
DELIVERED BY WOMEN,
LED BY MEN:
A GENDER AND EQUITY ANALYSIS
OF THE GLOBAL HEALTH AND
SOCIAL WORKFORCE
Human Resources for Health Observer Series No. 24

DELIVERED BY WOMEN,
LED BY MEN:
A GENDER AND EQUITY ANALYSIS
OF THE GLOBAL HEALTH AND
SOCIAL WORKFORCE
Human Resources for Health Observer Series No. 24
Delivered by women, led by men: A gender and equity analysis of the global health and social workforce.
(Human Resources for Health Observer Series No. 24)
ISBN 978-92-4-151546-7
© World Health Organization 2019
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO;
https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as
indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the
WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create
a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health
Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic
edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property
Organization.
Suggested citation. Delivered by women, led by men: A gender and equity analysis of the global health and social workforce.
Geneva: World Health Organization; 2019 (Human Resources for Health Observer Series No. 24). Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on
rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your
responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from
infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion
whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its
frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference
to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital
letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being
distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In
no event shall WHO be liable for damages arising from its use.
Design by Blossom.
Layout by L’IV Com Sàrl, Villars-sous-Yens, Switzerland.
Printed in Switzerland

Contents
Foreword: Women in Global Health as co-chair of Gender
Equity Hub
............................................................... vi
Acknowledgements .................................................... vii
Abbreviations .......................................................... viii
Executive summary ..................................................... 1
Key findings from the four thematic areas of the review ........................... 1
Overarching findings and conclusions from the review ............................ 1
Key messages from this review .............................................. 3
Key recommendations ...................................................... 4
Section 1. Approach .................................................... 5
Chapter 1. Introduction ................................................. 5
1.1 Background ........................................................... 5
1.2 Gender Equity Hub (GEH) ................................................ 9
1.3 Rationale for gender analysis on the health workforce ........................ 9
Chapter 2. Objectives and methodology ........................... 11
2.1 Objectives .......................................................... 11
2.2 Methodology ......................................................... 11
2.3 Limitations ........................................................... 12
Section 2. Key findings ................................................ 13
Chapter 3. Occupational segregation ................................ 13
3.1 Key messages ........................................................ 13
3.2 Occupational segregation: literature review ................................ 13
3.3 Occupational segregation by gender in the global health workforce ............ 18
3.4 Factors that lead to occupational segregation .............................. 20
3.5 Why occupational segregation matters .................................... 20
iii

Chapter 4. Decent work without discrimination, bias and sexual
harassment
............................................................. 24
4.1 Key messages ........................................................ 24
4.2 Decent work: introduction .............................................. 24
4.3 Decent work in the global health workforce ................................ 25
4.4 Discrimination ........................................................ 25
4.5 Bias ................................................................ 26
4.6 Sexual harassment .................................................... 26
4.7 Why addressing decent work in the global health workforce matters ............ 28
Chapter 5. Gender pay gap ........................................... 29
5.1 Key messages ........................................................ 29
5.2 Gender pay gap: introduction and background ............................. 29
5.3 The gender pay gap in the global health workforce .......................... 31
5.4 Factors that contribute to gender pay gaps ................................ 32
5.5 Why is addressing the gender pay gap in the global health workforce important? .. 33
Chapter 6. Leadership ................................................. 36
6.1 Key messages ........................................................ 36
6.2 Leadership and gender: background ...................................... 36
6.3 Leadership and governance in the global health and workforce ................ 36
6.4 Why addressing gender gaps in leadership matters .......................... 39
6.5 Factors contributing to leadership gaps in the global health workforce ........... 39
Section 3. Conclusions ................................................ 42
Chapter 7. Conclusions: policy context, findings, and next steps . 42
7.1 Policy context ........................................................ 42
7.2 Findings of the GEH literature review ...................................... 43
7.3 Next steps ........................................................... 45
Glossary ................................................................. 46
References ............................................................ 49
Annex 1. Membership of the Gender Equity Hub in the Global
Health Workforce Network
........................................ 59
Annex 2. Literature matrix ............................................ 60
A literature review
iv

Boxes
Box 1.1 Global Health Workforce Network Gender Equity Hub: priority areas ................................... 9
Box 1.2 Global Health Workforce Network Gender Equity Hub: five key activities
................................. 9
Box 3.1 Individual factors contributing to gender segregation
............................................. 21
Box 3.2 Organizational factors contributing to gender segregation
......................................... 21
Box 3.3 Societal factors contributing to gender segregation
.............................................. 22
Box 4.1 Origin of the #MeToo movement
........................................................... 28
Box 5.1 Factors contributing to gender pay gaps: key themes
............................................ 34
Box 6.1 Individual, household and community dimensions of gender stereotyping
.............................. 41
Box 7.1 Working for Health: five-year action plan for health employment and inclusive economic growth 2017–2021
(WHO, ILO, OECD)
........................................................................... 42
Figures
Figure ES.1 Key findings of GEH review of female health workforce, by thematic area ......................... 2
Figure ES.2 Overarching findings and conclusions of review
............................................ 2
Figure 1.1 Share of women employed in the health and social sectors compared to share of women employed in all
sectors by ILO region, 2013
.................................................................... 6
Figure 1.2 Sustainable Development Goals
......................................................... 7
Figure 1.3 Health workforce and gender: a theory of change
............................................ 8
Figure 1.4 Working for Health programme: a global movement for gender-transformative workforce development
..... 8
Figure 3.1 Women’s share of selected occupations (2012)
............................................ 14
Figure 3.2 Share of female doctors by OECD country (2015)
........................................... 15
Figure 3.3 Male and female employment (%) in health and education sectors (2015)
......................... 15
Figure 3.4 Average work day and unpaid work, men and women
........................................ 16
Figure 3.5 Paid and unpaid work (minutes per day) for men and women, by OECD country
.................... 16
Figure 3.6 Financial value of women’s contribution to the global health system, as part of global GDP
............ 17
Figure 3.7 The cycle of unpaid care work–paid work–paid care work
..................................... 18
Figure 3.8 United States share of nurses who are male (1970–2011)
.................................... 19
Figure 3.9 Percentage of economies that restrict women’s employment, by type of restriction
.................. 19
Figure 3.10 Do organizations have workplace gender policies?
......................................... 23
Figure 4.1 Percentage of United States medical academics reporting sexual harassment
...................... 26
Figure 4.2 Inadequacy of global sexual harassment laws
.............................................. 27
Figure 5.1 Equal pay versus the gender pay gap
.................................................... 29
Figure 5.2 Gender wage gap by country
.......................................................... 31
Figure 5.3 Female earnings as a percentage of men’s earnings among full-time, year-round nurses (2011)
........ 32
Figure 6.1 Who leads global health organizations?
.................................................. 37
Figure 6.2 Percentage of Member State ministries of health headed by women, by WHO region
................. 38
Figure 6.3 Women’s representation at World Health Assembly, 2005–2015
................................ 38
Figure 6.4 Global health leadership pyramid
....................................................... 39
Figure 7.1 Key finding in four focus areas of GEH literature review
...................................... 43
Figure 7.2 Key overarching findings of GEH literature review
........................................... 44
v

Foreword: Women in Global Health as
co-chair of Gender Equity Hub
On behalf of Women in Global Health I am delighted to receive this important report and acknowledge the many expert partners who gave their
time to generate the evidence that will underpin gender equality in health, and therefore better global health.
When I graduated as a medical doctor I knew I was standing on the shoulders of the pioneer women who had fought their way into medicine and
carved a path for me and other women. In some countries this is very recent history, since women did not qualify as doctors until the 1940s.
Today women account for 70% of the health and social care workforce and deliver care to around 5 billion people. But as this report shows,
despite progress, women remain largely segregated into lower-status and lower-paid jobs in health, are subject to discrimination, and, in some
contexts, are under the constant threat of violence. Global health is delivered by women and led by men, and that is neither fair nor smart.
Large numbers of women in health are working without the protection of legislation to guarantee them decent work and equal pay. Many are
underpaid or unpaid. The gender pay gap in the health sector is higher than other sectors despite it being a female-majority profession.
Disadvantage is multiplied by the intersection of gender with race, ethnicity, caste, or religion – depending where you are in the world.
We cannot wait for the global health system to correct its own course. Approximately 40 million new health and social care jobs will be needed
by 2030 to keep up with changing demographics and increased demand for health. Around 18 million health and social care jobs must be
filled in low-income countries to reach the Sustainable Development Goals (SDGs) and achieve the game-changing ambition of universal health
coverage. Gender-transformative change is needed to stop the leakage in the pipeline and loss of female ideas and talent. Similarly, we want to
increase male talent and perspectives in fields such as nursing where men are underrepresented.
Doing things differently by addressing gender inequities in global health and investing in the global health and social workforce will have a wider
multiplier effect, offering a “triple gender dividend” comprising the following.
• Health dividend. We can fill the millions of new jobs that must be created to meet growing demand and reach universal health coverage and
the health-related SDGs by 2030.
• Gender equality dividend. Investment in women and the education of girls to enter formal, paid work will increase gender equality and
women’s empowerment as women gain income, education and autonomy. In turn, this is likely to improve family education, nutrition,
women’s and children’s health, and other aspects of development.
• Development dividend. New jobs will be created, fuelling economic growth.
This gender dividend, once realized, will improve the health and lives of people everywhere. The health and social care worker shortage is
global. This is everybody’s business.
As co-chair of the Gender Equity Hub with WHO, Women in Global Health are pleased to work in the vanguard with WHO and our partners to
catalyse gender-transformative policy change for better global health.
Dr Roopa Dhatt
Co-chair of the Gender Equity Hub
Executive Director and co-founder of Women in Global Health
A literature review
vi

The lead authors and primary editors of this report are Mehr Manzoor, Research Director at Women in Global Health and a PhD candidate at
Tulane University, and Kelly Thompson, Programming and Gender Director at Women in Global Health and co-chair of the Gender Equity Hub.
Additional authors and editors are Ann Keeling, Senior Policy Adviser at Women in Global Health, and Roopa Dhatt, Executive Director at Women
in Global Health.
They worked under the close guidance of Tana Wuliji, Technical Officer for Health Workforce at WHO and co-chair of the Gender Equity Hub, and
Paul Marsden, Technical Officer for Health Workforce at WHO and acting co-chair of the Gender Equity Hub, as well as colleagues at Women
in Global Health who supported the project in many ways. We acknowledge the support and feedback provided by Temitayo Ifafore-Calfee,
Operations Director at Women in Global Health. They provided thought leadership, editorial advice and operational support for the development
of this report. We acknowledge editorial and graphic support by Christina Memmott, Graduate Student at Johns Hopkins University.
Extensive expert technical guidance was provided by Constance Newman, Senior Team Leader, Gender Equality and Health, Intrahealth
International. She provided extensive support and mentorship in the development of this paper and served as a constant source of expertise and
encouragement.
Over the course of the project several technical consultations were sought to seek relevant literature, input and feedback to strengthen the
report and its findings on the main theme of gender and equity within the global health workforce.
Gender Equity Hub members provided support and valuable feedback, including Lina Bader, Research and Evaluation Consultant at the
International Pharmaceutical Federation, who provided extensive support in evidence extraction and writing. Zahra Zeinali, Graduate Research
Assistant at Johns Hopkins University, provided key input on intersectionality. Extensive feedback was provided by Myra Betron, Director of
Gender at Jhpiego; Jennifer Breads, Technical Adviser in the Global Learning Office at Jhpiego; Professor Ivy Bourgeault, Professor at University
of Ottawa; Samantha Law, Manager at Chemonics; Tracy McClair, Jhpiego; Rosemary Morgan, Assistant Scientist at Johns Hopkins University
and Research in Gender and Ethics; Rosie Steege, Research in Gender and Ethics; and Samantha Rick, Deputy Director of the Frontline Health
Workers Coalition and Advocacy and Policy Officer at IntraHealth International.
External experts from international organizations and universities provided their generous support, guidance and feedback throughout the
development of this report. We would like to thank Ana Langer, Professor and Director of the Women and Health Initiative at Harvard University;
Jacquelyn Caglia, Assistant Director of the Women and Health Initiative at Harvard University; Ashveena Gajeele, Global Access in Action Fellow
at the Berkman Center for Internet and Society at Harvard University; Kate Hawkins, Research in Gender and Ethics; Rohina Joshi, Senior
Research Fellow at The George Institute for Global Health; Devaki Nambiar, Program Head–Health Systems and Equity at the George Institute
for Global Health; Ana Barata, USF Amora Saudável; Sara Causev, Women in Global Health Sweden Chapter; Kathleen Fenton, Paediatric and
Congenital Cardiac Surgeon at Cardiac Alliance; Isabelle Fox, Director of Surgical Missions at Mending Kids; Niyati Shah, Senior Gender Adviser
and Team Leader at USAID; and Geordan Shannon, Medical Doctor and Researcher at University College London.
Submissions of evidence and policy and practice experience were provided by Steven Buzuzi, ReBUILD Consortium; Mehr Manzoor, Women
in Global Health; Isabelle Carr, Australia Medical Students’ Association; Abigail Donner, Abt Associates; Vince Blaser, Frontline Health Workers
Coalition; Yvonne Commodore-Mensah, African Research Academies for Women; Neeru Gupta, University of New Brunswick; Mary Beth
Hastings, Iris Group; Carolina Haylock-Loor, Kirthi Jayakumar, Red Elephant Foundation; Estelle Kouokam, Countdown; Sandra Massiah, Public
Services International; Sarah McKee, Management Sciences for Health; Emma Nofal, Athena Swan NHS Fellow; Ema Paulino, International
Pharmaceutical Federation; Viktor Siebert, German Development Cooperation (GIZ); Marion Subah, Jhpiego; Sally Theobald, Liverpool School of
Tropical Medicine; Nupoor Tomar, Monash University; Sreytouch Vong, ReBUILD Consortium; and Sophie Witter, ReBUILD Consortium.
The report was commissioned by the World Health Organization.
Acknowledgements
vii

AFRO WHO Regional Office for Africa
EMRO WHO Regional Office for Eastern-Mediterranean
EURO WHO Regional Office for Europe
G7 Group of Seven
GDP gross domestic product
GEH Gender Equity Hub
ILO International Labour Organization
OECD Organisation for Economic Co-operation and Development
PAHO Pan American Health Organization
SDG Sustainable Development Goal
SEARO WHO Regional Office for South East Asia
WHO World Health Organization
WPRO WHO Regional Office for the Western Pacific
Abbreviations
A literature review
viii

Demographic changes and rising health care demands are projected
to drive the creation of 40 million new jobs by 2030 in the global
health and social sector. In parallel, there is an estimated shortfall
of 18 million health workers, primarily in low- and middle-income
countries, required to achieve the Sustainable Development Goals
(SDGs) and universal health coverage. The global mismatch between
health worker supply and demand is both a cause for concern and a
potential opportunity. Since women account for 70% of the health and
social care workforce, gaps in health worker supply will not be closed
without addressing the gender dynamics of the health and social
workforce. The female health and social care workers who deliver
the majority of care in all settings face barriers at work not faced by
their male colleagues. This not only undermines their own well-being
and livelihoods, it also constrains progress on gender equality and
negatively impacts health systems and the delivery of quality care.
In November 2017, the World Health Organization (WHO) established
the Gender Equity Hub (GEH), co-chaired by WHO and Women in
Global Health under the umbrella of the Global Health Workforce
Network. The GEH brings together key stakeholders to strengthen
gender-transformative policy guidance and implementation capacity
for overcoming gender biases and inequalities in the global health
and social workforce, in support of the implementation of the Global
Strategy on Human Resources for Health: Workforce 2030, and the
Working for Health five-year action plan (2017–2021) of WHO, the
International Labour Organization (ILO) and the Organisation for
Economic Co-operation and Development (OECD).
In 2018, the GEH identified and reviewed over 170 studies in a
literature review of gender and equity in the global health workforce,
with a focus on four themes: occupational segregation; decent work
free from bias, discrimination and harassment, including sexual
harassment; gender pay gap; and gender parity in leadership.
This report will inform the next phase of the work of the Global Health
Workforce Network GEH, which seeks to use these research findings
to advocate gender-transformative policy and action.
Executive summary
Key findings from the four thematic
areas of the review
The key findings in each of the four thematic areas covered by the
GEH review are summarized in Figure ES.1 and covered in detail in
Chapters 3–6 of this report.
Overarching findings and conclusions
from the review
In addition, the report identified eight overarching findings and
conclusions, summarized in Figure ES.2 and further elaborated in the
text below.
• Most of the 170 studies found and reviewed in this report come
from anglophone high-income country contexts and are unlikely to
be applicable to other contexts.
• There are gaps in data and research from all regions but the
most serious gaps are in low- and middle-income countries. This
is a major concern, since the most rapid progress in health is
needed in low- and middle-income countries to reach the SDGs,
attain universal health coverage and achieve the health for all
targets by 2030.
• Widespread gaps in the data and literature were found in countries
of all income levels on implementation research, application of
gender-transformative policy measures, and good practice on
addressing health system deficiencies caused by gender inequality.
• Major gaps and lack of comparable data were found in countries
from all regions. Examples include sexual harassment and gender
pay gap data.
• Studies were limited in methodological approaches. Few used an
intersectional approach to examine how gender disadvantage in
the health workforce can be compounded by other social identities
such as race and class.
1

Figure ES.1 Key findings of GEH review of female health workforce, by thematic area
Figure ES.2 Overarching findings and conclusions of review
Horizontal and vertical occupational segregation by gender is a
universal pattern in health, varies with context.
Driven by gender norms and stereotypes of jobs culturally labelled
‘men’s’ or ‘women’s’ work
Gender discrimination constrains women’s leadership/seniority
Gender stereotypes constrain men eg entering nursing
Women in health typically clustered into lower status/lower paid
jobs
Female majority professions given lower social value, status & pay
Women are 70% global health workforce but hold only 25% senior
roles
Gender leadership gaps driven by stereotypes, discrimination, power
imbalance, privilege
Women’s disadvantage intersects with/multiplied by other identities eg
race, class
Global health weakened by loss female talent, ideas, knowledge
Women leaders often expand health agenda, strengthening health for all
Gendered leadership gap in health is a barrier to reaching SDGs and UHC
Large % women in health workforce face bias and discrimination
Female health workers face burden sexual harassment causing
harm, ill health, attrition, loss morale, stress
Many countries lack laws and social protection that are the
foundation for gender equality at work
Male healthworkers more likely to be organised in trade unions
than female
Frontline female healthworkers in conflict/emergencies/remote
areas face violence, injury & death
GPG in health 26-26%, higher than average for other sectors
Most of GPG in health is unexplained by observable factors eg
education
Occupational segregation, women in lower status/paid roles, drives GPG.
Much of women’s work health/social care unpaid and excluded in GPG
data
Equal pay laws and collective bargaining absent in many countries
GPG leads to lifetime economic disadvantage for women
Closing GPG essential to reaching SDGs
OCCUPATIONAL
SEGREGATION LEADERSHIP
DECENT WORK:
DISCRIMINATION SEXUAL
HARASSMENT BIAS
GENDER PAY GAP (GPG)
OCCUPATIONAL
SEGREGATION LEADERSHIP
DECENT WORK:
DISCRIMINATION SEXUAL
HARASSMENT BIAS
GENDER PAY
GAP (GPG)
Overarching Findings from literature review:
• 170 studies in this review, most from global North
• Major gaps in data and research from low- and middle-income countries (LMICs) on
gender and equity dimensions health workforce
• Major gaps in implementation research on impact of policy change or gender
transformative approaches in different cultural settings
• Major gaps in data in all areas, particularly sexual harassment and data comparable
across countries on the gender pay gap
• Studies limited in methodological approaches. Very few adopt an intersectionality
lens or use mixed methods approaches
• Occupational segregation, vertical and horizontal, is major driver and consequence
of gender inequality
• Critical role of women in health (70% health workforce) is often overlooked, so
priority not given to addressing gender/equity in workforce
• Gender inequality in health and social care workforce will limit delivery of UHC &
health for all
A literature review
2

