Hamzaoui O, Jozwiak M, Geffriaud T, et al. Norepinephrine
exerts an inotropic effect during the early phase of human
septic shock. Br J Anaesth. 2018;120:517–524.
80. Holmes CL, Landry DW, Granton JT. Science review: vaso-
pressin and the cardiovascular system part 2—clinical
physiology. Crit Care. 2004;8:15–23.
81. Bown LS, Ricksten SE, Houltz E, et al. Vasopressin-induced
changes in splanchnic blood ow and hepatic and portal
venous pressures in liver resection. Acta Anaesthesiol Scand.
2016;60:607–615.
82. Colucci G, Stutz M, Rochat S, et al. The effect of desmopres-
sin on platelet function: a selective enhancement of proco-
agulant COAT platelets in patients with primary platelet
function defects. Blood. 2014;123:1905–1916.

Copyright © 2021 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
E
NARRATIVE REVIEW ARTICLE
July 2021
•
Volume 133
•
Number 1 www.anesthesia-analgesia.org 79
83. Mei Q, Liang BT. P2 purinergic receptor activation enhances
cardiac contractility in isolated rat and mouse hearts. Am J
Physiol Heart Circ Physiol. 2001;281:H334–H341.
84. Dutton RP. Haemostatic resuscitation. Br J Anaesth.
2012;109(suppl 1):i39–i46.
85. Holcomb JB, Tilley BC, Baraniuk S, et al; PROPPR Study
Group. Transfusion of plasma, platelets, and red blood
cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients
with severe trauma: the PROPPR randomized clinical trial.
JAMA. 2015;313:471–482.
86. Duchesne JC, Barbeau JM, Islam TM, Wahl G, Greiffenstein
P, McSwain NE Jr. Damage control resuscitation: from
emergency department to the operating room. Am Surg.
2011;77:201–206.
87. Bickell WH, Wall MJ Jr, Pepe PE, et al. Immediate versus
delayed uid resuscitation for hypotensive patients with
penetrating torso injuries. N Engl J Med. 1994;331:1105–1109.
88. Guyette FX, Brown JB, Zenati MS, et al. Tranexamic acid
during prehospital transport in patients at risk for hemor-
rhage after injury: a double-blind, placebo-controlled, ran-
domized clinical trial. JAMA Surg. 2020;156:11–20.
89. Harvin JA, Peirce CA, Mims MM, et al. The impact of
tranexamic acid on mortality in injured patients with hyper-
brinolysis. J Trauma Acute Care Surg. 2015;78:905–909.
90. Khan M, Jehan F, Bulger EM, et al; PROPPR Study Group.
Severely injured trauma patients with admission hyper-
brinolysis: is there a role of tranexamic acid? Findings from
the PROPPR trial. J Trauma Acute Care Surg. 2018;85:851–857.
91. Carrick MM, Morrison CA, Tapia NM, et al. Intraoperative
hypotensive resuscitation for patients undergoing lapa-
rotomy or thoracotomy for trauma: early termination of a
randomized prospective clinical trial. J Trauma Acute Care
Surg. 2016;80:886–896.
92. Schreiber MA, Meier EN, Tisherman SA, et al; ROC
Investigators. A controlled resuscitation strategy is feasible
and safe in hypotensive trauma patients: results of a pro-
spective randomized pilot trial. J Trauma Acute Care Surg.
2015;78:687–695.
93. Dutton RP, Mackenzie CF, Scalea TM. Hypotensive resus-
citation during active hemorrhage: impact on in-hospital
mortality. J Trauma. 2002;52:1141–1146.
94. Walsh M, Devereaux PJ, Garg AX, et al. Relationship
between intraoperative mean arterial pressure and clinical
outcomes after noncardiac surgery: toward an empirical
denition of hypotension. Anesthesiology. 2013;119:507–515.
95. Salmasi V, Maheshwari K, Yang D, et al. Relationship
between intraoperative hypotension, dened by either
reduction from baseline or absolute thresholds, and acute
kidney and myocardial injury after noncardiac surgery: a
retrospective cohort analysis. Anesthesiology. 2017;126:47–65.
96. Hess JR, Brohi K, Dutton RP, et al. The coagulopathy of
trauma: a review of mechanisms. J Trauma. 2008;65:748–754.