• Occupational segregation by gender in the health sector, driven
by gender inequality, is pronounced, and in turn is the foundation
for other gender inequalities identified in this report (such as the
gender pay gap). Although women hold around 70% of jobs in
the health workforce they remain largely segregated vertically,
with men holding the majority of higher-status roles. Female
health workers are clustered into lower-status and lower-paid
(often unpaid) roles and are further disadvantaged by horizontal
occupational segregation driven by gender stereotypes branding
some jobs suitable for women (nursing) or men (surgery). Women
are triply disadvantaged by social gender norms that attach
lower social value to majority female professions, which, in turn,
devalues the status and pay of those professions.
• Despite women being the majority of the global health and
social workforce, the role of women as drivers of health is often
unacknowledged. This contributes to a lack of priority given to
addressing gender inequality in the health and social workforce.
Gender-transformative policies and measures must be put in
place if global targets such as universal health coverage are to be
achieved. Also largely unacknowledged is the burden of unpaid
health and social care work typically done by women and girls.
Women’s unpaid work forms an insecure foundation for global
health.
• A key conclusion of this report is that gender inequality in the
health and social workforce weakens health systems and health
delivery. These gender inequities, however, can be fixed, and an
alternative, positive future scenario is possible.
Adopting gender-transformative policies, addressing gender inequities
in global health, and investing in decent work for the female health
workforce offer a wider social and economic multiplier – a “triple
gender dividend” – comprising the following.
• Health dividend. The millions of new jobs in health and social
care needed to meet growing demand, respond to demographic
changes and deliver universal health coverage by 2030 will be
filled.
• Gender equality dividend. Investment in women and the education
of girls to enter formal, paid work will increase gender equality
and women’s empowerment as women gain income, education
and autonomy. In turn, this is likely to improve family education,
nutrition, women and children’s health, and other aspects of
development.
• Development dividend. New jobs will be created, fuelling
economic growth.
This triple gender dividend will improve the health and lives of people
everywhere. The health and social care worker shortage is global, and
addressing gender inequality in the health workforce is everybody’s
business.
Key messages from this review
The following key messages emerged from this review.
• In general, women deliver global health and men lead it.
Progress on gender parity in leadership varies by country and
sector, but generally men hold the majority of senior roles in health
from global to community level. Global health is predominantly led
by men: 69% of global health organizations are headed by men,
and 80% of board chairs are men. Only 20% of global health
organizations were found to have gender parity on their boards,
and 25% had gender parity at senior management level. Health
systems will be stronger when the women who deliver them have
an equal say in the design of national health plans, policies and
systems.
• Workplace gender biases, discrimination and inequities are
systemic, and gender disparities are widening. In 2018 it was
estimated that workplace gender equality was 202 years away –
longer than 2016 estimates. Many organizations expect female
health workers to fit into systems designed for male life patterns
and gender roles (with, for example, no paid maternity leave), and
many countries still lack laws on matters that underpin gender
equality and dignity at work, such as sex discrimination, sexual
harassment, equal pay and social protection.
• Women in global health are underpaid and often unpaid. It is
estimated that women in health contribute 5% to global gross
domestic product (GDP) (US$ 3 trillion), out of which almost 50%
is unrecognized and unpaid. The World Economic Forum Global
gender gap report 2018 estimates the average gender pay gaps by
country at around 16%. The unadjusted gender pay gap appears
to be even higher in the health and social care sector, estimated at
26% in high-income countries and 29% in upper middle-income
countries. The gender pay gap in men’s favour is nearly universal
and largely unexplained. It has a lifelong economic impact for
women, contributing to poverty in old age. In sectors that are
female dominated, work is typically undervalued and lower paid.
• Workplace violence and sexual harassment in the health and
social sector are widespread and often hidden. Female health
workers face sexual harassment from male colleagues, male
3

patients and members of the community. It is often not recorded,
and women may not report it due to stigma and fear of retaliation.
Violence and harassment harms women, limits their ability to
do their job, and causes attrition, low morale and ill-health. In
Rwanda, female health workers experience much higher rates of
sexual harassment than male colleagues, and in Pakistan, lady
health workers have reported harassment from both management
and lower-level male staff.
• Occupational segregation by gender is deep and universal.
Women dominate nursing and men dominate surgery (horizontal
segregation). Men dominate senior, higher-status, higher-paid
roles (vertical segregation). Wider societal gender norms and
stereotypes reinforce this. Occupational segregation by gender
drives the gender pay gap and leads to loss of talent (for example,
with few men entering nursing).
Key recommendations
• It is time to change the narrative. Women, as the majority of the
global health and social care workforce, are the drivers of global
health. Research and policy dialogues on gender and global health
to date have neglected this reality and have focused on women’s
health and women’s access to health (both vitally important). It is
critical to record and recognize all the work women do in health
and social care – paid and unpaid – and bring unpaid health and
care work into the formal labour market. Women form the base of
the pyramid on which global health rests and should be valued as
change agents of health, not victims.
• Gender-transformative policies should be adopted that
challenge the underlying causes of gender inequities. Such
policies are essential to advancing gender equality in the health
and social workforce. Adding jobs to the health workforce under
current conditions will not solve the gender inequities that
exacerbate the health worker shortage, contributing to a mismatch
of supply and demand and wasted talent. Policies to date have
attempted to fix women to fit into inequitable systems; now we
need to fix the system and work environment to create decent
work for women and close gender gaps in leadership and pay.
• The focus of research in the global health and social workforce
should be shifted. Research priorities must prioritize low- and
middle-income countries; apply a gender and intersectionality
lens; include sex- and gender-disaggregated data; and include
the entire health and social workforce, including the social care
workforce. Research must go beyond describing the gender
inequities to also evaluate the impact of gender-transformative
interventions. Such research will aid understanding of context-
specific factors, including sociocultural dimensions. Moreover,
research focused on implementation and translation into policy
is needed to assess the viability and effectiveness of policies and
inform gender-transformative policy action.
• A mid-plan review should be aligned with the independent
review of the Working for Health five-year action plan for health
employment and inclusive economic growth (2017–2021) and
the medium-term fiscal plan that is to be carried out in 2019
to mark the midpoint in the five-year action plan. This proposed
review would involve WHO, ILO and OECD, assess progress on
deliverables on gender equality, and recommend steps to ensure
delivery of action plan commitments by 2021.
A literature review
4

1.1 Background
At present, over 234 million workers staff the health and social care
sector globally (1). The health and social care sector is the fastest
growing employment sector for women, with women comprising seven
out of ten health and social care workers (1).
On average, the share of women working in the
health and social care sector is nearly twice
their share of the total workforce. Although
the proportion of women in the workforce has
steadily risen in the last quarter of a century,
industry segregation patterns persist. In 2013,
while the proportion of women in the workforce
worldwide was only 39.5%, the proportion of women employed by
the global health and social sectors amounted to 70.3%. Figure 1.1
provides a breakdown of female employment in the health and social
sectors compared to the workforce as a whole across global regions (1).
As the main providers of health, women deliver health care to around
5 billion people globally and contribute US$ 3 trillion annually to
global health (2). However, approximately half of this contribution is
in the form of unpaid care work (2). The reduction of mortality rates
across all age groups over the past half century is largely due to the
underrecognized contribution of women to health and social care
(3, 4). This report highlights a critical opportunity to address the gaps
in our understanding of the challenges posed by gender inequality
in the global health workforce. Gender analysis in global health has
primarily focused on the point of service delivery and quality of care.
This has largely ignored the fact that women are not only recipients of
health care but are the primary drivers of health globally. This report
aims to move forward the agenda of gender equality in the global
health workforce. We recognize, however, significant gaps in research
and data, particularly from low- and middle-income countries, that
limit our evidence and conclusions.
It is essential to understand the gender-related trends and dynamics
in the health workforce if we are to build resilient health systems and
SECTION 1. APPROACH
Chapter 1. Introduction
achieve universal health coverage (2). Despite global momentum and
progress on gender equality, systemic challenges, gender biases, and
inequities persist in the global health workforce, predominantly to
the disadvantage of women. The women who run health systems do
not have an equal say with men in their design and delivery. These
significant challenges have been linked to health system inefficiencies
that impact the health worker training and supply pipeline,
recruitment, deployment, retention, and attrition, and contribute to
health workforce distribution imbalances between the formal and
informal health workforce, as well as between the public and private
sectors (5). As a result of women in the health workforce being largely
clustered into lower-status and underpaid (or unpaid) jobs, health
systems lose female talent, perspectives and morale.
It is essential to understand the gender-related trends and
dynamics in the health workforce if we are to build resilient
health systems and achieve universal health coverage
The women who are employed in global health are working in very
diverse health systems, settings and socioeconomic contexts. In
general, the current inequality between men and women in the health
workforce globally reflects the following.
• Women’s employment rights in many countries are not protected
by legislation governing critical areas such as equal pay for equal
work, non-discrimination and collective bargaining.
WOMEN COMPRISE 7 OUT OF 10 SOCIAL
HEALTH CARE WORKERS
5

• Medicine was established as a male-only profession and it has
taken time for women to overcome discrimination against their
entry to the profession, senior posts and better-paid specialisms.
• Unequal access of girls to education in many low- and middle-
income countries, particularly to secondary schooling, has limited
their access to training for formal health sector jobs.
• Gender stereotypes and norms common to all societies have
driven occupational segregation, sorting men and women into
different kind of jobs. For example, nursing is predominantly a
women’s job with men accounting for only 10% of those entering
the profession, whereas men hold the majority of jobs in surgical
specialties.
• Health systems and work conditions have been established to suit
men’s life patterns and not women’s; for example, many health
workers have no paid parental leave entitlement.
• Female health workers face a burden of bias, discrimination,
sexual harassment and violence not faced by their male
counterparts, and often not recorded or addressed.
• There is a lack of data and research to highlight gender gaps in
critical areas and to drive accountability and policy change.
• Political will and incentives are lacking for politicians and decision-
makers in health systems to adopt the gender-transformative
leadership and measures necessary to drive equality among
people of different genders, and among other marginalized
identities based on race, caste, class, ethnicity or religion.
All these factors have been obstacles to gender equality in the health
workforce.
According to projections of the World Health Organization (WHO)
Global Strategy on Human Resources for Health (6) and the World
Bank, 40 million new jobs in health and social care will be created
globally by 2030 to meet rising demand driven by demographic
changes, while a shortfall of 18 million health workers will need to
be addressed, primarily in low- and lower middle-income countries,
by 2030 to enable countries to reach the Sustainable Development
Goals (SDGs) and achieve universal health coverage (7, 8). To
address this shortfall, major investments in the health workforce and
acknowledgement of women’s contributions as drivers of health care
are needed. The WHO SDG Health Price Tag study estimates that
investments of US$ 3.9 trillion are needed by 2030 to increase the
prospects of achieving the health-related SDGs (investing US$ 51 per
capita in upper middle-income countries, US$ 58 per capita in lower
middle-income countries and $76 per capita in low-income countries)
(9). About half of these investments are required in the form of
Figure 1.1 Share of women employed in the health and social sectors compared to share of women employed in
all sectors by ILO region, 2013
Source: International Labour Organization (1).
10.00%
20.00%
80.00%
0.00%
70.00%
90.00%
60.00%
40.00%
30.00%
50.00%
45.3%
Europe and
Central Asia
76.8%
43.1%
Americas
74.0%
42.2%
Africa
54.1%
39.5%
World
70.3%
37.4%
Asia and the
Pacific
63.5%
Arab States
15.6%
38.3%
Share of female employment in all sectors
Share of female employment in the health and soical sectors
A literature review
6

training, educating and employing health workers (9). Investing in the
health workforce maximizes women’s economic empowerment and
participation, extends universal health coverage, contributes to global
health security, and also has a powerful multiplier effect on economic
growth (10). Moreover, addressing gender biases and inequities in
the health workforce is essential not only for achieving SDG 5 (gender
equality) and SDG 3 (health and well-being), but also for achieving
other SDGs, such as SDG 4 (quality education) and SDG 8 (decent
work and inclusive economic growth) (Figure 1.2) (11).
As health systems around the world are facing a growing mismatch
between health worker supply and demand, the time is right for the
global health community to take collective action. Recent global health
and workforce strategies are recognizing the critical importance of
addressing the gender challenges of the health workforce as key
to achieving universal health coverage by 2030, and maximizing
women’s economic empowerment and participation. This evidence is
facilitating a new narrative on the health workforce, shifting the focus
from health as a cost and a drag on the economy to health as an
investment and multiplier for inclusive economic growth (3).
The three major global efforts seeking to address the health workforce
and gender are as follows.
• WHO Global Strategy on Human Resources for Health: Workforce
2030. The Global Strategy was developed to advance progress
towards attainment of the SDGs and universal health coverage by
ensuring equitable access to health workers. The Global Strategy
calls for the alignment of gender, employment, education and
health with national human resources development and health
system strengthening strategies (6). It argues that the projected
global deficit of health workers, coupled with rising demand to
create approximately 40 million new health care jobs by 2030,
uniquely positions the health and social sector to offer substantial
and tangible opportunities for decent work, gender equity and
greater women’s labour participation.
• United Nations High-Level Commission on Health Employment
and Economic Growth. The High-Level Commission, established
by the United Nations Secretary-General in 2016, made the
following recommendation, reaffirmed by the 61st session of the
Commission on the Status of Women (2017) and the Milan Group
of Seven (G7) meeting (2017) (3):
Maximize women’s economic participation and foster their
empowerment through institutionalizing their leadership, addressing
gender biases and inequities in education and the health labour
market, and tackling gender concerns in health reform processes.
Figure 1.2 Sustainable Development Goals
7

• Working for Health five-year action plan (2017–2021).
Through the Working for Health five-year action plan, WHO, the
International Labour Organization (ILO) and the Organisation for
Economic Co-operation and Development (OECD) have agreed
to support the implementation of the High-Level Commission’s
10 recommendations. The recommendations and action plan
identified (a) the development of gender-transformative global
policy guidance and (b) support to build implementation capacity
to overcome gender biases and inequalities in the education
Figure 1.3 Health workforce and gender: a theory of change
Source: Based on WHO (12).
and health labour market as two key deliverables to maximize
women’s economic participation and empowerment (12). Gender-
transformative policy requires a series of actions to be embedded
at every stage of policy action (Figure 1.3 and Figure 1.4) (12).
With multiple stakeholders prioritizing gender equity, it is of utmost
importance that the approach to implementation is systematic,
coordinated and evidence based. To facilitate this process, the WHO
Global Health Workforce Network established the Gender Equity Hub
(GEH).
Figure 1.4 Working for Health programme: a global movement for gender-transformative workforce development
Source: Based on WHO (12).
Concerted, tri-partite
social dialogue
Improved health
labour market data,
analysis and evidence
Enhanced national
health workforce
strategies
Sustainable domestic
and international
investments
Transformation and
scale up of education,
skills and decent job
creation towards a
sustainable health
workforce
workforce
1
Accelerate progress towards universal health coverage and the SDGs by
ensuring equitable access to health workers within strenchened health systems
(1) Expansion;
(2) TRansformation of the health and soical workforce
(1) Advocacy, social dialogue and policy dialogue
(2) Data, evidence and accountability
(3) Education, skills and jobs
(4) Financing and investments
(5) International labour mobility
2
3
4
5
Vision
Work
streams
Goals
Orgs
SDGs
A literature review
8

1.2 Gender Equity Hub (GEH)
The development of evidence-based gender-transformative global
guidance and its implementation requires a collective and concerted
effort. The WHO established the GEH at the fourth Global Forum on
Human Resources for Health held in November 2017. The GEH brings
together key stakeholders to support the implementation of the WHO
Global Strategy on Human Resources for Health and to achieve the
deliverables of the Working for Health five-year action plan. The
purpose of the GEH is to accelerate large-scale gender-transformative
progress to address gender inequities and biases in the health and
social care workforce in order to achieve the SDGs. The GEH works in
tandem with the other thematic hubs of the Global Health Workforce
Network, focused on topics identified as crucial for progressing the
WHO Global Strategy and the Working for Health programme.
The GEH is co-chaired by WHO and Women in Global Health.
Women in Global Health is a not-for-profit organization built on a
global movement that brings together all genders and backgrounds
to achieve gender equality in global health leadership. The GEH
includes members from a range of global health stakeholders,
including intergovernmental and multilateral agencies, civil society
organizations, academic and research institutions, think tanks,
foundations, the private sector, and individual experts. Its main
objectives are to advance knowledge, data and research on gender
and the health workforce; develop tools to promote gender-
transformative approaches; and accelerate progress on addressing
gender inequities and bias. The four key GEH priority areas were
identified through a consultative workshop held at the fourth
Global Forum on Human Resources for Health (Box 1.1). The major
activities of the GEH were defined by examining areas of comparative
advantage, identifying gaps in existing work, and addressing high-
priority needs. Additionally, key activities needed to drive evidence-
guided policy change were identified (Box 1.2).
Box 1.1 Global Health Workforce Network
Gender Equity Hub: priority areas
• Occupational segregation
• Decent work: workplace free from bias, discrimination and
all forms of harassment, including sexual harassment
• Gender pay gap
• Leadership and governance
Box 1.2 Global Health Workforce Network
Gender Equity Hub: five key activities
• Mapping: global evidence on good practice
• Data, evidence and accountability: evaluating current data
and evidence, and identifying gaps for future research and
development
• Policy tools: developing policy briefs and tools
• Dissemination: advocacy, social dialogue and policy
dialogue to disseminate evidence, policy tools, advocacy
kits, accountability scorecards and guidance to other
Global Health Workforce Network hubs
• Implementation: facilitating implementation of policy
through policy workshops, business solutions and private
sector engagement
1.3 Rationale for gender analysis on the
health workforce
Most of the evidence and research on gender in health has focused
on the demand dimension of health care, such as barriers to service
access experienced by women and the impact of health expenditure
discrimination on women (13). The evidence base is relatively thin
on the gender dimensions of the health care delivery side and the
workforce. In particular, evidence from low- and middle-income
countries is limited. There is also little evidence available on the
social workforce. Where available, research in this area rarely extends
beyond simple sex disaggregation into the more critical aspects of
gender power relations in health systems and their implications for
working practices, career patterns and occupational choices (13, 14).
A gender-based analysis of the health workforce is important for
health systems research. For research to instigate social and policy
change for better health, it should aim “to transform institutions,
structures, systems, and norms that are discriminatory” (15). In recent
years different forms and frameworks for researching gender relations
have emerged, including calls for adopting an intersectionality lens
that considers, in addition to gender, other identity factors that
contribute to discrimination. Other approaches, such as substantive
equality, emphasize the importance of considering the effects of past
discrimination, recognizing that rights, entitlements, opportunities and
9

access are not equally distributed throughout society, and there is
sometimes a need to treat people differently to achieve equal results.
For research to instigate social and policy change for better
health, it ought to aim “to transform institutions, structures,
systems, and norms that are discriminatory”.
A gender-based analysis of the health workforce is also urgently
needed to ensure that the expansion of health systems in the SDG era
capitalizes on the opportunity to transition to gender-transformative
health systems. Since this scale-up will focus on addressing the
projected global shortage of health and social care workers by
2030, and women are the majority of workers in these sectors,
gender analysis is critical to creating new jobs that will attract and
retain women workers. Investing in evidence on gender aspects of
human resources for health can inform global health policy-makers
and institutions and encourage them to apply a gender lens to the
health workforce. Effective gender-transformative health workforce
policies will address discrimination and rights abuses (such as sexual
harassment) that contravene good employment practice and law,
eliminate the gender pay gap, address occupational segregation and
increase gender-equal leadership. Gender analysis of the female
health and social care workforce will enable realization of a wider
gender dividend by bringing more women into paid, formal labour
market jobs with a positive multiplier for the health, education,
nutrition, income and empowerment of those women, their families
and communities.
With global health policy responsiveness to gender lagging behind,
more evidence on the gender dimensions of the health workforce
is needed to support the development of evidence-based, gender-
transformative health policies and actions across global health
systems and institutions.
A literature review
10

2.1 Objectives
The main objectives of this literature review are:
• to identify the available data and evidence from the literature
(published and grey) on addressing gender inequities in the health
workforce;
• to examine case studies, policies, tools, and strategies and their
impact on addressing health workforce gender inequities and
occupational segregation issues;
• to map programmes, initiatives, stakeholders, campaigns and
intersectoral opportunities across the public and private sectors of
relevance to addressing gender inequities and biases in the health
workforce;
• to synthesize lessons learned from the evidence, programmes,
initiatives and campaigns.
2.2 Methodology
Coupled with a global call for case studies, the GEH undertook a
comprehensive review of peer-reviewed articles, policy briefs and
programme interventions to evaluate gender and equity research within
the health workforce globally. Although the GEH prioritizes gender and
equity within the global health and social care workforce, the literature
on the social care workforce was not explored in this report, given the
limited material available. The process was as follows.
1. The GEH conducted a global call for best practices from December
2017 to January 2018. All articles, policy briefs, programmes and
other interventions received were analysed. The GEH received a
total of 25 submissions through this call, which included peer-
reviewed publications, programme interventions, and policy briefs.
All these submissions were included in the review.
Chapter 2. Objectives and methodology
2. Following the completion of the call for submissions, the GEH
members provided further publications and articles to guide the
literature review during February 2018 and March 2018. A total of
98 articles were received after removing duplicates.
3. A comprehensive and robust literature review was conducted
from December 2017 to July 2018 utilizing a keyword search of
the PubMed and Google Scholar electronic databases. Keywords
used to perform the search included the following: gender,
intersectionality, bias, discrimination, inequalities, harassment,
sexual harassment, violence, stereotyping, gender wage/pay gaps,
occupational segregation, gender parity, women’s leadership in
global health, health workforce, technology, corporate and finance.
AND/OR Boolean operators were used to search the databases.
A total of 100 additional articles were found after removing
duplicates from step 1 and step 2.
4. For the articles retrieved in steps 2 and 3, paper titles and
abstracts were examined using the following inclusion criteria:
» studies published in peer-reviewed journals
» published in the year 2000 and beyond
» English language publications
» articles for which the full text was available or accessible to us
» articles that provided evidence from three other sectors:
technology, corporate and finance.
Studies evaluating gender and equity dimensions in the workforce,
and articles pertaining to the health workforce, were prioritized.
The search ended upon saturation of the findings.
5. A total of 170 articles were included in the review after
performing steps 1 to 4.
6. We applied a structured evidence matrix and extraction tool
to extract findings from the 170 articles in eight months from
December 2017 to July 2018.
7. A draft report was made available for consultation from May 2018
to July 2018.
11

2.3 Limitations
There is a vast amount of literature, policies and programmes on
gender in the workforce. However, when the scope of the search
is narrowed to English language literature on gender in the health
workforce, the amount of material is much more limited. The members
of the Global Health Workforce Network GEH (see Annex 1) provided
extensive research articles and materials to ensure the review was
comprehensive. We received and reviewed very few programmes
and even fewer policies during this review, with the shortage being
particularly apparent for low- and middle-income countries. Literature
from the social care sector was not included in this review but will be
considered in subsequent reviews. Overall, there were some common
trends in the limitations of the overall body of literature on gender and
the health workforce, as described in the following paragraphs.
Intersectionality
The review was unable to apply a truly intersectional lens to gender
in the health workforce as the evidence predominantly focused on
gender, but did not provide further intersectional review, or provide
additional understanding of the impact of factors such as class, race,
ethnicity or religion on the health workforce.
Geographical focus
More reviews of the health workforce, particularly women in medicine,
have been undertaken in the United States of America, and to some
extent in Europe. However, there is limited evidence for gender in
the health workforce across other regions. Additionally, there is
no comprehensive global review of gender in the health workforce
available. It is important to note here that the review only took
into consideration evidence in English, which also imposed some
limitations on the geographical scope of the evidence.
Occupational focus
The literature demonstrated a focus on women in medicine,
particularly in the leadership and governance thematic area. There
was limited literature on the social workforce. Within medicine, there
was also a focus on specific specialties, in particular surgery. In recent
years, there has been more evidence emerging on nurses, midwives
and community health workers, though there is still limited information
about the experiences of women in other occupations throughout the
health workforce.
Sex- and gender-disaggregated data
Studies that evaluate discrimination as an aspect of gender are very
challenging. In many research studies, discrimination remains implicit.
The lack of data disaggregated by sex and gender within global health
further elevates the problem. This has resulted in limited attention to
gender discrimination within the health workforce.
Focus on women
The overwhelming majority of studies available look at gender and the
health workforce focusing on women. The experiences of men and
non-binary people were not found in any of the materials reviewed.
There is a need to shift the narrative and research focus away from
traditional or mainstream approaches that examine the deficits
in female characteristics or the perceived positive attributes of
male leadership, behaviour and job preferences towards a more
transformative approach that investigates the root cause of gender
inequalities embedded in systems of discrimination, bias, norms,
institutional systems and pay policies.
While the review was focused on the health sector to ensure that it
was manageable and useful, additional evidence was drawn from
other sectors included in the review methodology (such as technology,
finance and corporate).
Finally, while the evidence focused on barriers that affect women
in the health workforce, there is very limited information and few
case studies on the application of evidence-based recommendations
and policy actions to address these barriers. Many of the
recommendations or solutions put forward in the evidence were based
on barriers or drawn from the literature reviewed but were not tested.
Further implementation research is required to assess their viability
and effectiveness.
A literature review
12

3.1 Key messages
• Occupational segregation impacts service delivery and the health
system by limiting full participation of all genders in all aspects of
the health workforce, fostering greater gender inequities.
• Both horizontal and vertical occupational segregation by gender
are found globally in the health sector but vary depending on the
context and history of the country. Occupational segregation has
its roots in two cultural ideologies: gender essentialism and male
primacy.
• Occupational segregation by gender is driven by long-standing
gender norms that define caring as female work and portray men
as more suited to technical specialisms in medicine.
• Gender discrimination is a primary reason for women not entering
higher-earning medical specialties or taking leadership roles,
while gender stereotypes deter men from joining female-majority
professions such as nursing.
• The horizontal and vertical dimensions of occupational segregation
combine to cluster women into lower-paid and lower-status work,
with a lifelong impact on their earnings and economic security in
old age.
• Female-dominated professions, including caregiving and nursing,
tend to be given lower social value by gendered social norms, and
are therefore associated with lower pay and prestige.
3.2 Occupational segregation:
literature review
Occupational segregation is the first of the four workforce themes
prioritized by the GEH. The concept of “sex segregation” was first
introduced by Gross (1968) to elaborate the differences in the kinds
SECTION 2. KEY FINDINGS
Chapter 3. Occupational segregation
of jobs men and women undertake, on the basis of both supply-
side factors such as personal choice and demand-side factors
such as discrimination in the workplace (16). Prior to this the word
“segregation” was used primarily in reference to separation of races.
Segregation is a fundamental pathway to social inequalities that
not only separates different groups based on their demographic
characteristics such as gender, race or class, but also forms a basis
for discrimination and bias (17).
Occupational segregation impacts all genders and their experiences in
labour markets. Gender segregation manifests itself in various forms,
ranging from a narrower set of choices and job opportunities for specific
genders to stereotypes that result in gender pay gaps and reinforce
unequal power structures within a society (18). It is one of the most
enduring aspects of labour markets across the world and exists in
diverse political, economic, cultural and religious settings (17).
Women account for 70% of the health workforce, but they are
mostly concentrated in nursing and midwifery professions,
while far fewer are physicians
There are two types of occupational segregation: horizontal
segregation and vertical segregation (19). The levels of segregation
are determined by size of occupation, gender composition of the
workforce and distinctions in occupational settings (16). It is important
to assess segregation by examining both within occupational
categories and across categories. For example, women account for
70% of the health workforce but they are mostly concentrated in
nursing and midwifery professions, while far fewer are physicians (20).
According to UN Women, globally women are concentrated in service
jobs (61.5%) as compared to agriculture (25%) or industry (13.5%),
and women occupy fewer leadership roles as parliamentarians (23%)
or as chief executive officers (4%) compared to men (21). Figure 3.1
depicts women’s share of selected occupations in the United States in
13

2012 (22). While women are highly represented as dental assistants,
nurses, and even pharmacists, they make up less than half of the
physicians and surgeons in the United States (22).
Patterns of occupational segregation, especially women’s participation
in the formal labour market, vary significantly by region and country,
and are influenced by culture, income levels, local law and other
factors such as education or qualifications. Figure 3.2 highlights
how occupational segregation can vary significantly by country, as
evidenced by the share of female doctors in each OECD country (23).
The gender stereotype that assigns men the role of breadwinner while
women are prescribed the role of homemaker and child care is still
dominant and pervasive in many cultures. This stereotype remains
the leading cause of occupational segregation, as it either devalues
women’s contributions in the labour force or limits their participation
in the workforce. Moreover, a range of inequities emerge as a result
of gender segregation; for example, female-dominated jobs are
associated with lower salaries, fewer on-job trainings and limited
opportunities to exercise authority (16). The concept of occupational
segregation is applicable to all people, regardless of whether they
live in high-income countries or low-income countries (17). However,
the patterns of segregation may differ. For example, in high-income
countries women are concentrated in health, education, wholesale
and retail, while in low-income or lower middle-income countries
they are concentrated in the agriculture sector (21). Occupational
Figure 3.1 Women’s share of selected occupations (2012)
Source: Based on data from Hegewisch and Hartmann (22).
segregation in the health and education sectors is significantly more
disproportionate in high-income countries compared to upper middle-
income, lower middle-income, and low-income countries, as seen in
Figure 3.3 (24).
Occupational segregation has historically been attributed to factors
such as investments in human capital, social norms and stereotypes,
comparative advantages men have over women due to their physical
and biological characteristics, and the differences in income levels
between men and women (25). Women have had to struggle to
gain their basic rights to education and economic opportunities
(26). Women were also banned from entering different professions,
including medicine. For example, in the United Kingdom, women were
not allowed to enrol in medical schools until the late 19th century.
Realizing that the only pathway for women in the United Kingdom to
enter the medical profession was through nursing education, Elizabeth
Garrett gained her nursing qualification in 1865 and later became the
first woman to qualify as a doctor (27). The first woman to register as
a medical doctor in the United States was Dr Elizabeth Blackwell in
1858, and even then, she obtained a foreign degree to do so. In some
countries it took until the 1940s before a woman was able to qualify
as a doctor. Restrictions on women’s entry to specific professions and
types of work continue today but vary significantly across regions.
Men and women also spend very different amounts of time on unpaid
care work, with women spending between 2 and 10 times more time
20%
30%
90%
0%
80%
100%
70%
50%
40%
60%
Computer
Programmers
Bus
Drivers
Libraians
Registered
Nurses
Pre-
Kindergarten
Teachers
10%
Dental
Assistants
Cashiers LawyersPharmacists Photographers Mail
Carriers,
Post Office
CarpentersPhysicians
and
Surgeons
Civil
Engineers
A literature review
14

Figure 3.2 Share of female doctors by OECD country (2015)
Source: Based on data from ILO (24).
Source: based on data from OECD Health Statistics 2018.
Switzerland
Chile
Korea
Italy
Luxemburg
Japan
United States
Australia
Belgium
Iceland
50.0%30.0%20.0%0.0%
Turkey
10.0% 40.0% 60.0% 70.0% 80.0%
Hunary
Greece
Canada
Isreal
Ireland
New Zealand
France
German
United Kingdom
Norway
OECD34
Austria
Sweden
Denmark
Spain
Netherlands
Portugal
Czech Republic
Poland
Slovak Republic
Finland
Slovenia
Estonia
Latvia
Figure 3.3 Male and female employment (%) in health and education sectors (2015)
Male Employment
Female Employment
5%
35%
0%
30%
25%
15%
10%
20%
High IncomeUpper-Middle
Income
Lower-Middle
Income
Low Income
15

on unpaid care compared to men, depending on the country. This
unequal division of unpaid care work is associated with gendered
social norms of femininity and motherhood (28). Time use surveys
or data reveal that women spend more time on unpaid care and
household work compared to men (29). In general, women carry out
almost three more hours of unpaid work per day than men (29, 30)
(Figure 3.4). For example, women are expected to take care of
their families, home, children, or elderly relatives. In lower-income
countries, women are more likely to spend time on chores such as
collecting firewood and water; travel related to household activities;
or grocery shopping (29). Unpaid care work is directly correlated with
occupational downgrading, whereby women remain segregated into
part-time or vulnerable working conditions (31). Figure 3.5 displays
a breakdown of minutes per day spent on paid and unpaid work
between men and women in selected OECD countries (32).
Unpaid and informal work makes up nearly half of women’s
contributions to the global health sector. In 2015, the Commission on
Women and Health analysed data accounting for more than half of
the world’s population and found that women’s financial contribution
to the global health system amounted to nearly 5% of global GDP.
Of this contribution, nearly half was for unpaid work, as shown in
Figure 3.6. Dr Felicia Knaul, Director of the Harvard Global Equity
Initiative, announced that the “findings on women’s paid and unpaid
financial contributions to health worldwide only begin to explore and
quantify the work of women as health professionals in the paid health
care labour force, and their unpaid work to support health and prevent
illness undertaken in their own homes, in the homes of others, and
through volunteering in the health sector” (2).
While women’s contributions to the global health care sector makes
a substantial difference to countries’ economies, as well as individual
and societal well-being, the ratio of paid to unpaid work means that
Figure 3.4 Average work day and unpaid work, men
and women
Source: Based on data from World Economic Forum (30).
Unpaid work
7 HRS, 47 MIN
8 HRS, 39 MIN
1 Hour
30 Min
4 Hour
47 Min
Figure 3.5 Paid and unpaid work (minutes per day)
for men and women, by OECD country
Source: World Economic Forum 2017, based on data from OECD social
protection and well-being database.
Poland
Portugal
Austria
Italy
India
Japan
Ireland
Australia
Work (minutes per day)
Slovenia
China
Germany
Hungary
New Zealand
Spain
United Kingdom
Netherlands
Canada
South Africa
Estonia
Belgium
Denmark
United States
France
Finland
Korea, Rep.
Norway
Sweden
400200400800 600 200 600 800
0
Mexico
Turkey
Unpaid work, men
Paid work, men
Unpaid work, women
Paid work, women
A literature review
16

Figure 3.6 Financial value of women’s contribution to the global health system, as part of global GDP
Source: Langer et al. (2).
nearly half of this work remains unrecognized and unaccounted for in
decision-making. Unpaid or informal health care work, often critical
to a society’s health care system and well-being, routinely goes
unvalued. For instance, in Spain, 88% of all health work is unpaid
(33). The burden of unpaid work in health and social care, which falls
mainly upon women and girls, limits their access to both education
and paid work in and beyond the care sector, forming a “unpaid care
work-paid work- paid care work” circle as shown in Figure 3.7. (34)
Since women and girls from socially disadvantaged groups carry a
disproportionately large burden of unpaid care work; it affects both
the type and quality of jobs that are available to them and reinforces
their disadvantage. (34) These unfavourable conditions impact gender
equality both within the labour market as well as in unpaid care
contributions; resulting in gender segregation of jobs.
The segregation of people into occupations based on gender is
reinforced by two culturally determined narratives (35).
• Gender essentialism: the belief that men and women are different
and have different working styles and skills. This assumes, for
example, that women have a natural tendency for caring, nurturing
jobs while men are more inclined to be managerial or mechanical.
2.47%
2.35%
Global GDP
Unpaid
Paid
• Male primacy: the belief that men and boys are naturally more
dominant and more status worthy compared to women and
girls. Gendered barriers restrict women and girls from entering
male-dominated occupations such as surgical care, while there
are barriers that restrict men from entering female-dominated
occupations such as education or social care (35).
Despite making progress towards gender equality, equal engagement
of all genders in certain occupations and levels of decision-making
is limited. In their book Occupational ghettos, Charles and Grusky
argue that while egalitarian forces have reduced vertical segregation
in “non-manual” jobs (managerial, sales or service jobs), horizontal
segregation persists due to gender essentialism as women remain
concentrated in non-manual jobs in the post-industrial era while men
dominate the skilled trades (36). Women are entering male-dominated
jobs at a faster rate than men are entering female-dominated
occupations. Less than 10% of all registered nurses in the United
States are male, though that proportion has been steadily increasing
over the past 50 years, as seen in Figure 3.8 (37). While women face
gender-based discrimination and the “glass ceiling” limiting their
advancement in male-majority jobs, men who enter female-majority
professions have advantages that may speed their promotion, referred
to as the “glass escalator” (38).
17

The ILO 2018 report on world employment highlights that women
in low- and middle-income countries are in more vulnerable forms
of employment compared to men, and there are fewer employment
opportunities for young people (below the age of 25 years) (39). In
Arab States and northern Africa, women are twice as likely to be
unemployed as men (39). One reason for this is labour laws that
restrict women from entering certain fields. Women face more
institutionalized restrictions in the workplace in some regions
compared to others, such as South Asia, Middle East and North
Africa, as seen in Figure 3.9 (40). These differences hinder progress
on gender equality. A report commissioned by the European Union
determined that an acceptable level of gender gap for “gender-
neutral” occupations would be a mix of men and women between
40% and 60% (41). The United Nations has put this benchmark
between 45% and 55% (42).
Trends in the labour market have changed significantly, with most
countries projecting growth in women’s participation in the labour
force. But it is a concern that globally, women’s labour force
participation has declined on average by 2% between 1990 and 2017
(43). Only high-income countries have shown an upward trend during
this period, while low-income countries have fluctuated between
downward and upward trajectories. While there are many variations
Figure 3.7 The cycle of unpaid care work–paid work–paid care work
Source: ILO (34).
between countries, the trend for the middle-income, low- and middle-
income, and lower middle-income categories of countries is for a
decline in women’s formal labour market participation (43). There
are many possible explanations, one being that as families increase
their income there is pressure for women to revert to the traditional
stereotype of a homemaker, or that in economic recessions women
are often the first group pushed out of the formal labour market into
the informal sector.
Globally, women’s labour force participation has declined on
average by 2% between 1990 and 2017.
3.3 Occupational segregation by
gender in the global health workforce
Women in the global health workforce have an inverted career
pyramid (44). Gender differences in participation in the global health
workforce are driven by men’s greater access to education, training
and the formal labour market; historical discrimination against
women’s access to higher-status and higher-paid specialties, which
manifests in a lack of female role models, gender stereotyping and,
PAID CARE
WORK
PAID WORK
Levels and distribution of unpaid
care work impact the conditions
in which unpaid carers enter and
remain in paid work, and influence
working conditions of care
workers.
Gender equality in the labour market,
including in women’s participation,
employment and working conditions
also imply positive outcomes for care
recipients.
Care workers in adequate numbers and
working conditions contribute directly to
gender equality in the world of work and the
redistribute unpaid care work.
UNPAID CARE
WORK
A literature review
18
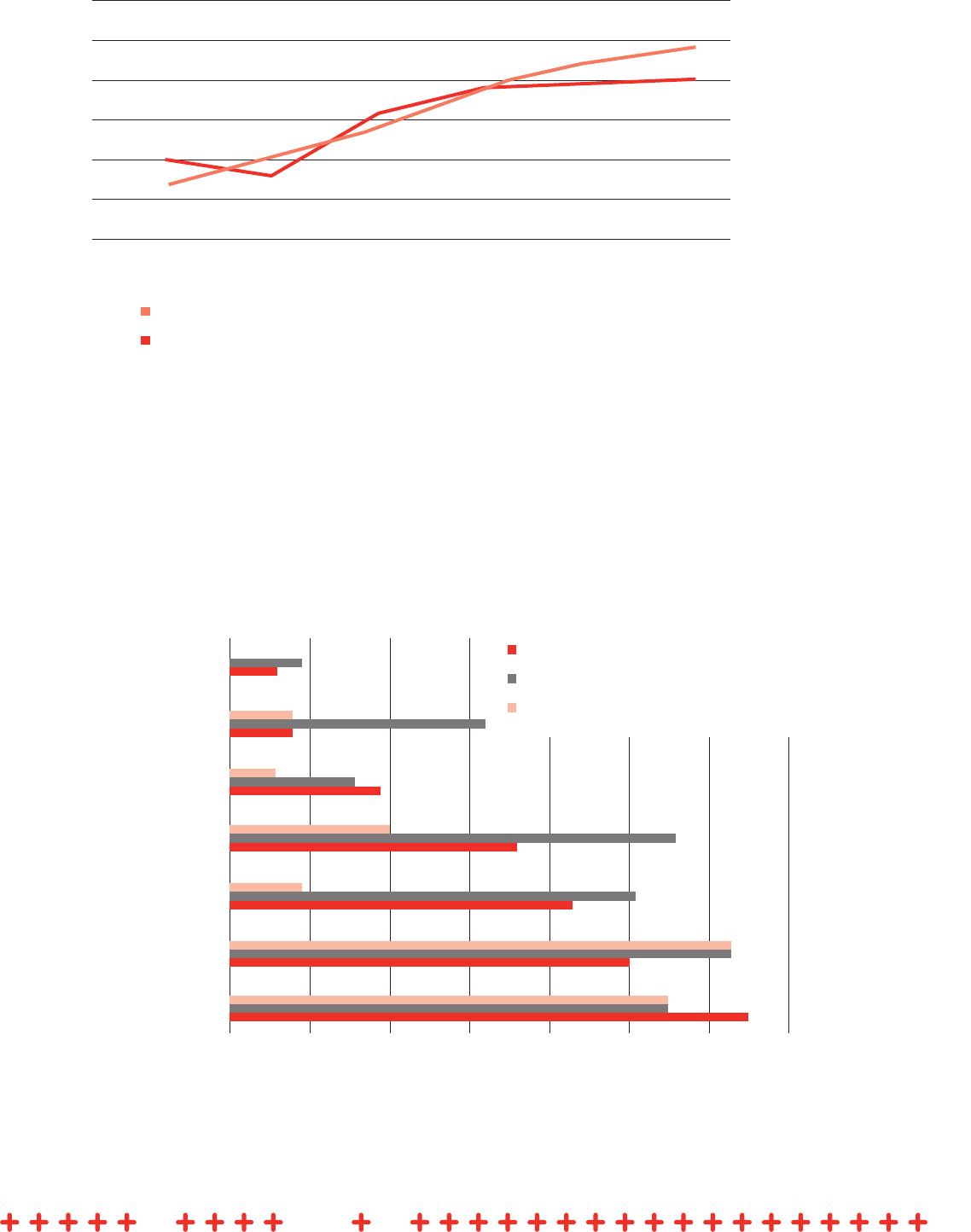
Figure 3.8 United States share of nurses who are male (1970–2011)
Source: United States Census Bureau (37).
Figure 3.9 Percentage of economies that restrict women’s employment, by type of restriction
Share of registered nurses who are male
Share of licensed practical and vocational nurses who are male
2.0%
12.0%
0.0%
10.0%
6.0%
4.0%
8.0%
2011
1990
1980
1970
20062000
Source: World Bank (40).
50%30%20%0% 10% 40% 60% 70%
East Asia & Pacific
Latin America & Caribbean
Europe & Central Asia
Sub-Saharan Africa
South Asia
Middle East & North Africa
OECD High-income
Jobs deemed hazardous, arduous or morally inappropriate
Industry-specific restrictions (eg. in mining or construction)
Restrictions on working during night hours
19

in some countries, formal restrictions on women’s work during night
hours; women’s greater burden of unpaid reproductive work, which
may deter them from entering some specialties; cultural stereotypes
that deter men from aspiring to join majority female professions such
as nursing; and gender discrimination against women in entry to
higher-status specialties and leadership roles.
Globally, women are highly concentrated in primary care, nursing
and midwifery, with significant variation between countries. This is
an example of horizontal segregation, such as Denmark, women
make up 90% of the nursing and midwifery professionals (20). In
addition, women account for one third of all physicians within the
United States, while in Scandinavian countries women make up
45–56% of doctors, and in the Russian Federation 70% of physicians
are women (45). Despite a large proportion of female physicians in
Russia, studies noted that far few were found to be in prestigious
specialties, tertiary care and academic medicine. (45) The percentage
of women in dentistry globally is projected to increase to 28% by
2030 (46). Horizontal segregation leads to the feminization of certain
medical specialties (47); women are more likely to choose the fields of
paediatrics, paediatric surgery, obstetrics, gynaecology, oncology and
dermatology (48–52).
Globally, women are highly concentrated in primary care,
nursing and midwifery, with significant variation between
countries
Moreover, gender inequality within the medical workforce remains
highly contested, particularly for surgical specialties, as only one
third of women doctors select surgery compared to men (53). One
reason for this is the perception that surgical specialisms are a male
domain where toxic masculinity is common, creating a hostile work
environment for women. The #MeToo movement in the United States
has encouraged women in medicine to come forward and share their
experiences of harassment in hospitals and operating rooms (54).
The higher numbers of men pursuing internal medicine and hospital
specialisms, plus the higher numbers of women pursuing family
practice, obstetrics and gynaecology, has resulted in the gender-
based segregation of men and women in medicine in the United
States (55). Women are increasingly entering obstetrics, while their
numbers in breast surgery and urology remain low.
While there is plethora of literature investigating why men and women
studying medicine pursue different specialties, most of these studies
have been conducted in the United States or the United Kingdom.
This limits our understanding of the factors explaining why more and
more women are being excluded from different health care specialties
(53, 56). With large gender gaps in wages and leadership positions in
health care, it is critical to understand the drivers of these patterns of
occupational segregation (57–59).
Horizontal segregation also impacts women in health across all
occupations. In the United States, women in nursing and medicine
work the same number of hours as men but earn 78% of their male
counterpart’s earnings (60). Women health workers tend to work
fewer hours than men in countries where data are available, except
in the Russian Federation, where they were found to work longer
hours (60). In Canada, when primary care providers were compared
by gender, women self-reported fewer hours of work than men, saw
less patients and delivered fewer services. However, using hours as an
indication of work impact did not reflect the realities that women were
more likely to spend longer with their patients, and to address more
problems during each visit (61).
In the United States, women in nursing and medicine work
the same number of hours as men but earn 78% of their male
counterpart’s earnings.
3.4 Factors that lead to occupational
segregation
There is no single factor that can unilaterally explain gender
segregation in education and the labour market (62). Boxes 3.1, 3.2
and 3.3 highlight some of the individual, organizational and societal
factors contributing to gender segregation.
3.5 Why occupational segregation
matters
Global health policy-makers and decision-makers need to understand
the factors that lead to the clustering of men and women in certain
jobs. Studies have shown that organizations that adopt policies to
attract, develop, compensate and retain the best talent will be the
ultimate winners (81). However, an analysis of the gender-related
A literature review
20