97. Tisherman SA, Schmicker RH, Brasel KJ, et al. Detailed
description of all deaths in both the shock and traumatic
brain injury hypertonic saline trials of the resuscitation
outcomes consortium. Ann Surg. 2015;261:586–590.
98. Janak JC, Mazuchowski EL, Kotwal RS, et al. Patterns of
anatomic injury in critically injured combat casualties: a
network analysis. Sci Rep. 2019;9:13767.
99. Wilson MH. Traumatic brain injury: an underappreciated
public health issue. Lancet Public Health. 2016;1:e44.
100. Foulon P, De Backer D. The hemodynamic effects of nor-
epinephrine: far more than an increase in blood pressure!
Ann Transl Med. 2018;6:S25.
101. Repessé X, Charron C, Fink J, et al. Value and determinants
of the mean systemic lling pressure in critically ill patients.
Am J Physiol Heart Circ Physiol. 2015;309:H1003–H1007.
102. Beloncle F, Meziani F, Lerolle N, Radermacher P, Asfar P.
Does vasopressor therapy have an indication in hemor-
rhagic shock? Ann Intensive Care. 2013;3:13.
103. Maegele M, Lefering R, Sakowitz O, et al. The incidence
and management of moderate to severe head injury. Dtsch
Arztebl Int. 2019;116:167–173.
104. Wiles MD. Blood pressure in trauma resuscitation: ‘pop the
clot’ vs. ‘drain the brain’? Anaesthesia. 2017;72:1448–1455.
105. Tobin JM, Dutton RP, Pittet JF, Sharma D. Hypotensive
resuscitation in a head-injured multi-trauma patient. J Crit
Care. 2014;29:313.e1–313.e5.
106. Liu L, Tian K, Xue M, et al. Small doses of arginine vaso-
pressin in combination with norepinephrine “buy” time
for denitive treatment for uncontrolled hemorrhagic
shock in rats. Shock. 2013;40:398–406.
107. Lee JH, Kim K, Jo YH, et al. Early norepinephrine infu-
sion delays cardiac arrest after hemorrhagic shock in rats.
J Emerg Med. 2009;37:376–382.
108. Dalibon N, Schlumberger S, Saada M, Fischler M, Riou B.
Haemodynamic assessment of hypovolaemia under gen-
eral anaesthesia in pigs submitted to graded haemorrhage
and retransfusion. Br J Anaesth. 1999;82:97–103.
109. Oren-Grinberg A, Talmor D, Brown SM. Focused critical
care echocardiography. Crit Care Med. 2013;41:2618–2626.
110. Ferrada P, Evans D, Wolfe L, et al. Findings of a random-
ized controlled trial using limited transthoracic echocar-
diogram (LTTE) as a hemodynamic monitoring tool in the
trauma bay. J Trauma Acute Care Surg. 2014;76:31–37.
111. Leichtle SW, Singleton A, Singh M, Griffee MJ, Tobin
JM. Transesophageal echocardiography in the evalu-
ation of the trauma patient: a trauma resuscitation
transesophageal echocardiography exam. J Crit Care.
2017;40:202–206.
112. Shea SM, Staudt AM, Thomas KA, et al. The use of low-
titer group O whole blood is independently associated
with improved survival compared to component therapy
in adults with severe traumatic hemorrhage. Transfusion.
2020;60(suppl 3):S2–S9.
113. Abramson D, Scalea TM, Hitchcock R, Trooskin SZ, Henry
SM, Greenspan J. Lactate clearance and survival following
injury. J Trauma. 1993;35:584–588.
114. Odom SR, Howell MD, Silva GS, et al. Lactate clearance as
a predictor of mortality in trauma patients. J Trauma Acute
Care Surg. 2013;74:999–1004.
115. Régnier MA, Raux M, Le Manach Y, et al. Prognostic sig-
nicance of blood lactate and lactate clearance in trauma
patients. Anesthesiology. 2012;117:1276–1288.
116. Zhang Z, Xu X. Lactate clearance is a useful biomarker
for the prediction of all-cause mortality in critically ill
patients: a systematic review and meta-analysis*. Crit Care
Med. 2014;42:2118–2125.