Box 3.1 Individual factors contributing to gender
segregation
EARLY DEVELOPMENT AND FAMILY RELATIONS
Early development impacts the career choices people make.
Examples
• Gender-biased toys given to children influence their
interests and career choices (63).
• Demographics and personal values are associated with
gender differences in specialty choice (55, 64).
WORK–LIFE BALANCE
Control of lifestyle and work–life balance influence specialty
preference for women (49, 65, 66) and men (67).
Women’s greater burden in terms of household work,
responsibility for family, child care and protected time for
breastfeeding is considered one of the drivers for occupational
segregation (55, 68).
Examples
• Often workplaces do not have private space for feeding
mothers (69).
• In comparison, due to decreased societal expectations
of child care, men with children see less impact on their
careers compared to women. Women on the other hand
often have to struggle to balance expectations (70).
CHOICE AND INTERESTS
Gender norms also influence occupation choice and interest
as students – women are encouraged to pursue a career
choice based on idealism, where men are more likely to be
influenced by the prospect of a good income or prestige (48).
Example
• The #MeToo movement has enabled many American
women in medicine to come forward and admit that
they chose a female-dominated specialty over a male-
dominated specialty just to avoid exposure to toxic working
environments.
Box 3.2 Organizational factors contributing to
gender segregation
WORKING HOURS
Work scheduling challenges – such as long training hours
and inflexible rotation schedules – conflict with the societal
expectation that women are the primary caregivers in their
families.
Examples
• It has been shown that the more inflexible or time
consuming a specialty is, the more likely it is to be male
dominated, as in the case of surgery (2, 71, 72).
WORKING CONDITIONS (AUTONOMY, WAGES, JOB
SECURITY, HEALTH AND SAFETY)
Working conditions can lead to gender segregation.
Examples
• Women in male-dominated sectors tend to experience
gender discrimination, differences in task allocation, fewer
opportunities for promotion and lower salaries at higher
frequencies (73).
• Fear of workplace discrimination or selection bias leads
women to take lower-paying jobs.
ROLE MODELS
The paucity of female role models and lack of successful
women in surgical specialty is the most often cited reason for
reduced interest in surgery among female medical students.
Example
• One study found that only 35% of female medical students
could identify a mentor during surgical clerkship; while in
another study found that among female surgical students
who had mentors, 90% had a male mentor as compared
to female mentor. (74, 75).
INSTITUTIONAL POLICIES
Social policies such as parental leave, maternity leave, and
subsidized child care also influence the career choices of men
and women (76) and ways in which they organize personal
lives (68).
21
Box 3.3 Societal factors contributing to gender
segregation
GENDER STEREOTYPES
There are gender stereotypes that define characteristics of
female-dominated jobs.
Examples
• There are expectations that women may be willing to take
on more tasks, are less inclined to complain, and are more
patient with monotonous work. Women’s lower participation
in labour unions keeps women in low-paying, flexible roles
and in jobs that involve less decision-making (77).
• Overall, gender stereotypes drive institutional policies, for
example with regard to parental leave, care leave, and
availability of child care facilities. The lack of gender-
responsive policies, combined with societal expectations,
means lower retention and recruitment of women (41).
• The fact that certain medical specialties conform with
traits seen as traditionally masculine also deters women
from joining, for example the existence of the so-called
“male surgeons’ club” (78).
• When men enter occupations that are traditionally more
feminine they can experience setbacks in prestige and
pay. Men with children are more likely to avoid these
occupations (79).
DISCRIMINATION
Sex and gender are important considerations for hiring and
promotion (77).
Examples
• Women may be discouraged from taking surgery as a
specialty due to discriminatory attitudes during training
rotations in general surgery (52, 78).
• Women discriminating against women may perpetuate the
cycle of gender disparity, especially within surgical care (80).
Occupational segregation is an important workforce priority because
it can lead to loss of talent and diverse voices from the workforce.
Gender segregation is one of the major reasons behind shortages
and surpluses of workers across occupations, as women tend to
be concentrated in roles seen as caring and nurturing, while men
are in technical or managerial jobs. Gender segregation is also an
established source of gender inequality, as it reinforces some of
the gender stereotypes associated with men’s and women’s gender
roles, working styles and competencies. It is also linked to economic
empowerment and poverty. Women often have less coverage for social
protection, such as pensions, due to their absence from the labour
force. They are also prone to higher levels of employment in unpaid or
part-time jobs and have less access to quality employment (39). Men
are more concentrated into higher-paying jobs in the private sector
and in sectors that are less willing to provide protected leave for care
needs, such as child care or elder care. Social stigma is attached to
men entering more female-dominated jobs. These stereotypes limit
women’s participation in labour markets and, on the other hand, put
significant pressure on men to not take leave, such as parental leave,
when it is available to them (18). Gender segregation also results in
lower salaries and worse working conditions in occupations dominated
by women (17).
Gender segregation also affects the educational choices of men
and women and the type of specialties they choose during medical
training. Gender segregation in the health workforce has implications
for the development of strong and resilient health systems that are
capable of tackling health needs worldwide (83). The number of
women enrolled in medical schools has increased over the years.
Recent data from the Association of American Medical Colleges in
the United States show that in 2017 women outnumbered men in
medical colleges for the first time in history (84). Since 2015, female
enrolment has increased by 4% while male enrolment has decreased
by 6.7%, which indicates that the future of medicine and global health
is female (84). However, an increase in enrolment at medical schools
does not necessarily ensure a supply of health care professionals
to meet population needs. For example, women continue to be
underrepresented in the fields of surgery and surgical subspecialties,
a trend that is found not only in the United States, but also in Canada,
the Netherlands and the United Kingdom (53, 80).
Gender segregation in the health workforce has implications for
the development of strong and resilient health systems that are
capable of tackling health needs worldwide.
policies of 140 global health organizations found that only 43%
had specific policies in place to promote gender equality in their
workplaces, including strategies to support women’s career paths.
In fact, 30% of these organizations did not even mention workplace
gender equality in their policies (Figure 3.10) (82). The time is right for
global health systems and organizations to reflect on their strategies
and design systems and structures that create conducive working
environments where all members of the workforce can thrive and
achieve their full potential.
A literature review
22

Organizational structures or systems need to create enabling
environments for all genders. As more women are getting trained
and educated, we need to create job opportunities where all workers
regardless of their gender can thrive. Similarly, we need to change
mindsets around men entering female-majority jobs such as nursing.
There is a need to remove labels such as “male dominated” and
“female dominated” from the health and social care workforce
vocabulary if we are to adopt gender-transformative approaches
within the health and social care sector and achieve gender equality in
this sector. Failure to address the shortage of health workers will have
a crippling effect on poverty alleviation, development, and economic
growth, as well as stalling progress on the SDGs and universal health
coverage.
Figure 3.10 Do organizations have workplace gender
policies?
Source: Global Health 50/50 (82).
have specific
measures in
place
commit to gender
equality but lack
specific measures
simply comply
with laws
15%
make no
reference
to any
measures or
commitments
30%
12%
43%
23

4.1 Key messages
• A large percentage of women in the global health workforce face
discrimination, bias and sexual harassment.
• Women are more likely to face sexual harassment in the workplace
than men. For example, in the United States 30% of female
medical academics reported accounts of sexual harassment
compared to 4% of men.
• Many countries, particularly low- and middle-income countries,
do not have a legislative framework to support gender equality at
work, including laws to prohibit sexual discrimination and sexual
harassment at work.
• While the #MeToo movement has encouraged more open
discussion of sexual harassment in some countries, it remains a
serious and widespread abuse causing attrition, loss of morale,
stress and ill-health for survivors.
• Female health workers in conflicts or emergencies or working
in remote areas can face violence in the course of their work,
with a number of female health workers severely injured or killed
every year.
“To reduce the gender gap and add up to US$ 6 trillion to the
global economy by 2025, nations must eliminate gender biases
and inequities for women at work, including in the health
labour market.” James Campbell, Director, WHO Health Workforce
Department, December 2017
4.2 Decent work: introduction
Decent work is the second of the four workforce themes prioritized
by the GEH. SDG 8 – Decent work and economic growth – sets the
agenda for full and productive employment and decent work, and for
Chapter 4. Decent work without
discrimination, bias and sexual harassment
promotion of sustained, inclusive and sustainable economic growth
for all as key to alleviating poverty, protecting the environment, and
ensuring people’s well-being (11). Decent work involves creating
conducive work environments built on the principle of equal
opportunities for all, free of discrimination, bias or harassment,
including sexual harassment. This is an important goal that is a
cross-cutting theme across other forms of inequalities, including
occupational segregation and the gender pay gap. In the context
of this paper, decent work includes work free from discrimination,
bias and sexual harassment, and with equal pay within the health
care workforce. The gender pay gap is discussed in Chapter 5.
Addressing discrimination and bias within the global health workforce
is an important step towards achieving gender equality and building
stronger and resilient health systems that uphold the basic principles
of human rights (5).
“By 2030, achieve full and productive employment and decent
work for all women and men, including for young people and
persons with disabilities, and equal pay for work of equal
value.” SDG 8, Decent work and economic growth, Target 8.5
With 40 million new health jobs to be created by 2030, the
overarching objective is now to create jobs differently, according to the
principles of decent work, and to meet the targets in SDG 8, especially
Target 8.5. Currently, the majority of women in the global health
workforce work under conditions that do not meet the standards
for decent work, not least because of the near universal gender pay
gap. So, the objective must also be to ensure that both new jobs and
existing jobs in the global health workforce are upgraded to meet
decent work standards, not only because it is the right thing to do but
also to create a stronger foundation for better health for all.
While modern workplaces are far less dangerous and demanding than
they were historically, they are manifesting discrimination and bias in
subtle ways (85). There is a large body of research that shows women
face discrimination in almost every field of science and engineering
(86). The discrimination also varies based on career stage and field
A literature review
24

(86). As a result, men and women have different work experiences
even if they work in the same organization. For example, the
expectation to work long hours, to be constantly available, to adapt
to rigid career tracks and to have inflexible work schedules creates
stress, reduces morale, and conflicts with the work–life balance
of employees. Women are more likely to face these challenges to
work–life balance than men. The difficulty of keeping up with these
growing expectations pushes women to take up part-time jobs, or
remain segregated into female-majority jobs, or take leave from work
(85) to fulfil their caring roles at homes. Women have been observed
to move towards professions that offer greater flexibility. They often
have to trade off flexibility and earnings (87). Men and women may
start off with the same salaries or lower gender pay gaps, but the gap
increases over the course of their career due to career interruptions
and differences in job experience or number of hours worked (87).
The penalty for taking leave or time out is huge and accounts for
about 67% of the total penalty from career interruptions (87). Highly
trained women pay a higher price for returning to work after leave
(88, 89), and working mothers are perceived to be less committed
to work due to their family obligations and hence considered less
desirable for hiring or promotion (90). When it comes to hiring or
promotion decisions, gender bias against female candidates favours
male candidates (91).
Some women at the workplace face an additional dilemma of “double
jeopardy” – a double burden of discrimination, not only on account of
their gender, but also because of their race or caste (92). Most of the
expectations at work result from the gender norms and stereotypes
to which men and women are assigned. As a result, men gain
opportunities while women more often lose both in career progression
and earnings.
4.3 Decent work in the global health
workforce
The gender and power relationships that exist within and outside
the health system create differences in exposure and vulnerabilities
among men and women that lead to reproduction of inequalities
within the health system (84). Power relations, based on hierarchical
health systems that “rank” the value of each profession and each
person, create a workplace environment that fosters a lack of decent
work conditions.
Workplace violence and discrimination is also linked to the social norms
that create gender hierarchies and imbalances, starting from home and
progressing to society at large. Women face a disproportionate burden
of violence and discrimination across all sectors (80, 93).
4.4 Discrimination
There are many forms of gender discrimination, including direct
discrimination (for example, excluding women from decision-making
and training opportunities); indirect discrimination (for example,
exclusion of informal or home-based health workers from protective
labour laws); sexual harassment; gender stereotyping that limits
women to inferior roles and informal care roles (as in the case of
community health workers); vertical and horizontal occupational
segregation; wage discrimination; and benefits and working conditions
discrimination (5, 94). Gender discrimination and inequality are key
barriers to entry, re entry and retention of female health workers (5).
Caregiver discrimination is prevalent in many forms, for example, by
fee demotion for pregnant students, who are often left behind in their
curriculum or practicum; or by prohibiting pregnant students from
continuing education (95).
Literature suggests that gender discrimination and gender inequality
within organizations are linked to low morale, low self-esteem, and
lower productivity for the workers, and affects mental and physical
health (5, 96–98). This gives rise to health system inefficiencies
that obstruct the pipeline of qualified and skilled health workers,
create recruitment challenges, and lead to absenteeism, attrition and
maldistribution of the health workforce (5).
Gender discrimination and gender inequality within
organizations are linked to low morale, low self-esteem, and
lower productivity for the workers, and affects mental and
physical health.
Female-majority jobs often face a greater burden of discrimination.
For example, the WHO report on midwives’ voices (99) highlights how
power structures and gender dynamics should be restructured to
address the needs of midwives. Midwives provide high-quality care
to women, newborns and their families, but many are frustrated with
their lack of voice and power to bring change. Of the nurses in the
study, 36% reported not being respected by their seniors, 32% said
they would like to be heard or listened to, and about 37% of midwives
faced harassment at work (99).
Women’s childbearing and family obligations also prevent them from
undertaking health trainings or scholarships or enrolling in schools
(95), often because training is not set up to accommodate the needs
of workers with care responsibilities.
25
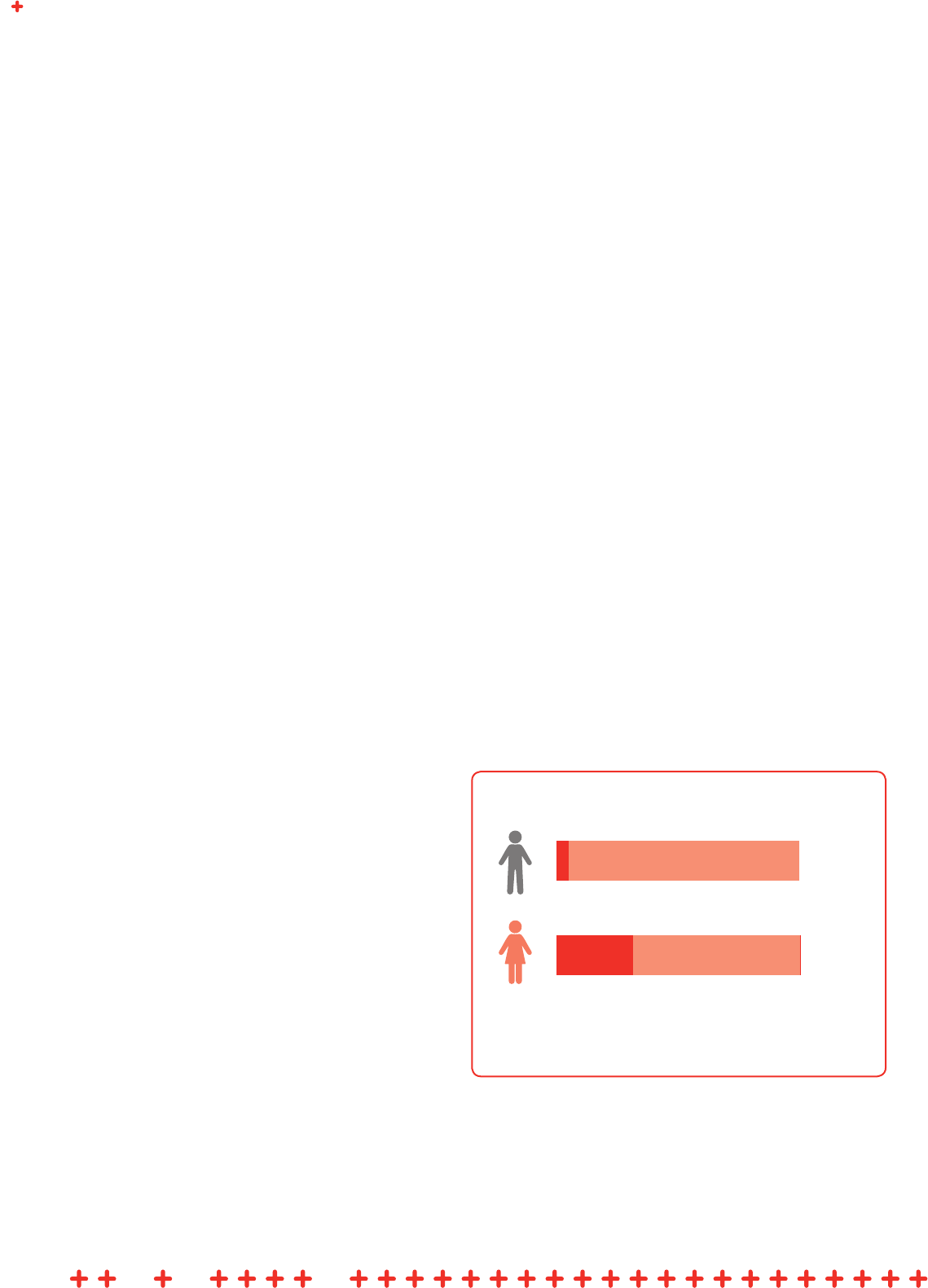
4.5 Bias
Women are more likely to face bias at work. It is important to note
that gender is only one intersection, and that many women experience
additional bias due to their race, ethnicity, culture, regional, caste
or class. These types of bias lead to a double burden or “double
jeopardy” faced by women with additional marginalized identities (92).
Men can also face bias in female-majority jobs, which may result in
lower status.
Gender bias in global health academia is well established. One
study found that both men and women have a subtle bias towards
women when it comes to hiring and promotion. Another study
found that letters of recommendations are written differently for
men (“his research”) and women (“her teaching”) (100). These
biases exacerbate gender gaps in academic medicine. For example,
women represent only 20% of deans in the top 25 global schools of
medicine and 36% in the top 25 global schools of public health (101).
Academic publishing is also a gendered system, with fewer women
represented on editorial boards and as peer reviewers (102). Women
are likely to publish less during the first decade of their scientific
careers compared to men (103). This is evident from data revealing
that men authored about 70% of the total publications on Web of
Science between 2008 and 2012 (104).
4.6 Sexual harassment
Sexual harassment refers to unwelcome sexual advances or requests
for sexual favours, whether verbal, physical or visual. There are
many forms of sexual harassment: it may include hiring, firing and
promotion decisions subject to provision of sexual favours, unwanted
sexual advances, touching, sexual violence, and inappropriate
comments or obscene remarks, which generally create a work
environment for women that is hostile, intimidating and demeaning.
Men also face sexual harassment at work but women suffer the
majority by far. For example, in the United States, 30% of female
medical academics reported sexual harassment compared to 4%
of men (Figure 4.1) (105). Of those who reported harassment, 47%
stated that these experiences negatively impacted their career
development (105). Female health and social care workers face
harassment and violence from three sources – male colleagues, male
patients and the wider community, including visitors to facilities or
men in the community if they are outreach workers. The stigma in
reporting cases in the health professions has created a misperception
that sexual harassment cases are rare. But health systems are no
exception. Nurses and community health workers have commonly
been subject to sexual harassment despite the work environment
being predominantly women (106).
Sexual harassment against female health workers appears to be
a universal phenomenon. Migrant female health workers can be
particularly vulnerable to violence and harassment, as can female
health and social care workers in domestic settings. A review in
Rwanda found that approximately 39% of health workers had faced at
least one form of workplace violence, such as verbal abuse, bullying
and sexual harassment, in the 12-month period prior to the study,
with women disproportionately affected (83). In Nepal, 42% of health
workers reported experiencing sexual harassment in the form of
verbal and physical abuse, and almost two thirds of the health workers
reported being harassed by their senior male colleagues (96). Lady
health workers in Pakistan reported experiencing sexual harassment
from both senior and junior staff, including management (107, 108).
In the Republic of Korea, 19.7% of women in nursing reported
experiencing sexual harassment, noting that the operating theatre was
the most frequent place for this to occur (109). Women are likely to
experience sexual harassment, even if they are higher in the traditional
medical hierarchy. In a survey of physicians in the United States, 30%
of those surveyed reported having faced a personal incident of sexual
violence in the workplace (106). Threats of violence or harassment do
not only come from sources internal to the health system; for example,
Figure 4.1 Percentage of United States medical
academics reporting sexual harassment
Source: Based on Jagsi et al. (105).
1,066 recipients of NIH academic
career development awards
4%
30%
A literature review
26

community health workers in Kenya experienced threats of violence
by husbands when providing HIV testing to wives. Cases of rape were
also reported, leading to calls for security services to accompany
community health workers (108).
Women are likely to experience sexual harassment, even if they
are higher in the traditional medical hierarchy.
Sexual harassment in the workplace is difficult to combat on a global
scale, given the vast differences in laws and policies addressing or
penalizing sexual assault around the world. Figure 4.2 depicts the
number of countries that have no laws, civil remedies, or criminal
penalties for workplace sexual harassment (110).
Harassment is prevalent in academic medicine as well. A meta-analysis
of studies on harassment and discrimination in medical training showed
that around 60% of students and trainees experienced discrimination
and sexual harassment during their training period (111, 112). A recent
report from the National Academies of Sciences, Engineering, and
Medicine raised concerns about the prevalence of sexual harassment
in academic sciences, engineering and medicine, which threatens the
integrity of education and research in these fields (113). The survey
findings from this survey found as high as 50% of female medical
students experiencing sexual harassment from faculty or staff at one of
the universities in United States .
Conflict-affected countries or remote settings present unique risks to
women in health care, where they are highly vulnerable to violence
(114). In Cambodia, women in conflict-affected areas face reported
risks to their personal safety, and loss of family contact (115). In
Pakistan, female polio outreach workers have been murdered and
attacked, not only causing tragic loss of life (116) but also stalling
elimination of polio from the country. A young midwife in Nigeria was
abducted and killed in October 2018 (117). Failure to protect front line
female health workers in conflicts and emergencies inevitably restricts
services to highly vulnerable women desperately in need of all health
services but particularly during pregnancy and childbirth.
In Pakistan, female polio outreach workers have been murdered
and attacked, causing not only tragic loss of life but also
stalling elimination of polio from the country.
Sexual harassment is so prevalent it cannot be treated as an
individual occurrence or aberration and needs organizational
strategies, based on law, to address culture, prevention, accountability
and support to survivors. Very few organizations keep systematic data
on cases and outcomes, making it difficult to analyse the extent of
sexual harassment and its impact on female health workers, and to
build policy measures to eliminate it. While the #MeToo movement has
built momentum towards raising the profile of sexual harassment and
assault, it remains a source of stigma and taboo. The onus of proving
guilt too often falls on the shoulders of the survivor. Since power
remains the underlying motive behind acts of sexual harassment and
violence at work (118), survivors are often silenced or risk facing
retaliation. Where there are no proper guidelines or policies to address
incidents of sexual harassment, cases may be dealt with on an ad
hoc basis, often favouring the perpetrator, who is likely to be more
powerful in the system (119).
Due to imbalances of power, fear of not being believed, and the
prospect of retaliation, survivors of harassment have often remained
silent. But with the #MeToo movement, the focus has rightly shifted to
addressing all forms of harassment in the workplace, including sexual
harassment (120). Issues that were once considered taboo can now
be more openly discussed in workplaces in some countries (121).
While this gives a unique opportunity to global health policy-makers
to agree and commit to institutionalizing policies and culture change
to eradicate all forms of harassment and discrimination, there are still
many contexts where discussions of sexual harassment are culturally
inappropriate, and where women are either silenced or face the threat
of losing their jobs if they report harassment (Box 4.1).
Figure 4.2 Inadequacy of global sexual harassment laws
Source: Council on Foreign Relations (110).
59 countries do not have laws
prohibiting sexual harassment in
the workplace
100 countries do not have civil
remedies for sexual harassment in
the workplace
110 countries do not have
criminal penalties for sexual
harassment in the workplace
27

4.7 Why addressing decent work in the
global health workforce matters
Bias and discrimination rob women of opportunities but also rob health
systems of female talent. This becomes everybody’s problem because
it impacts the quality of health systems used by all genders. Creating
safe and enabling work environments where all genders can work to
their full potential has huge implications for the economic productivity
Box 4.1 Origin of the #MeToo movement
The #MeToo movement first originated in 2007, when Tarana
Burke, an African American woman, launched a campaign
to reach out to sexual assault survivors in underprivileged
communities (122).
This campaign turned viral when actress Alyssa Milano
converted it into a hashtag and called on followers to share
their stories of sexual harassment and assault on Twitter using
the phrase “Me Too” (122).
and well-being of populations. It would improve health workforce
recruitment and productivity, as well as retention. It would also have
positive effects on quality of care, which would improve patient
outcomes and health system efficiencies. It is the fundamental right of
health workers to have freedom to express their opinions and be able
to participate and engage in improving the conditions of the health
workforce. Ensuring workplaces where all female health workers are
assured of safety, dignity and respect is essential to addressing global
health worker shortages, meeting health care demands, and unlocking
wider social and economic potential.
Creating safe and enabling work environments where all
genders can work to their full potential has huge implications
for the economic productivity and well-being of populations.
Sexual harassment in the workplace has a variety of negative impacts
on female health workers, including on their physical and mental
health. Studies have shown sexual harassment experienced during
medical training can influence decisions on specialty and residency
programme selection (95). Furthermore, this effect extends beyond
the individual experiencing harassment to the health system as a
whole. Examples of systemic consequences include impediment of
health workers’ advancement, increased stress and decreased morale
and productivity, and a limited pool of health workers to deal with
today’s health challenges (5, 123). In a world needing to create an
additional 40 million health and social care sector jobs there is an
immediate need to record, prevent and address the causes of sexual
harassment, not only because it is a human rights violation but also
because it results in attrition, loss of female talent, and reduced
morale and productivity. The perception that certain types of work or
sectors are likely to make women vulnerable to the risk of violence
and sexual harassment will affect recruitment and health worker
supply. Current levels of sexual harassment are diminishing patient
outcomes and creating major inefficiencies in health systems.
A literature review
28

5.1 Key messages
• Most of the gender pay gap remains unexplained by factors
such as age, experience, education, number of hours worked, or
specialty choice. This suggests discrimination and bias against
women and in favour of men.
• The unadjusted pay gaps in health and social care, estimated at
26% in high-income countries and 29% in upper middle-income
countries, are higher than other economic sectors.
• Occupational segregation by gender, with women tending to be
clustered into lower-status and low-paid sectors and specialisms
in health, is associated with a gender pay gap in favour of men.
• Equal pay for equal work legislation and strong collective
bargaining, absent in many countries, are essential for addressing
the gender pay gap in the health sector.
• The gender pay gap results in lower lifetime income for women,
reduced access to pay-related social and health benefits (where
they exist), and increased poverty for women in older age.
Chapter 5. Gender pay gap
• Women’s economic inclusion, and therefore closing the gender
pay gap, is critical to achieving the SDG overarching objective of
leaving no one behind.
5.2 Gender pay gap: introduction and
background
The gender pay gap – the third theme prioritized by the GEH – refers
to the difference in average earnings between men and women. Equal
pay refers to men and women performing the same role receiving the
same pay – that is, equal pay for work of equal value (Figure 5.1).
Gender pay equity was first defined by the ILO Equal Remuneration
Convention, 1951 (No. 100), which aimed to ensure that the work
done by men and women was compensated equally (124–126).
The Convention was the first of its kind, recognizing that women
were on the front line of production during the Second World War in
many countries and that there was a need to address gender pay
discrimination if equality was to be achieved (125). Almost 70 years
later the Convention is still relevant, as differences in pay remain the
most prevalent form of discrimination against women.
Figure 5.1 Equal pay versus the gender pay gap
EQUAL PAY
Means that mean and women
performing the same role must
receive the same pay
*for representation purposes only
THE GENDER PAY GAP
VS.
Indicates the difference in
average earnings between
men and women
$ $
=
29
Currently, awareness of the gender pay gap and the implications for
women of unequal pay are of higher profile politically than ever before,
and a global framework for action has been set within the SDGs.
SDG Target 8.5 aims to achieve “equal pay for work of equal value”
by 2030. Also, 2017 saw the launch of the Equal Pay International
Coalition, a multistakeholder partnership including ILO, UN Women
and OECD, established to drive concerted action to close the gender
pay gap. WHO is currently working with the ILO to analyse labour force
survey data for around 104 countries to generate more insights.
At the meeting of the G7 held in Canada 2018, commitments
were made to prioritize action on the gender pay gap as a way to
achieve economic equality. Measures such as prohibiting employers
from asking about previous salaries and ensuring some form of
transparency on pay determinations were prioritized. Following this,
gender equality and women’s empowerment, including reducing
the gender pay gap, have been put onto the agenda for the 2019
G7 meeting in France (127). Similarly, recognizing that no Group of
Twenty (G20) country has yet closed the gaps in women’s economic
participation, a political commitment was made by the G20 to reduce
these gaps by 25% by 2025 (128).
The SDG uses average hourly earnings for men and women as its
measure (Indicator 8.5.1). Differences in the methodology used lead
to different estimates of the gender pay gap. A 2018 ILO report on
the gender pay gap comparing average (mean) hourly wages for
men and women from 73 countries found a global gender pay gap
of 16% (129). Using a measure comparing median earnings of men
and women, however, increased the gap to 22%. A complementary
measure, the weighted gender pay gap, allows for the clustering
of men and women into different occupations, analyses gaps in
occupational subgroups and then weights them reflecting the size
of each subgroup in the total workforce. Using this methodology, the
mean hourly gender pay gap identified by the 2018 ILO data was
positive in all but two countries, and the mean hourly global gender
pay gap increased from about 16% to 19% (129). Clearly, adopting
the same measure would facilitate cross-country comparisons.
It is important to control for the difference in hours worked by men
and women and divide total compensation by hours worked to assess
the gender pay gap, since men may work more hours than women.
Women are more likely to work part time than men where the option
is available. Hourly wages, however, do not include bonuses, stock
options, and other forms of compensation that may be included in
annual salaries, particularly for higher-level positions. Since men are
more likely to hold positions of leadership where such benefits are
available, total compensation is a better measure than hourly wages
(130, 131).
It is also important to note that the gender pay gap, by definition,
measures paid work and so omits the substantial amount of unpaid
health and social care work done by women. In Lesotho, in response
to the increase in HIV/AIDS, women were expected to take up most of
the informal and predominantly unpaid care. There was no expectation
that men would work for free (108). Including unpaid work would
substantially increase the gender pay gap between men and women.
UN Women concluded that globally women earn 77 cents for every
dollar earned by men – a gap that will take an estimated 70 years to
close (132). In high-income countries women earn 75% of the pay
of their male counterparts, and in low-income countries, 83% (133).
ILO’s 2018 report found significant differences between countries,
with the mean hourly gender pay gap ranging from 34% in Pakistan to
–10.3% in the Philippines, meaning that women in the formal labour
market in the Philippines earn 10% more on average than men (129).
Globally women earn 77 cents for every dollar earned by men –
a gap that it is estimated will take 70 years to close.
Most of the studies evaluating the gender pay gap and the factors
contributing to wage differentials between men and women have
been based on data from high-income countries, especially the United
States. Due to limited data from low-income countries, there are
very few cross-country or regional comparisons. Currently the few
comparative studies that exist have compared high-income countries,
such as European countries (134).
As shown in Figure 5.2, the OECD collects data on the gender wage
(pay) gap for selected countries, with the highest gender wage (pay)
gaps found in Republic of Korea 34.6 %, Estonia 28.3%, and Japan
24.5 %, and the lowest found in Romania 1.5 %, Costa Rica 3.0
% and Luxembourg 3.4 % (135). Despite limitations, the current
evidence provides lessons to draw from and highlights the need
for more research to understand the factors driving variations in
the gender pay gap across and within countries and occupations,
particularly in low-income countries.
A literature review
30

5.3 The gender pay gap in the global
health workforce
In global health there is limited evidence on the gender pay gap
and an urgent need to understand it better. Evidence from low- and
middle-income countries is particularly limited. The 2017 Global
gender gap report estimated the average gender pay gap by country
at between 16% and 21% (30, 127). Figures from the ILO, however,
on the unadjusted gender pay gap in the health and social care
sectors, estimate it at higher than other sectors, at 26% in high-
income countries and 29% in upper-middle countries (1). Employment
sectors with a majority of female employees, such as health and
social care, are typically given lower social value and paid less. More
evidence with better methodologies is needed, particularly from low-
income countries, to identify gender pay gaps in the health and social
sectors, assess the causes and translate evidence into effective policy
measures.
The gender pay gap varies across different occupations within health
care. In the United States, the health care industry has one of the
largest gender pay gaps for any sector, and there are also large
differences in wages between professions in health (134). In the
United States, the number of women pharmacists has increased but
the gender pay gap persists (136). The gender pay gap still existed
amongst academic pharmacists, even after allowing for qualifications
and years of service. Similarly, the number of women taking up
anaesthesiology in the United States is increasing but female
anaesthesiologists still earn 25% less than their male counterparts
compared with a 17% gap for all physicians (137–139). One study
conducted in medical faculties in the United States concluded that
women were less likely to become full professors compared to men
and earned lower wages even after controlling for observable factors
(140). A recent survey of 65 000 physicians in the United States
revealed that women doctors earned an average of 27.7% less than
their male counterparts in 2017, a total average of US$ 105 000 less
in a year (141). One study from Australia found the average gender
pay gap to be 16.7% (142). Even in health sectors where women play
a large role, such as dentistry, they continue to earn less than their
male colleagues (45, 143).
A study from Australia showed that gender pay gaps tend to be
wider in high-paying jobs, and that men receive higher returns
to schooling compared to women (142). Association between the
gender pay gap and “family gap” is also significant (144). While pay
for fathers increases with the number of children, every additional
child a woman has is associated with a drop in pay (144). The most
likely explanation for this is that men with children are considered to
be more committed to their work, and thus deserving of and more
Figure 5.2 Gender wage gap by country
Note: 2017 or latest available data; based on data from OECD 2017
(https://data.oecd.org/earnwage/).
30200 10 40
Romania
Norway
Colombia
Hungary
France
Ireland
Spain
Cyprus
Netherlands
Portugal
Slovak Republic
Czech Republic
Finland
United States
EU (28 countries)
Latvia
Japan
Korea
Slovenia
Denmark
Luxembourg
Bulgaria
31

likely to be offered higher wages, whereas women with children are
considered less committed. Gaps vary, based on income levels, with
wider gaps amongst low-income women. Thus, the women who can
least afford it are not seen as deserving by employers and perceived
to lack commitment (142, 144).
Research also highlights that the gender pay gap between men and
women in medicine is connected with gender differences in specialty
choice and hours worked. However, recent studies suggest the gender
gaps in physician salaries persist even after controlling for specialty,
practice type, and hours worked (138). Women physicians also faced
trade-offs between career and family: one study found that women
physicians earned 11% less if they were married; 14% less if they
had one child; and 22% less if they had more than one child (145).
On one hand, there are studies that show the gap in wages converges
after controlling for observable factors such as specialty and numbers
of hours worked; while other studies show a disparity in physicians’
starting salaries. Limitations in these studies, due to methodological
differences or lack of comparable data, make it difficult to draw
conclusions, except that more and better research is needed to
identify gender pay gaps by men and women in comparable jobs,
medical sectors and levels, and the drivers of those gaps.
Figure 5.3 (37) shows the average female nurse earnings as a
percentage of men’s earnings, indicating that on average across all
nurse occupations women earned only 91% of what men earned.
5.4 Factors that contribute to gender
pay gaps
Research shows that both microeconomic and macroeconomic
factors affect the gender pay gap, and that there is a pay difference
between men and women regardless of the industry or profession
studied. Additionally, non-employment-related factors, such as
gender, race and ethnicity, create advantages for certain people, while
disadvantaging others (146). Disability is likely to be another important
factor. It is critical, depending on the context, that the gender pay gap
is analysed with an intersectional lens.
Initially, human capital factors associated with greater work
productivity, such as years of education, training, skill sets, number
of hours worked and years of work experience, were thought to be
major drivers of gender pay gaps. However, recent studies show that
even after controlling for such observable factors the gender pay gap
remains, and a large portion of the gap remains unexplained (142,
147–150). The 2018 ILO Global wage report (129) decomposed the
gender pay gap by human capital attributes, characteristics defining
job in a sector, and the type of workplace, and found considerable
variation between countries; however, on average, education and other
labour market factors explained relatively little of the gender pay gap
(129). The ILO concluded: “The unexplained part of the gender pay gap
generally dominates almost all countries, irrespective of income group.
In high-income countries, education contributes on average less than
1 percentage point of the gender pay gap, through it contributes much
more in some individual countries.”
“The unexplained part of the gender pay gap generally
dominates almost all countries, irrespective of income group.
In high-income countries, education contributes on average
less than 1 percentage point of the gender pay gap, through it
contributes much more in some individual countries.” 2018 ILO
Global wage report
The ILO concluded that this finding on education should not be
surprising, since in many countries women have higher educational
levels than men in the same occupational sectors but earn less.
Although lower-income countries and middle-income countries may
have a large percentage of women with low levels of education,
those women tend to be clustered in the informal rather than the
formal labour market, and so do not impact gender pay gap figures.
The report puts forward several drivers of the gender pay gap: the
fact that women are not paid equally for work of equal value; the
Figure 5.3 Female earnings as a percentage of men’s
earnings among full-time, year-round nurses (2011)
Source: United States Census Bureau (37).
878684 85 89
LPN/LVN
Average
(all nurses)
Nurse
anesthetists
Nurse
practicioners
Registered
nurses
88 90 91 92 93 94
A literature review
32

clustering of women into female-majority jobs and sectors giving less
value and lower rewards; and the “motherhood gap”, which varies
widely between countries and may be related to a number of factors
that affect working mothers, including constrained choices of more
“family-friendly” jobs, reduced hours, career interruptions, or gender-
biased hiring and promotion. Data from the report estimate that the
motherhood pay gap ranges from 1% or less in Canada, Mongolia
and South Africa to as much as 30% in Turkey (129). The drivers for
these significant differences need to understood and built into policy
measures.
Feminist economists have argued that use of gender as a dummy
variable in labour market analysis and wage regressions fails to
account for processes in which gender intersects with other social
stratifiers and how it shapes individual experiences of men and
women within the workforce as well as society at large. These
theorists argue that deeper understanding of discrimination is
required in labour market analysis, using feminist thinking (151, 152).
An important issue is the gendered social value given to professions
and jobs, which attaches greater value and rewards to work typically
done by men than to work typically done by women. This is highly
relevant for “caring professions”, such as nursing, which are female-
majority occupations.
Gender pay gaps are pervasive among all sectors, but they are greater
in private organizations compared to public sector and non-profit
sectors (153). It has been argued that this is because the public
sector is expected to act as a model employer that is more equitable
and value based (154).
Occupational segregation and job sorting by sex remain the leading
factor linked to the gender pay gaps, particularly in the health and
social care sector. Findings on occupational segregation in the
health sector are outlined in Chapter 3 of this review. Occupational
segregation is a dominant phenomenon within labour markets, with
women more likely to enter teaching and nursing jobs while men
enter more technical and mechanical professions. However, evidence
on trends in occupational segregation are not always available to
policy-makers, meaning they cannot make a connection between
low-paying jobs, in which women are often employed, and gender pay
gaps (94, 134, 155). Moreover, as stated above, a large part of the
gender pay gap remains unexplained. This means that studies have
found gender pay gaps in labour market analysis even after controlling
for observable factors such as specialty choice, work hours, or other
characteristics, and a large part remains due to “unexplained factors”
in the regression model (142, 147–149). Discrimination as well as
subtle and unconscious bias are often difficult to control for, and are
likely to be major drivers of gender pay gaps. However, putting these
complex terms in an “unexplained” error term is problematic, as it
gives no explanation on which to base policy (151). These gender
biases have implications for women’s careers, hiring rates, salaries
and promotions; hence, these unseen and unfair barriers women face
in the health care labour market will need to be addressed if we are
to reduce gender pay gaps (86, 134). Better research and context-
specific data are needed to deepen our understanding of gender pay
gaps within the health and social sector.
Gender biases have implications for women’s careers, hiring
rates, salaries and promotions; hence, these unseen and unfair
barriers women face in the health care labour market will need
to be addressed if we are to reduce gender pay gaps.
The fact that there are gender pay gaps in health care is a major
cause for concern at many levels as it implies that women, despite
being the majority of the global health workforce, are still unable to
gain respect and job status equal to their male counterparts. It is
estimated that almost US$ 160 trillion is lost globally due to gender
differences in earnings between men and women (162). Thus, the
gender pay gap remains a huge global health concern, since building
stronger and more resilient health systems would require that those
health systems enable women to participate in the workforce to their
full potential.
5.5 Why is addressing the gender pay
gap in the global health workforce
important?
Addressing the gender pay gap is critical to achieving fair and
resilient health systems. Gender differences in income have long-term
economic implications and lead to a gender wealth gap and poverty
for many women in old age (163). Wealth inequalities are gaining
interest among scholars as wealth accumulation increases financial
stability, opportunities, and purchasing power (164). Financial stability
and empowerment are also important factors in seeking health care
and continuing treatment, especially for women (165). The gender
pay gap therefore has implications for women’s own health outcomes.
Addressing gender equality and the elimination of discriminatory
practices in the workforce are closely linked.
33

Box 5.1 Factors contributing to gender pay gaps: key themes
INDIVIDUAL FACTORS
Differences in education, training, skills
Gender pay gaps exist even after controlling for differences in education, skill set, and training. The gaps widen with higher levels of
education for women, while men receive higher returns on schooling. Factors such as age, experience, specialty choice, and practice
settings also do not explain the gap (142, 156–158).
Differences in work experience
The gender pay gap widens with seniority (159). This phenomenon was found to be true for both physician and non-physician groups
of women (140). Large deficits in rank for senior faculty women were confirmed in logistic models that accounted for a wide range
of other professional characteristics and achievements, including total career publications, years of seniority, hours worked per week,
department type, minority status, medical versus non-medical final degree, and school (140). Gender gaps are also wider for higher-
salaried jobs (66).
Differences in numbers of hours worked, or part-time versus full-time work
Gender pay gaps are prevalent across almost all occupations but differ significantly in size. One factor that is associated with this
difference is whether an occupation is male dominated or female dominated, with male-dominated jobs being higher paid. Among
the many reasons for this is the difference in total number of hours worked, with women working fewer hours than men. Women face
constraints in balancing paid work with family responsibilities; hence they either opt out of the workforce or take up part-time work.
Women with children pay what is known as a “motherhood penalty”, whether as a single or married parent, as they are likely to work
less hours than men. The penalty is higher for women with low-paying jobs. Married men and those with dependent children, on the
other hand, gain a “fatherhood bonus” and have been found to earn higher wages than single men (142, 158, 160).
INSTITUTIONAL FACTORS
Occupational segregation
Industrial and job sorting of men and women into specific types of jobs substantially contributes to men’s higher compensation,
especially in the United States and Europe. Women are concentrated in primary health care, low-grade and low-paying jobs, the public
sector, and part-time employment (94, 134, 155). Low awareness of occupational segregation and the gender pay gap contributes to
maintaining the status quo (161).
Workplace authority
The pay gap widens at executive levels and with higher levels of education.
Hiring and promotion
Subtle unconscious biases in hiring and promotion processes have implications for women’s careers and advancements that impact
their earning potential.
Collective bargaining and unions
Men tend to be more likely to be part of networks and unions. Collective bargaining has been shown to be effective in negotiating
comparable salaries. When men participate in unions and women are not union members, then even the same hourly wages may lead
to pay differentials. Female-dominated jobs and sectors are still largely non-unionized, which has also led to gender pay gaps (134).
A literature review
34

Within the health workforce, it is important to address the gender pay
gap for multiple reasons, including the following.
• The gender pay gap is directly linked to poverty, as it has
implications for lifelong financial stability. Poverty affects women
at disproportionately higher rates compared to men (166), and
eliminating the gender pay gap could halve poverty levels for
women (167).
• Earning lower pay means lower pensions and less income from
social security for retired women compared to retired men (168).
Similarly, it means women qualify for lower disability and life
insurance benefits.
• Wage differences lead to lower morale and motivation to work
longer hours, or may cause women to quit the health workforce
altogether. With the majority of the health care workforce being
women, this has serious implications, as women may be more
likely to opt for working shorter hours and part-time jobs. With a
major and growing global shortage of health workers, addressing
the gender pay gap will improve the health workforce labour
supply, support achievement of universal health coverage, drive
economic growth, and help meet the health care needs of the
global population.
• Societal expectations of gender roles may lead women to either
delay marriage and childbearing until their thirties or to forgo it
completely. This phenomenon has long-term implications for the
health and well-being of societies (169, 170).
• Understanding patterns of the gender pay gap in a particular
context will drive solutions and more inclusive labour markets for
women. For example, if the widest gender pay gap is amongst
low-paid women workers, then minimum wage legislation, social
protection for women on the boundaries of the informal and formal
labour markets, and support for collective bargaining will be
critical. If the widest gap is amongst women in higher-status jobs
or mothers or fathers, then other policy solutions will be needed.
Despite advances in policies and reductions in the gender pay gap
over the years, a significant difference persists, calling for global
action to address the problem. In a recent survey on equal pay
conducted in the United States, it was found that almost one third of
Americans were not aware that the gap existed and men were twice
as likely to think it did not exist compared to women (156). In another
study, 80% of men thought their salaries were comparable to those
of women, compared to 41% of women who felt their incomes were
comparable to those of men (171). Thus, there is a need to increase
awareness of the problem in order to address it.
A major conclusion on the gender pay gap from this review is
that existing data and evidence are too scarce and not sufficiently
comparable to use as the foundation for policy measures in most
countries. Too much remains “unexplained”, and we need to move
beyond simple measures of the gender pay gap to more complex
methods that adjust for occupational segregation of men and women
(both horizontal and vertical), take an intersectional approach relevant
to the social context, and include the large numbers of women
working outside the formal, paid labour market. In the health sector,
addressing occupational segregation (Chapter 3) and the gendered
leadership gaps (Chapter 6) will both be critical to reducing gender
pay gaps.
35

6.1 Key messages
• Women make up 70% of the global health workforce but occupy
only 25% of leadership roles. Men hold the majority of leadership
roles in health at all levels, from global to community.
• The current gender gaps in leadership are predominantly a result
of power imbalances, gender stereotyping, discrimination and
structures that create pathways for one gender to excel while
others remain segregated in subordinated roles.
• Lack of gender balance in health leadership means global health
loses female talent, perspectives and knowledge. The women who
deliver global health do not have an equal say in its design and
delivery.
• Women’s limited opportunity to enter leadership roles is
compounded by the intersection with other factors such as race,
religion, caste, class and ethnicity, which can further disadvantage
women with more than one marginalized identity (for example, a
low-caste woman).
• There is evidence that women in leadership positions in health
expand the agenda, giving greater priority to rights – such as
sexual and reproductive health and rights – that apply to all
genders but, where absent, can have the most negative impacts on
women’s health.
• The persistent absence of female talent from leadership positions
is likely to prove a significant barrier to the rapid scaling up of the
global health and social care workforce needed to achieve the
SDGs, including universal health coverage.
6.2 Leadership and gender: background
Leadership is the fourth theme prioritized by the GEH. The current
gender gaps in leadership are predominantly a result of power
imbalances, gender stereotyping, discrimination and structures that
Chapter 6. Leadership
create pathways for one gender to excel while others remain segregated
in subordinated roles. Gender gaps in leadership are pervasive in all
sectors, including health. Women make up only 5% of the Fortune 500
CEOs (172); 24% of parliamentary seats (173); and 39% of the total
labour force (43). With the SDGs restating gender equality as a global
priority, addressing gender gaps in leadership is key.
6.3 Leadership and governance in the
global health and workforce
Leadership comes in many forms and it matters at all levels of global
health. Women are leaders in their communities providing health at
the front line, they are the first responders in outbreaks and disasters,
and they are predominantly the caregivers in their homes and family.
However, due to power structures within workplaces, women remain
underrepresented in top positions.
Women’s representation in top policy-making positions remains
low in global health agencies, with women holding around 25% of
the most influential leadership and governance roles. As shown in
Figure 6.1, an evaluation of 140 global health organizations found
that decision-making power remains largely in the hands of men,
with 69% of organizations and 80% of organization boards led by
men (82). Moreover, beyond gender parity, women have less visibility,
less recognition and less influence than men. This shapes the health
agenda and resources at all levels – even at the community level.
Anecdotal examples of the contribution made by community health
workers is important in capturing the impact women are having on
the health of their communities, but most have little or no opportunity
for promotion to more influential leadership roles. This applies across
health professions. Most recently, nurses and midwives, in response
to leadership disempowerment, have launched the Nursing Now 2020
campaign, with one key goal being to have nurses or midwives in
leadership roles and on governing boards at all levels in health (174).
The gender gap in health leadership goes beyond the numbers.
Deep-rooted power structures, including patriarchal and gender bias,
creates a preferential opportunity for men to be leaders in the mostly
A literature review
36

powerful, influential roles in society. In the health sector, especially
given the historical structure of hospitals and health systems based on
hierarchy and patriarchy, the power relations create an environment
that enables men and disempowers women, limiting their ability
to reach their maximum potential as leaders. A contextual analysis
of women in the health workforce shows there are unique barriers
women face based on gender. They are less invested in and supported
in their roles, as they operate in environments that are not enabling
for all genders (2).
In the health sector, especially given the historical structure of
hospitals and health systems based on hierarchy and patriarchy,
the power relations create an environment that enables men
and disempowers women, limiting their ability to reach their
maximum potential as leaders.
One study identified those positions that embody power, influence
and leadership as the “final male bastions” and noted that women
are less likely to be in positions of power and authority, have the
opportunity to advance, be rewarded for the work they do, and find
themselves in strong support networks (175). These positions of
power and leadership roles in global health can take on many forms,
from the executive team of a United Nations agency to the head of
a community nongovernmental organization or to the head of a local
health clinic. While leadership is often linked to the most senior and
well paid positions, one can be a leader at all levels, including in
underpaid or underrecognized roles in health.
Across the health workforce, women are underrepresented in the
upper levels of management, leadership and governance. Only 31%
of ministries of health are led by women (176, 177). At the high end is
the Africa Region with 38%, with South-East Asia at the low end with
18% of ministries of health led by women (177) (Figure 6.2).
In examining health leadership, Women in Global Health found on
average 25% of Member State chief delegates, to the World Health
Assembly, were women, increasing over time, since 2005, as seen
in Figure 6.3. (101). Percentages of women 2016-2016 were
26%, 31% and 29% respectively. In many cases this mirrors the
underrepresentation of women in the senior levels of ministries of
health. For example, women held only 20% of senior roles in the
Ministry of Health in Cambodia (178). However, there is an opportunity
to transform the health leadership to be more representative of the
largely women-led health workforce (Figure 6.4).
The majority of the reviews of leadership in the health workforce have
previously focused on women’s leadership in medicine. Emerging
literature has started exploring trends in other sectors, for example,
the work undertaken by the Nursing Now campaign. Similarly,
another study in 2006 found that despite increasing numbers of
women in pharmacy, they are still underrepresented in leadership
roles (136). Research is expanding beyond the United States; for
example, one study found that women are underrepresented in
prestigious specialisms and leadership roles regardless of the rate at
which women are entering the health sector in a country (45). Within
anaesthesiology women’s leadership is lower than in other medical
professions in the United States (179). Looking at the leadership in
the World Federation of Societies of Anaesthesiologists, a striking
Figure 6.1 Who leads global health organizations?
Executive Directors
20% 80%31% 69%
Board Chairs
Source: Global Health 5050: https://globalhealth5050.org/gh5050-summary-findings-on-leadership-and-parity/.
37

Figure 6.2 Percentage of Member State ministries of health headed by women, by WHO
Source: Women in Global Health, 2018
36%
64%
31%
69%
39%
61%
19%
81%
18%
82%
24%
76%
Figure 6.3 Women’s representation as chief delegates at World Health Assembly, 2005–2015
Source: Women in Global Health, 2018
Gender representation at the World Health Assembly 2005- 2017
HOW CAN WE ACHIEVE GENDER PARITY IN GLOBAL HEALTH?
@WomeninGH
WomeninGH
www.womeningh.org
2005
16%
WOMEN
2015
22%
WOMEN
2017
31%
WOMEN
A literature review
38

lack of representation can be observed across boards (5:1, men:
women), councils (15:5) and committee chairs (9:1) (180). There
are gender gaps in academic medicine as well, for example, in the
top 50 American medical schools only 24% of the directors were
women (181). A gender analysis of Kenya’s health training institutions
found that women made up 76% of the nursing profession, but men
held 62% of the faculty positions (182). One study found that men
with 15 to 19 years of experience were 17% more likely to hold full
professorships when compared to women with the same years of
experience, even after adjusting for other factors such as number of
publications and degrees (160).
6.4 Why addressing gender gaps in
leadership matters
Addressing gender gaps in leadership sets the agenda for equal
representation of genders at all levels of the organization as well
as across different sectors of health. It leads to a more empowered
workforce, improved motivation, reduced attrition, improved quality of
care, and better understanding of health systems, which feeds into
designing more suitable solutions (183).
Addressing gender gaps in leadership leads to a more
empowered workforce, improved motivation, reduced attrition,
improved quality of care, and better understanding of health
systems, which feeds into designing more suitable solutions.
There is a need for the diversification of leadership in the health
workforce. Across sectors women are seen to exhibit transformational
leadership qualities, including those that focus on motivating others,
supporting the advance of the whole team while attending to individual
needs, and creating excitement about the future, more frequently than
men. With these foundational qualities, studies have confirmed that
overall women were seen as more effective leaders (184). Within the
health sector, there is some evidence to indicate the same. Several
studies in India indicated that women leaders in health have resulted in
positive benefits such as the reduction of neonatal mortality, increased
expenditure on health facilities, antenatal care and immunizations, and
prioritization of issues traditionally related to women (181). Evidence
also shows that providing nurses with the opportunity to lead and shape
health services leads to improvements in health outcomes and supports
innovation, recruitment and retention (185).
6.5 Factors contributing to leadership
gaps in the global health workforce
The lack of women in leadership is often said to result from a “glass
ceiling”, but recent literature aptly identifies that the lack of women
in leadership is more the result of a labyrinth, a twisting and turning
series of barriers that are both visible and invisible, rather than a
sudden and clear limit that prevents women from reaching the final
upper level of leadership (186). There are a multitude of barriers faced
by women in advancing in leadership. These barriers exist at the
individual, interpersonal, institutional, and community levels, and up
Figure 6.4 Global health leadership pyramid
Source: Women in Global Health, 2018
1. Fortune 500 list for healthcare sector, Fortune, 2018
2. Global Health 50/50 Report, Global Health 50/50, 2018
3. World Health Organization Member States, Womean in
Global Health (data) unpublished), 2018
4. Work Health Organization’s World Health Assembly List of Delegates and Other
Participants, Women in Global Health (data unpublished), 2018
5. QS World Ranking 2018: Top 25 Global Universities for Public Health and Medicine, 2018
6. Improving employment and Working conditions in health services, international Labour
Organization, 2017
7. Improving employment and Working conditions in health services, international Labour
Organization, 2017
Women’s representation in global health leadership, based on influence
Fortune 500
Healthcare CEOs
(1)
Heads of
global health
organizations
& boards of
global health
organizations
(2)
Ministers of
Health (3)
World Health
Assembly heads
of Delegations
(4)
Deans of top
Public Health &
Medical Schools
(5)
Health
and Social
Workforce (6)
Long-Term Care
Workforce (7)
3.7%
25%
31%
27%
28%
70%
90%
= 10%
39

to the public policy level. The global health and social workforce has
a problem which is not limited to a “glass ceiling effect”. Rather, the
whole pipeline is leaking women all the way up to the top. (187).
The lack of women in leadership is more the result of a
labyrinth, a twisting and turning series of barriers that are
both visible and invisible, rather than a sudden and clear limit
that prevents women from reaching the final upper level of
leadership.
It is important to note that gender is only one dimension of the
labyrinth that women in the health workforce must negotiate on
their way to leadership. There are multiple ways to understand
marginalization within health systems leadership. For example, a
unitary approach focuses on one primary marker of difference as
sufficient for explaining a social problem, in isolation from other
markers (for example, gender as separate from race) (188); a
multiple approach considers more than one explanatory factor but
does so in an additive manner (for example, gender plus race equals
greater disadvantage) (188); and an intersectionality approach
explicitly focuses on the relationships between factors and mutually
constructed processes that lead to social differences. Inequities are
never the result of single, distinct factors; rather, they are the outcome
of intersections of different social locations, power relations and
experiences (189). Gender as one aspect of an individual’s identity
plays a major role in a person’s experience of the world, including
professional development and career advancement. However, not
acknowledging the dynamic interconnectedness of gender with other
social identities, especially when considering women who do not fulfil
the “white woman from the West” benchmark, is a pitfall that hinders
adoption of solutions that benefit all women. And this benchmark is
the typical image used to portray most women in leadership positions.
The majority of the reviews and studies found similar barriers to
women advancing within their professions and reaching leadership
positions across geographies and occupations. They include the
following.
• Overall gender norms and expectations of men and women
negatively impact women’s advancement to leadership (115, 190).
Traditional gender norms do not portray women as leaders, and
leadership qualities are associated traditionally with masculine
traits. Women are perceived as having more communal traits,
leading to a double bind if they exhibit leadership traits perceived
as traditionally masculine (184). In Uganda and Zambia,
gender norms and the understanding of key leadership traits
negatively impacted the advancement of women and skewed
the organizational processes leading to leadership – such as
hiring and promotion – as leadership itself was gendered (190).
Leadership stereotyping is only one way in which gender norms
impact women’s advancement in the health workforce. One study
noted that gender norms influenced women’s progression to
leadership at three intersecting levels – individual, household and
community – as shown in Box 6.1 (178).
• Bullying and sexual harassment have negatively impacted women’s
advancement to leadership positions (191, 194). Adverse systemic
consequences include “impediment of health workers’ advancement,
increased stress and decreased morale and productivity”, and
a “limited pool of health workers to deal with today’s health
challenges” (5). The story of Dr Caroline Tan, an Australian
neurosurgeon, personifies the impacts of sexual harassment and
assault on women’s career advancement in health care. Dr Tan, who
won a tribunal case against a fellow surgeon, faced targeted attacks
by the perpetrator to undermine her credibility, a delay in the award
of her fellowship by the Royal Australian College of Surgeons, and
difficulty in securing a position, despite high examination scores and
excellent references (195).
• The interrelationship between horizontal occupational segregation
and the occupational leadership hierarchy within the health
workforce has influenced women’s career advancement and the
way women leaders are represented. In Jordan, a study found
that two thirds of men in the health workforce were doctors,
whereas almost 80% of nurses were women, while men held
90% of managerial positions (196). It was noted that in South and
Central Asia, nursing was seen as a low-status profession and
nurses were directly managed by doctors who served in the main
decision-making roles (186). Nurses were seen as “extra hands”
for doctors, and were presented with few or no opportunities for
career advancement and leadership (186). The Review Board of
the All-Party Parliamentary Group on Global Health in the United
Kingdom found “overwhelming evidence” that nurses in leadership
were not being engaged adequately in policy-making or decision-
making at all levels, from local to global (186).
• Women often report that lack of recognition and respect is a
detriment to their career advancement and entry into leadership
roles. One study found that women received only 1 in 10 awards in
health and medicine (197), while another study found that female
A literature review
40

Box 6.1 Individual, household and community
dimensions of gender stereotyping
INDIVIDUAL
In Cambodia, it was shown that gender norms affected how
men and women engaged in the health sector, and in turn
their progression to leadership (115).
HOUSEHOLD
Regardless of organizational policies, women were held back
by gendered time use. In Cambodia, women’s advancement
was impacted by family responsibilities (115). In Japan, women
in medicine saw a “motherhood penalty” with reduced hours
worked, and several years of unemployment during early
child-rearing, with consequences for their access to leadership
(45). Even in Scandinavia, where policies and cultural attitudes
promote work–life integration, women were more likely to
switch from specialties and leadership tracks after childbirth
to positions that provided more flexibility with childrearing (45).
A study of women doctors in the United Kingdom attributed
the lack of women’s leadership roles to the rigidity of career
paths leading to leadership within medicine, and reliance on
a hierarchical system that disregards the modern needs of
people to balance career expectations with other responsibilities
outside work (191).
COMMUNITY
In a review of the post-conflict health system in Cambodia,
women had reduced clinical time due to community
expectations of gender roles. For example, women reported
being unable to work night shifts due to disapproval from the
community (115). In Zimbabwe, men were more likely to be
selected for very remote and rural areas, where they were
able to gain invaluable career experiences. These experiences
supported men’s career advancement over women through
increased promotions, and participation in international
trainings and workshops (192). In Afghanistan, women were
able to gain increased access to resources at the community
level as community health workers, due to gendered social
norms, but men were more likely to hold leadership positions
and in turn control resource allocation (193).
managers felt that their voices were not as respected as those
of their male colleagues, and also faced additional discrimination
due to younger age or perceived lower technical skills (198).
In Pakistan, where the requirement for lady health workers to
travel to people’s houses and to work with men clashed with
cultural norms, lady health workers reported lack of respect and
devaluation of their work (199).
• These studies also highlight the need for a deeper analysis of
the detrimental impact that gender inequality in health workforce
leadership is likely to have on health outcomes.
Removing gender gaps in leadership roles makes good business sense.
It leads to the creation of a workforce pipeline that supplies educated,
trained and skilled health workers using 100% of the talent pool.
41

This chapter brings together the findings of the GEH literature review,
draws conclusions, and outlines next steps. All these will influence
gender equity in the health workforce. Since countries have different
starting points in terms of health systems, resource levels, health
worker supply, gender equality and socioeconomic context, there
can be no universal blueprint for addressing gender equality in the
health workforce. All policy measures will need to be contextualized to
suit the local situation, with all genders in the local health workforce
having a voice in the decision-making process.
The findings of this report and the Gender at Work framework (200)
will form the foundation for the next phase of gender policy work by
the GEH, with the aim of supporting country-level implementation and
measurement of context- and evidence-based policy solutions.
7.1 Policy context
The Sustainable Development Goals (SDGs), the overarching
goal to reach universal health coverage, the Global Strategy on
Human Resources for Health, and the joint WHO, ILO and OECD
Working for Health five-year action plan (Box 7.1) together create
a strong platform for addressing the gender inequality that causes
inefficiencies in the health workforce. They also set a timetable, since
the commitments of the five-year action plan are to be delivered by
2021, and the SDGs, universal health coverage and Global Strategy
on Human Resources for Health have a timeline of 2030.
There is no health without the people who deliver health care.
With growing global demand for health care and a projected health
worker shortage, there is an urgent need to scale up the numbers of
new health worker jobs in high-, middle- and low-income countries.
Since women form the majority of health and social care workers,
the Working for Health five-year action plan 2017–2021 recognizes
the importance and urgency of addressing gender inequity in the
health workforce. The deliverables of the plan include gender-
SECTION 3. CONCLUSIONS
Chapter 7. Conclusions: policy context,
findings, and next steps
transformative policy development and implementation capacity to
overcome gender inequities and form the foundation for the work of
the GEH, including this report.
Box 7.1 Working for Health: five-year action
plan for health employment and inclusive
economic growth 2017–2021 (WHO, ILO, OECD)
RECOMMENDATION 2
Maximize women’s economic participation and foster their
empowerment through institutionalizing their leadership,
addressing gender biases and inequities in education and the
health labour market, and tackling gender concerns in health
reform processes.
DELIVERABLES
2.1 Gender-transformative global policy guidance developed
and regional and national initiatives accelerated to analyse
and overcome gender biases and inequalities in education
and the health labour market across the health and social
workforce (for example, increasing opportunities for formal
education, transforming unpaid care and informal work into
decent jobs, equal pay for work of equal value, decent working
conditions and occupational safety and health, promoting
employment free from harassment, discrimination and
violence, equal representation in management and leadership
positions, social protection/child care, and elderly care).
2.2 Gender-transformative policy development and
implementation capacity to overcome gender biases and
inequalities in education and the health labour market
supported.
A literature review
42

Horizontal and vertical occupational segregation by gender is a
universal pattern in health, varies with context.
Driven by gender norms and stereotypes of jobs culturally labelled
‘men’s’ or ‘women’s’ work
Gender discrimination constrains women’s leadership/seniority
Gender stereotypes constrain men eg entering nursing
Women in health typically clustered into lower status/lower paid
jobs
Female majority professions given lower social value, status & pay
Women 70% global health workforce but hold only 25% senior roles
Gender leadership gaps driven by stereotypes, discrimination, power
imbalance, privilege
Women’s disadvantage intersects with/multiplied by other identities eg
race, class
Global health weakened by loss female talent, ideas, knowledge
Women leaders often expand health agenda, strengthening health for all
Gendered leadership gap in health is a barrier to reaching SDGs and UHC
Large % women in health workforce face bias and discrimination
Female health workers face burden sexual harassment causing
harm, ill health, attrition, loss morale, stress
Many countries lack laws and social protection that are the
foundation for gender equality at work
Male healthworkers more likely to be organised in trade unions
than female
Frontline female healthworkers in conflict/emergencies/remote
areas face violence, injury & death
GPG in health 26-26%, higher than average for other sectors
Most of GPG in health is unexplained by observable factors eg
education
Occupational segregation, women in lower status/paid roles, drives GPG.
Much of women’s work health/social care unpaid and excluded in GPG
data
Equal pay laws and collective bargaining absent in many countries
GPG leads to lifetime economic disadvantage for women
Closing GPG essential to reaching SDGs
OCCUPATIONAL
SEGREGATION LEADERSHIP
DECENT WORK:
DISCRIMINATION SEXUAL
HARASSMENT BIAS
GENDER PAY GAP (GPG)
7.2 Findings of the GEH literature
review
The findings of the GEH literature review are divided into two parts:
1. findings from each of the four focus areas covered by the report;
2. overarching findings and conclusions generated from the exercise.
The following subsections highlight what the literature review found –
or did not find – in the sources that were reviewed.
7.2.1 Key findings of the GEH literature review on the
four focus themes
Key findings from the four focus areas of the GEH literature review
are summarized in Figure 7.1. Each theme is explored in depth in a
separate chapter of this report.
Figure 7.1 Key finding in four focus areas of GEH literature review
7.2.2 Overarching findings from the GEH literature
review
Of the eight overarching findings (summarized in Figure 7.2), five
highlight serious deficiencies in data and research, which limit
compilation of a comprehensive global picture upon which to base
policy.
First, the majority of the 170 studies identified and reviewed in this
report come from the global North and report findings from the
global North, many of which are not transferable to settings with
different cultures and resource levels. There are major gaps in data
and research from all regions, but the most serious gaps on gender
and equity in the health workforce are in low- and middle-income
countries. This is of particular concern since the most rapid and
radical progress is needed in low- and middle-income countries to
reach the SDGs, attain universal health coverage and achieve the
health for all targets by 2030.
43

In addition, widespread gaps in the data and literature were found from
countries of all income levels on implementation, application of gender-
transformative policy measures and what works to change the health
system weaknesses and deficiencies caused by gender inequality. This
will be an important focus for the work of the GEH going forward.
Major gaps and lack of comparable data were also found in countries
from all regions. Examples include sexual harassment and gender
pay gap data. Despite the prominence the #MeToo movement has
given to the issue of sexual harassment in the last year, a disturbing
59 countries still lack legislation prohibiting sexual harassment in
the workplace. The #MeToo movement has prompted women in
health in some countries to speak about their experience of sexual
harassment and abuse at work. Although, from confidential reports,
sexual harassment of female health workers by co-workers, patients
and members of the community appear to be widespread, with
consequent harm both for women affected and for health systems,
systematic collection of data and research studies are not common. A
supportive legal framework and data collection are the starting points
for identifying patterns of and trends in sexual harassment, abuse
and violence suffered by female health workers and putting in place
preventive measures and support for survivors.
Similarly, with the gender pay gap, data collection is uneven and not
always comparable across countries, while several studies conclude
that much of the gender pay gap is “unexplained” by observable
factors. Clearly, research is needed to explain the “unexplained” and
identify solutions to inequities in pay, which have serious lifelong
impacts for women’s income, autonomy and well-being.
Figure 7.2 Key overarching findings of GEH literature review
Finally, in the list of deficiencies in the data and literature, studies
identified for the review were limited in methodological approaches.
Although in many countries female health workers are clustered into
different sectors of health and social care by social identities such
as race, ethnicity, class, and migrant status, very few studies take
an intersectional approach to highlight how gender disadvantage in
employment can be compounded by other social identities. Some
countries are now investigating pay gaps based on disability and race,
in addition to gender. It is critical to take an intersectional approach to
understand how multiple identities interact with gender in the health
workforce to compound inequity.
Three further overarching conclusions from this review also need
emphasis. The first is the near universal and pronounced occupational
segregation of women and men within the health workforce. This
report emphasizes that the fast-growing health and social care sectors
are important employers of women and critical drivers of economic
growth. But although women hold around 70% of jobs in the health
workforce, they remain largely segregated within it, both vertically
and horizontally. Vertical segregation, with men holding the majority of
higher-status, higher-paid roles, is a pattern found in most countries.
It is particularly acute in the health and social care sector, resulting in
an estimated gender pay gap higher than the average for other sectors
of the economy. It is a paradox that even in female-majority health
professions, such as nursing, the small minority of male employees
often have a “glass escalator” to the top, reaching leadership positions
faster than their female colleagues. Women in the health workforce
are disadvantaged by being clustered into lower-status and lower-
paid (often unpaid) roles, and are further disadvantaged by horizontal
OCCUPATIONAL
SEGREGATION LEADERSHIP
DECENT WORK:
DISCRIMINATION SEXUAL
HARASSMENT BIAS
GENDER PAY
GAP (GPG)
Overarching Findings from literature review:
• 170 studies in this review, most from global North
• Major gaps in data and research from low- and middle-income countries (LMICs) on
gender and equity dimensions health workforce
• Major gaps in implementation research on impact of policy change or gender
transformative approaches in different cultural settings
• Major gaps in data in all areas, particularly sexual harassment and data comparable
across countries on the gender pay gap
• Studies limited in methodological approaches. Very few adopt an intersectionality
lens or use mixed methods approaches
• Occupational segregation, vertical and horizontal, is major driver and consequence
of gender inequality
• Critical role of women in health (70% health workforce) is often overlooked, so
priority not given to addressing gender/equity in workforce
• Gender inequality in health and social care workforce will limit delivery of UHC &
health for all
A literature review
44

occupational segregation resulting from gender norms and stereotypes
that brand some jobs in health more suitable for women (nursing) or
men (surgery). Women are then triply disadvantaged by social gender
norms that attach lower social value to majority female professions and
thereby devalue the status and pay of those professions.
Occupational segregation in the health sector is driven by gender
inequality and, in turn, is the foundation for other gender inequalities
identified in this report. Occupational segregation in the health
workforce drives the gender pay gap and also makes lower-status
female health workers, often on insecure contracts and less unionized
than men, more vulnerable to sexual harassment, abuse and violence.
There is nothing inevitable about occupational segregation by gender
in the health workforce. Education and employment patterns in many
countries have changed rapidly over the last 25 years with far more
women entering medicine and, in some countries, now forming the
majority of medical students. Countries vary, for example, in the
percentage of men in nursing. Occupational segregation in health is not
fixed over time or across countries and policy measures can be taken to
change it. In its next phase of work, the GEH will identify good practice
examples to see what lessons can be learned and transferred.
A second and related point is that, despite women being the majority
of the global health workforce, their role as drivers of health is often
unacknowledged. Trends in applications for medical training show that
health as a profession continues to attract women and is likely to remain
a major employer of women. The lack of acknowledgement of women’s
role, however, contributes to a lack of priority given to addressing
gender inequality in the health workforce. This has to change fast, with
gender-transformative policies and measures put in place if global
targets such as universal health coverage are to be achieved.
Critical and also largely unacknowledged is the burden of unpaid
health and social care work typically done by women and girls caring
for sick and disabled family and community members. Women also
perform (unpaid) voluntary roles in health promotion and service
delivery. This review has focused on findings from the formal labour
market and a priority going forward will be to gather evidence on the
unpaid health and social care work that forms an insecure foundation
for the global health pyramid. Women’s unpaid work must be recorded
and valued, with measures put in place to enable women and girls
engaged in unpaid work to access education, training and the formal
labour market, where their work would be counted and paid.
Finally, a key conclusion of this report is that gender inequality in
the health and social workforce weakens health systems and health
delivery. However, an alternative, far more positive future scenario is
possible. Addressing gender inequalities in global health and investing
in decent work for the female health and social workforce will have
a wider social and economic multiplier – a “triple gender dividend” –
comprising the following.
• Health dividend. The millions of new jobs in health and social care
needed to meet growing demand, respond to demographic changes
and deliver universal health coverage by 2030 will be filled.
• Gender equality dividend. Investment in women and the education
of girls to enter formal, paid work will increase gender equality and
women’s empowerment as women gain income, education and
autonomy. In turn, this is likely to improve family education, nutrition,
women and children’s health, and other aspects of development.
• Development dividend. New jobs will be created, fuelling economic
growth.
This triple gender dividend will improve the health and lives of people
everywhere. The health and social care worker shortage is global, and
addressing gender inequality in the health workforce is everybody’s
business.
7.3 Next steps
This literature review is the foundation for the next phase of the work
of the Global Health Workforce Network GEH, which will use these
findings, together with an analysis of best practices from within and
beyond the health and social sector, to inform gender-transformative
policy and action.
To advance this work, the GEH will develop advocacy and policy
toolkits to target key stakeholders, including WHO Member States, to
integrate gender-transformative health and social workforce policies
into their national health workforce plans.
The GEH will also bring together various actors at the national level
to design and evaluate gender-transformative health workforce
policy interventions, with the aim of supporting implementation and
measurement of context- and evidence-based policy options. This
will provide a platform for policy-makers to collaborate with key
governmental partners and external experts.
Finally, the GEH will convene a review in 2019, midway through the
Working for Health five-year action plan 2017–2021, supporting WHO,
ILO and OECD to assess progress on the two action plan deliverables
on gender equality and, on the basis of that review, recommend steps
to ensure the achievement of these deliverables by 2021.
45

Bias is an inclination or prejudice for or against one person or group, especially in a way considered to be unfair, that often results in
discrimination (5).
Decent work is defined by the ILO as “the aspirations of people in their working lives. It involves opportunities for work that is productive
and delivers a fair income, security in the workplace and social protection for families, better prospects for personal development and social
integration, freedom for people to express their concerns, organize and participate in the decisions that affect their lives and equality of
opportunity and treatment for all women and men” (201).
Discrimination in employment and occupation includes practices that place individuals in a subordinate or disadvantaged position in the
workplace or labour market because of characteristics (race, religion, sex, political opinion, national extraction, social origin, or other attribute)
that bear no relation to the persons’ competencies or the inherent requirements of the job (5).
Feminization is the movement of women into traditionally male-dominated occupations (202).
Gender is a social construction reflecting the distribution of power between women and men, girls and boys and gender-diverse persons. This
distribution of power is influenced by history, laws, policies and politics, and by economic, cultural, community and family norms that shape the
behaviours, expectations, identities and attributes considered appropriate for all people – women and men, girls and boys, and gender-diverse
people. How an individual expresses their gender identity varies across context, time, and place, and throughout their life-course. Gender
interacts with, but is distinct from, the binary categories (male, female) of biological sex. When a person’s gender identity does not correspond
with their assigned sex, they may identify as transgender (2). Gender also intersects with, and is shaped by, other axes of inequality – age,
education, economic position and power, race, and ethnicity.
Gender blind refers to the failure to recognize that the roles and responsibilities of men and boys, and women and girls, are assigned to them
in specific social, cultural, economic, and political contexts and backgrounds. Projects, programmes, policies and attitudes that are gender blind
do not take into account these different roles and diverse needs. They maintain the status quo and will not help transform the unequal structure
of gender relations (203).
Gender discrimination describes any distinction, exclusion, or restriction made on the basis of socially constructed gender roles and norms that
prevents a person from enjoying full human rights. It can be direct or indirect, or overt or covert, and is associated with negative consequences
for the person who experiences it (5).
Gender equality in the health workforce describes a condition whereby men and women can enter the health occupation of their choice,
develop the requisite skills and knowledge, be fairly paid, enjoy fair and safe working environments, and advance in a career without reference
to gender. It implies that workplaces are structured to integrate family and work and to reflect the value of caregiving for men and women (204).
Gender equity is the process of being fair to all genders. To ensure fairness, measures must often be put in place to compensate for the
historical and social disadvantages that prevent women and men from operating on a level playing field. Equity is the process by which equality
can be achieved as an outcome (205).
Glossary
A literature review
46

Gender pay gap encompasses differences in men’s and women’s average earnings, which refer to (a) remuneration in cash or in kind paid to
an employee for the work done, together with remuneration for time not worked; (b) net earnings from self-employment; or (c) total earnings
from both employment and self-employment (125).
Gender-transformative policies and programming include policies and programmes that seek to transform gender relations to promote
equality and achieve programme objectives. This approach attempts to promote gender equality by (a) fostering critical examination of
inequalities and gender roles, norms, and dynamics; (b) recognizing and strengthening positive norms that support equality and an enabling
environment; (c) promoting the relative position of women, girls, and marginalized groups; and (d) transforming the underlying social structures,
policies, and broadly held social norms that perpetuate gender inequalities (206).
Health workforce is defined by WHO as “all people engaged in actions whose primary intent is to enhance health”, including those engaged
in direct care roles (such as physicians, nurses, midwives, pharmacists, and dentists), leaders, policy-makers, researchers, management and
support staff (such as ambulance drivers and accountants). This review focuses on direct care providers (207).
Horizontal segregation refers to differences in types of occupations and sectors in which men and women are concentrated. Greater numbers
of women, for example, are concentrated in low-paying, part-time and unpaid care or domestic work as compared to men (19).
Intersectionality is a feminist theory and analytical tool for understanding and responding to the ways in which gender intersects with other
identities to create new oppressions. The experiences of marginalization and privilege are defined not only by gender but also by other identity
factors such as race, class, age, religion and sexual orientation, all of which are determined, shaped by, and embedded in social systems of
power. Intersectional paradigms view such characteristics as race and class as mutually constructed systems of power that require special
measures to reach women who face multiple forms of discrimination (191).
Non-binary, also referred to as genderqueer, is a category for gender identities that do not conform to the gender binary of masculine or
feminine. Non-binary people may express a combination of masculinity and femininity, or neither, in their gender expression. Those who
incorporate aspects of both male and female may identify as “androgynous”, “mixed gender” or “pangender”, while those who move between
genders in a fluid way may identify as “bigender”, “gender fluid” or “pangender”. Some people who move between two or more than two
genders identify as “trigender” or “pangender”. Some people identify with an additional gender, known as “third gender”, “other gender”
or sometimes “pangender”. Note that “pangender” is a flexible term. People with no gender identify as “agender”, “gender neutral”, “non-
gendered”, “genderless”, “neuter”, or “neutrois” (208).
Occupational downgrading is a phenomenon “where women choose employment below their skills level and accept poorer working
conditions” (29).
Occupational segregation is the distribution of workers across and within occupations (24).
Occupational gender segregation is the difference in the types of jobs men and women enter (19).
Sexual harassment refers to unwelcome sexual advances or requests for sexual favours, whether verbal, physical, or visual. These behaviours
are illegal if the submission to such behaviours is made a condition for employment or a decision affecting the individual, or has the purpose of
interfering with an individual’s performance (209).
Substantive equality is a principle that considers the effects of past discrimination, recognizes that rights, entitlements, opportunities and
access are not equally distributed throughout society, and accepts the need to sometimes treat people differently to achieve equal results.
It allows for differential treatment to level the playing field for women, particularly where structures of dominance and subordination are
embedded in the baseline of opportunity (191).
47

Tokenism refers to a phenomenon whereby an organization includes a representative from a minority or disadvantaged social group in an
activity or position only in order to give an appearance of fairness and inclusion. It may be said to occur in the workplace when one group
represents less than 15% of an organization. The members of that group may be subject to predictable forms of discrimination (210).
Toxic masculinity refers to stereotypical masculine behaviours associated with the male gender. It includes the social expectation for men to
act in a dominant or “alpha male” manner. These expectations restrict men and boys from expressing their emotions or being affectionate, and
limit their emotional range to such negative expressions as anger (211). Toxic masculinity also leads men and boys to engage in higher-risk
behaviours such as use of alcohol or tobacco, violence, and aggressive driving (212). This is also related to the concept (introduced by R.W.
Connell) of “hegemonic masculinity” – an attitude that legitimizes men’s dominance over women and other gender identities that are perceived
to be feminine in a given society (213).
Unpaid care work refers to all unpaid services provided within a household for its members, including care of persons, housework and
voluntary community work (29). These activities are considered work because theoretically one could pay a third person to perform them.
“Unpaid” indicates that the individual performing the activity is not remunerated. “Care” refers to the activity that provides what is necessary for
the health, well-being, maintenance, and protection of someone or something. “Work” refers to an activity that involves mental or physical effort
and is costly in terms of time resources (29). This includes services provided by community health workers that are unpaid or on a voluntary
basis.
Vertical segregation refers to the concentration of men and women in different positions of power, leadership and decision-making, for
example, men dominating leadership positions and political life compared to women (19).
Women’s rights. The Beijing Platform for Action, in paragraph 2 of its mission statement, states: “The Platform for Action reaffirms the
fundamental principle … that the human rights of women and of the girl child are an inalienable, integral and indivisible part of universal human
rights. As an agenda for action, the Platform seeks to promote and protect the full enjoyment of all human rights and the fundamental freedoms
of all women throughout their life cycle” (214).
Workplace violence includes physical assault, verbal abuse, sexual or racial harassment, bullying or mobbing (5).
A literature review
48

1. Improving employment and working conditions in health services.
Geneva: International Labour Organization; 2017.
2. Langer A, Meleis A, Knaul FM, Atun R, Aran M, Arreola-Ornelas
H et al. Women and health: the key for sustainable development.
Lancet. 2015;386(9999):1165–210.
3. Final report of the expert group to the High-level Commission on
Health Employment and Economic Growth. Geneva: World Health
Organization; 2016.
4. GBD 2016 mortality collaborators. Global, regional and national
under-5 mortality, adult mortality, age-specific mortality, and life
expectancy, 1970–2016: a systematic analysis for the Global
Burden of Disease Study 2016. Lancet. 2017;390(10100):1084–
150.
5. Newman C. Time to address gender discrimination and
inequality in the health workforce. Human Resources for Health,
2014;12(25).
6. Global Strategy on Human Resources for Health: Workforce 2030.
Geneva: World Health Organization; 2016.
7. Liu JX, Goryakin Y, Maeda A, Bruckner T, Scheffler R. Global
health workforce labor market projections for 2030. Human
Resources for Health. 2017;15(11).
8. Cometto G. The WHO Global Strategy on Human Resources
for Health and the UN Commission on Health Employment
and Economic Growth. In: Fourth Global Symposium on
Health Systems Research. Vancouver, Canada: World Health
Organization; 2016.
9. Stenberg K, Hanssen O, Tan-Torres Edejer T, Bertram M, Brindley
C, Meshreky A et al. Financing transformative health systems
towards achievement of the health Sustainable Development
Goals: a model for projected resource needs in 67 low-
income and middle-income countries. Lancet Global Health.
2017;5(9):875–87.
References
10. Working for health and growth: investing in the health workforce.
Report of the High-level Commission on Health Employment and
Economic Growth. Geneva: World Health Organization; 2016.
11. Sustainable Development Goals. United Nations Development
Programme (https://www.undp.org/content/undp/en/home/
sustainable-development-goals.html, accessed 3 March 2019).
12. Five-year action plan for health employment and inclusive
economic growth (2017–2021). Geneva: World Health
Organization; 2018.
13. Standing H. Gender: a missing dimension in human resource
policy and planning for health reforms. Human Resources
Development Journal. 2001;4(1):27–42.
14. Morgan R, George A, Ssali S, Hawkins K, Molyneux S, Theobald
S. How to do (or not to do) … gender analysis in health systems
research. Health Policy and Planning. 2016;31(8):1069–78.
15. Theobald S, Morgan R, Hawkins K, Ssali S, George A, Molyneux S.
The importance of gender analysis in research for health systems
strengthening. Health Policy and Planning. 2017;32(Suppl. 5):v1–
v3.
16. Reskin B. Sex segregation in the workplace. Annual Review of
Sociology. 1993;19:241–70.
17. Anker R, Malkas H, Korten A. Gender-based occupational
segregation in the 1990s. Geneva: International Labour Office;
2003.
18. Gender segregation in education, training and the labour market:
review of the implementation of the Beijing Platform for Action in
the EU Member States. Brussels: European Institute for Gender
Equality; 2017.
19. Gender equality glossary and thesaurus. European Institute for
Gender Equality (https://eige.europa.eu/rdc/thesaurus/browse,
accessed 4 March 2019).
49

20. A factfile on health workforce statistics: gender and health
workforce statistics. Geneva: World Health Organization,
Department of Human Resources for Health; 2008.
21. Occupational segregation. UN Women (http://interactive.
unwomen.org/multimedia/infographic/changingworldofwork/en/
index.html, accessed 4 March 2019).
22. Hegewisch A, Hartmann H. Segregation and the gender wage
gap: a job half done. Washington (DC): Institute for Women’s
Policy Research; 2014 (https://www.dol.gov/wb/resources/
occupational_segregation_and_wage_gap.pdf, accessed 4
March 2019).
23. Gender equality: women make up most of the health sector
workers but they are under-represented in high-skilled jobs.
Paris: Organisation for Economic Co-operation and Development;
2017 (http://www.oecd.org/gender/data/women-make-up-most-
of-the-health-sector-workers-but-they-are-under-represented-in-
high-skilled-jobs.htm, accessed 5 March 2019).
24. Women at work trends. Geneva: International Labour Office;
2016.
25. Gender segregation. Brussels: European Institute for Gender
Equality (https://eige.europa.eu/rdc/thesaurus/terms/1210.
esaurus/terms/1210, accessed 5 March 2019).
26. Women’s rights are human rights. New York: United Nations
Office of the High Commissioner for Human Rights; 2014.
27. Jefferson L, Bloor K, Maynard A. Women in medicine: historical
perspectives and recent trends. British Medical Bulletin.
2015;114:5–15.
28. Razavi S. The political and social economy of care in a
development context: conceptual issues, research questions
and policy options. Gender and Development Programme
Paper Number 3. United Nations Research Institute for Social
Development; 2007.
29. Ferrant G, Pesando LM, Nowacka K. Unpaid care work: the
missing link in the analysis of gender gaps in labour outcomes.
Paris: Organisation for Economic Co-operation and Development;
2014 (https://www.oecd.org/dev/development-gender/Unpaid_
care_work.pdf, accessed 5 March 2019).
30. Global gender gap report. World Economic Forum; 2016.
31. Hegewisch A, Gornick JC. The impact of work-family policies on
women’s employment: a review of research from OECD countries.
Community, Work and Family. 2011;14(2):119–38.
32. Parker C. It’s official: women work nearly an hour longer than
men every day. World Economic Forum; 2017 (https://www.
weforum.org/agenda/2017/06/its-official-women-work-nearly-
an-hour-longer-than-men-every-day/, accessed 5 March 2019).
33. Buchan J, Dhillon IS, Campbell J. Health employment and
economic growth: an evidence base. Geneva: World Health
Organization; 2017.
34. Care work and care jobs for the future of decent work. Geneva:
International Labour Organization; 2018.
35. Newman CJ, Fogarty L, Nthabiseng Makoae L, Reavely E.
Occupational segregation, gender essentialism and male primacy
as major barriers to equity in HIV/AIDS caregiving: findings from
Lesotho. International Journal for Equity in Health. 2011;10:24.
36. Charles M, Grusky DB. Occupational ghettos: the worldwide
segregation of women and men. Stanford University Press; 2004.
37. Men in nursing occupations: American Community Survey
highlight report. United States Census Bureau; 2013.
38. Williams CL. The glass escalator: hidden advantages for men in
the “female” professions. Social Problems. 1992;39(3):253–67.
39. World employment social outlook 2018. Geneva: International
Labour Office; 2018.
40. Women, business and the law. Washington (DC): World Bank;
2018.
41. Burchell B, Rubery J, Smith M, Hardy V. A new method to
understand occupational gender segregation in European labour
markets. Brussels: European Commission, Directorate-General for
Justice; 2015.
42. System-Wide Strategy on Gender Parity. New York: United
Nations; 2017.
A literature review
50

43. Labor force participation rate, female. Washington (DC): World
Bank; 2018 (https://data.worldbank.org/indicator/SL.TLF.CACT.
FE.ZS?end=2017&start=1990&view=chart, accessed 5 March
2019).
44. Jones VA. Why aren’t there more women surgeons? JAMA.
2000;283(5):670.
45. Ramakrishnan A, Sambuco D, Jagsi R. Women’s participation
in the medical profession: insights from experiences in Japan,
Scandinavia, Russia, and Eastern Europe. Journal of Women’s
Health. 2014;23(11).
46. Diringer J, Phipps K, Carsel B. Critical trends affecting the future
of dentistry: assessing the shifting landscape. Report prepared for
American Dental Association; 2013.
47. Russo G, Gonçalves L, Craveiro I, Dussault G. Feminization of the
medical workforce in low-income settings: findings from surveys
in three African capital cities. Human Resources for Health.
2015;13(1):64.
48. Khader Y, Al-Zoubi D, Amarin Z, Alkafagei A, Khasawneh M,
Burgan S et al. Factors affecting medical students in formulating
their specialty preferences in Jordan. BMC Medical Education.
2008;23(8):32.
49. Fukuda Y, Harada T. Gender differences in specialty preference
and mismatch with real needs in Japanese medical students.
BMC Medical Education. 2010;10:15.
50. Buddeberg-Fischer B, Klaghofer R, Abel T, Buddeberg C.
The influence of gender and personality traits on the career
planning of Swiss medical students. Swiss Medical Weekly.
2003;133:535–40.
51. Lambert E, Holmboe E. The relationship between specialty choice
and gender of U.S. medical students, 1990–2003. Academic
Medicine. 2005;80:797–802.
52. Ng-Sueng LF, Vargas-Matos I, Mayta-Tristán P, Pereyra-Elías R,
Montenegro-Idrogo JJ, Inga-Berrospi F et al. Gender associated
with the intention to choose a medical specialty in medical
students: a cross-sectional study in 11 countries in Latin
America. PloS One. 2016;11(8):e0161000.
53. Novielli K, Hojat M, Park PK, Gonnella JS, Veloski JJ. Change of
interest in surgery during medical school: a comparison of men
and women. Academic Medicine. 2001;76(10):S58–61.
54. Chuck E. #MeToo in medicine: women, harassed in hospitals
and operating rooms, await reckoning. NBC News, 20 February
2018 (https://www.nbcnews.com/storyline/sexual-misconduct/
harassed-hospitals-operating-rooms-women-medicine-await-
their-metoo-moment-n846031, accessed 5 March 2019).
55. Boulis A, Jacobs J, Veloski JJ, Gender segregation by specialty
during medical school. Academic Medicine. 2001;76:10.
56. Richardson HC, Redfern N. Why do women reject surgical
careers? Annals of the Royal College of Surgeons of England.
2000;82(9 Suppl.):290–3.
57. Evers A, Sieverding M. Why do highly qualified women (still)
earn less? Gender differences in long-term predictors of career
success. Psychology of Women Quarterly. 2013;38(1):93–106.
58. Tomizawa Y. Gender gap in medicine: only one woman councilor
in the Japan Surgical Society. Tohoku Journal of Experimental
Medicine. 2015;235(2):97–102.
59. Baecher-Lind L. Women in leadership positions within obstetrics
and gynecology: does the past explain the present? Obstetrics
and Gynecology. 2012;120(6):1415–8.
60. Gupta N, Diallo K, Zurn P, Dal Poz MR. Assessing human
resources for health: what can be learned from labour force
surveys? Human Resources for Health. 2003;1(1):5.
61. Hedden L, Barer ML, Cardiff K, McGrail KM, Law MR, Bourgeault
IL. The implications of the feminization of the primary care
physician workforce on service supply: a systematic review.
Human Resources for Health. 2014;12:32.
62. Bettio F, Verashchagina A, and European Commission. Gender
segregation in the labour market: root causes, implications and
policy responses in the EU. European Commission’s Expert Group
on Gender and Employment Issues; 2009.
63. Williams GC, Saizow R, Ross L, Deci EL. Motivation underlying
career choice for internal medicine and surgery. Social Science
and Medicine. 1997;45(11):1705–13.
51

64. Rosenblatt R, Andrilla C. The impact of U.S. medical students’
debt on their choice of primary care careers: an analysis of
data from the 2002 Medical School Graduation Questionnaire.
Academic Medicine. 2005;80(9):815–9.
65. Gjerberg E. Gender similarities in doctors’ preferences – and
gender differences in final specialisation. Social Science and
Medicine. 2002;54:591–605.
66. Heiliger PJ, Hingstman L. Career preferences and the work-
family balance in medicine: gender differences among medical
specialists. Social Science and Medicine. 2000;50:1235–46.
67. Bruce AN, Battista A, Plankey MW, Johnson LB, Marshall
MB. Perceptions of gender-based discrimination during
surgical training and practice. Medical Education Online.
2015;20(1):25923.
68. Diderichsen S, Johansson EE, Verdonk P, Lagro-Janssen T,
Hamberg K. Few gender differences in specialty preferences and
motivational factors: a cross-sectional Swedish study on last-year
medical students. BMC Medical Education. 2013;13(39).
69. Sauers J. Why women really quit breastfeeding. Harper’s Bazaar,
17 July 2018 (https://www.harpersbazaar.com/culture/features/
a21203672/why-women-stop-breastfeeding-pumping-at-work/,
accessed 5 March 2019).
70. England P. Gender inequality in labor markets: the role of
motherhood and segregation. Social Politics. 2005;12(2):264–
88.
71. Harries RL, McGoldrick C, Mohan H, Fitzgerald JEF, Gokani VJ.
Less than full-time training in surgical specialities: consensus
recommendations for flexible training by the Association of
Surgeons in Training. International Journal of Surgery. 2015;23:1.
72. Evans J, Goldacre MJ, Lambert TW. Views of UK medical
graduates about flexible and part-time working in medicine: a
qualitative study. Medical Education. 2000;34:355–62.
73. Eurofound yearbook 2013: living and working in Europe.
Luxembourg: Publications Office of the European Union; 2014.
74. Ek EW, Ek ET, Mackay SD. Undergraduate experience of surgical
teaching and its influence and its influence on career choice. ANZ
J Surg 2005;75:713-8.
75. Peel, J.K., C.M. Schlachta, and N.A. Alkhamesi, A systematic
review of the factors affecting choice of surgery as a career. Can
J Surg, 2018. 61(1): p. 58–67.
76. Evertsson M, England P, Mooi-Reci I, Hermsen J, de Bruijn
J, Cotter D. Is gender inequality greater at lower or higher
educational levels? Common patterns in the Netherlands,
Sweden, and the United States. Social Politics. 2009;16:210–41.
77. Anker R. Theories of occupational segregation by sex: an
overview. International Labour Review. 1997;136:3.
78. Gargiulo DA, Hyman NH, Hebert JC. Women in surgery: do
we really understand the deterrents? Archives of Surgery.
2006;141(4):405–8.
79. Madichie NO. Sex in the kitchen: changing gender roles in
a female-dominated occupation. International Journal of
Entrepreneurship and Small Business. 2013;18(1):90–102.
80. Fitzgerald JE, Tang SW, Ravindra P, Maxwell-Armstrong CA.
Gender-related perceptions of careers in surgery among new
medical graduates: results of a cross-sectional study. American
Journal of Surgery. 2013;206(1):112–9.
81. Tetik S. Talent management: a review of theoretical perspectives
and a guideline for practitioners. Nile Journal of Business and
Economics. 2016;4:40–56.
82. The Global Health 50/50 report: how gender-responsive are the
world’s most influential global health organisations? London:
Global Health 50/50; 2018.
83. Newman CJ, de Vries DH, d’Arc Kanakuze J, Ngendahimana
G. Workplace violence and gender discrimination in Rwanda’s
health workforce: increasing safety and gender equality. Human
Resources for Health. 2011;19(9):19.
84. More women than men enrolled in U.S. medical schools in 2017.
Association of American Medical Colleges News, 18 December
2017 (https://news.aamc.org/press-releases/article/applicant-
enrollment-2017/, accessed 5 March 2019).
85. Correll SJ, Kelly EL, O’Connor LT, Williams JC. Redesigning,
redefining work. Work and Occupations. 2014;41(1):3–17.
A literature review
52

86. Beyond bias and barriers: fulfilling the potential of women
in academic science and engineering. National Academy of
Sciences (US), National Academy of Engineering (US), and
Institute of Medicine (US) Committee on Maximizing the Potential
of Women in Academic Science and Engineering. Washington
(DC): National Academies Press (US); 2007.
87. Goldin C, Katz LF. The cost of workplace flexibility for high-
powered professionals. Annals of the American Academy.
2011;638(1):45–67.
88. Rose S, Hartman H. The long-term gender gap. Challenge.
2004;47(5):30–50.
89. Goldin C, Katz LF. Transitions: career and family life cycles of the
educational elite. American Economic Review. 2008;98(2):363–9.
90. Correll SJ, Benard S, Paik I. Getting a job: is there a motherhood
penalty? American Journal of Sociology. 2007;112:5.
91. Moss-Racusin CA, Dovidio JF, Brescoll VL, Graham MJ,
Handelsman J. Science faculty’s subtle gender biases favor male
students. Proceedings of the National Academy of Sciences.
2012;109(41):16474–9.
92. Williams JC, Phillips KW, Hall EV. Double jeopardy? Gender bias
against women in science. WorkLifeLaw; 2015.
93. Cooper CL, Swanson N. Workplace violence in the health sector:
state of the art (http://www.who.int/violence_injury_prevention/
violence/activities/workplace/WVstateart.pdf, accessed 5 March
2019).
94. Equality at work: the continuing challenge. Global report under
the follow-up to the ILO Declaration on Fundamental Principles
and Rights at Work. International Labour Conference, 100th
session, 2011. Geneva: International Labour Office; 2011.
95. Newman C, Ng C, Pacqué-Margolis S, Frymus D. Integration
of gender-transformative interventions in health professional
education reform for the 21st century: implications of an expert
review. Human Resources for Health. 2016;14:14.
96. Prasad SB, Bhusal KP. Work place sexual harassment among
female health workers in grass-root level health institutions in
Nepal. Occupational Medicine and Health Affairs. 2015;3:4.
97. Channar ZA, Abbassi Z, Ujan IA. Gender discrimination in
workforce and its impact on the employees. Pakistan Journal of
Commerce and Social Sciences. 2011;5(1):177–91.
98. Merkin RS, Shah MK. The impact of sexual harassment on job
satisfaction, turnover intentions, and absenteeism: findings
from Pakistan compared to the United States. SpringerPlus.
2014;3:215.
99. Midwives’ voices, midwives’ realities: findings from a global
consultation on providing quality midwifery care. Geneva: World
Health Organization; 2016.
100. Trix F, Penska C. Exploring the color of glass: letters of
recommendation for female and male medical faculty. Discourse
and Society. 2003;14(2):191–220.
101. Women in Global Health [data unpublished]. 2018.
102. Lundine J, Bourgeault IL, Clark J, Heidari S, Balabanova
D. The gendered system of academic publishing. Lancet.
2018;391:1754–6.
103. Jagsi R, Guancial EA, Worobey CC, Henault LE, Chang Y, Starr R et
al. The “gender gap” in authorship of academic medical literature:
a 35-year perspective. New England Journal of Medicine.
2006;355(3):281–7.
104. Larivière V, Ni C, Gingras Y, Cronin B, Sugimoto CR.
Bibliometrics: global gender disparities in science. Nature.
2013;504(7479):211–3.
105. Jagsi R, Griffith KA, Jones R, Perumalswami CR, Ubel P, Stewart
A. Sexual harassment and discrimination experiences of academic
medical faculty. JAMA. 2016;315(19):2120–1.
106. Isaacs D. Sexual harassment. Journal of Pediatrics and Child
Health. 2018;54:341–2.
107. Mumtaz Z, Salway S, Waseem M, Umer N. Gender-based barriers
to primary health care provision in Pakistan: the experience of
female providers. Health Policy and Planning. 2003;18(3):261–9.
108. Steege R, Taegtmeyer M, McCollum R, Hawkins K, Ormel H, Kok
M et al. How do gender relations affect the working lives of close
to community health service providers? Empirical research, a
review and conceptual framework. Social Science and Medicine.
2018;209:1–13.
53

109. Park M, Cho S-H, Hong H-J. Prevalence and perpetrators of
workplace violence by nursing unit and the relationship between
violence and the perceived work environment. Journal of Nursing
Scholarship. 2015;47(1):87–95.
110. Women’s workplace equality index. Council on Foreign Relations
(https://www.cfr.org/interactive/legal-barriers/, accessed 6 March
2019).
111. Launer J. Sexual harassment of women in medicine: a
problem for men to address. Postgraduate Medical Journal.
2018;94:1108.
112. Fnais N, Soobiah C, Chen MH, Lillie E, Perrier L, Tashkhandi
M et al. Harassment and discrimination in medical training:
a systematic review and meta-analysis. Academic Medicine.
2014;89(5):817–27.
113. National Academies of Sciences, Engineering, and Medicine.
Sexual harassment of women: climate, culture, and
consequences in academic sciences, engineering, and medicine.
Washington (DC): National Academies Press; 2018.
114. Witter S, Namakula J, Wurie H, Chirwa Y, So S, Vong S et al. The
gendered health workforce: mixed methods analysis from four
fragile and post-conflict contexts. Health Policy and Planning.
2017;32(5):v52–v62.
115. Hyde S, Hawkins K. Promoting women’s leadership in the post-
conflict health sector in Cambodia. Building Back Better/Research
in Gender and Ethics: Building stronger health systems (RinGs);
2017.
116. Saifi S, Andone D. Two polio workers killed in attack in Pakistan.
CNN News, 18 March 2018.
117. Harper J. A 24-year-old midwife was taken hostage in March –
and killed this month. NPR, 23 October 2018.
118. Popovich PM, Warren MA. The role of power in sexual
harassment as a counterproductive behavior in organizations.
Human Resource Management Review. 2010;20:45–53.
119. Nielsen MBD, Kjær S, Aldrich PT, Madsen IEH, Friborg MK,
Rugulies R et al. Sexual harassment in care work – dilemmas and
consequences: a qualitative investigation. International Journal of
Nursing Studies. 2017;70:122–30.
120. Lee B-H. #Me Too movement: it is time that we all act
and participate in transformation. Psychiatry Investigation.
2018;15(5):433.
121. Drezner DW. #MeToo and the trouble with new norms.
Washington Post, 14 February 2018.
122. Vagianos A. The “Me Too” campaign was created by a
black woman 10 years ago. Huffington Post, 17 October
2017 (https://www.huffingtonpost.com/entry/the-me-too-
campaign-was-created-by-a-black-woman-10-years-ago_
us_59e61a7fe4b02a215b336fee, accessed 6 March 2019).
123. Thompson K. #MeToo: we stand with the those in the health
workforce who are subjected to sexual harassment in their
workplace. Women in Global Health; 2018 (https://www.
womeningh.org/me-too, accessed 6 March 2019).
124. Spotlight on statistics: gender and health workforce statistics.
Geneva: World Health Organization; 2008.
125. Oelz M, Onley S, Tomei M. Equal pay: an introductory guide.
Geneva: International Labour Office; 2013.
126. Murphy T, Zheng H. What is the definition of gender pay equity?
Cornell University, Industrial and Labor Relations School; 2016.
127. Canada called for a feminist G7: did the G7 deliver? A report card
on the 2018 G7 commitments to gender equality. International
Center for Research on Women; 2018.
128. Langou GD, Sachetti FC, Fuentes ER, de Sanfeliu MB, Drakeman
C, Ochoa P. Achieving “25 by 25”: actions to make women’s
labour inclusion a G20 priority. Consejo Argentino para las
Relaciones Internacionales; 2018.
129. Global wage report 2018/19: what lies behind gender pay gaps.
Geneva: International Labour Office; 2018.
130. Mesch DJ, Rooney PM. Executive compensation and gender:
a longitudinal study of a national nonprofit organization. Paper
presented at ARNOVA, Los Angeles, California, United States of
America, 2004.
131. Lips HM. The gender pay gap: challenging the rationalizations.
Perceived equity, discrimination, and the limits of human capital
models. Sex Roles. 2013;68(3–4):169–185.
A literature review
54

132. Equal pay for work of equal value. UN Women; 2017 (http://www.
unwomen.org/en/news/in-focus/csw61/equal-pay, accessed 6
March 2019).
133. Terada-Hagiwara A, Camingue-Romance SF, Zveglich JE Jr.
Gender pay gap: a macro perspective. ADB Economics Working
Paper Series No. 538. Mandaluyong City, Philippines: Asian
Development Bank; 2018.
134. Chamberlain A. Demystifying the gender pay gap: evidence from
Glassdoor salary data. Glassdoor; 2016.
135. Gender wage gap. Paris: Organisation for Economic Co-
operation and Development; 2017 (https://stats.oecd.org/index.
aspx?queryid=54751, accessed 6 March 2019).
136. Gardner SF, Stowe CD. The impact of a gender shift on a
profession: women in pharmacy. Forum on Public Policy; 2006.
137. Baird M, Daugherty L, Kumar KB, Arifkhanova A. Regional and
gender differences and trends in the anesthesiologist workforce.
Anesthesiology. 2015;123(5):997–1012.
138. Seabury SA, Chandra A, Jena AB. Trends in the earnings of male
and female health care professionals in the United States, 1987
to 2010. JAMA Internal Medicine. 2013;173:1748–50.
139. Anesthesiologist compensation report 2012. Medscape; 2012.
140. Ash AS, Carr PL, Goldstein R, Friedman RH. Compensation and
advancement of women in academic medicine: is there equity?
Annals of Internal Medicine. 2004;141(2):205–12.
141. Kavilanz P. The gender pay gap for women doctors is big – and
getting worse. CNN Business, 14 March 2018 (https://money.
cnn.com/2018/03/14/news/economy/gender-pay-gap-doctors/
index.html, accessed 6 March 2019).
142. Vecchio N, Scuffham PA, Hilton MF, Whiteford HA. Differences
in wage rates for males and females in the health sector: a
consideration of unpaid overtime to decompose the gender wage
gap. Human Resources for Health. 2013;11(9):9–10.
143. Vujicic M, Wall TP, Nasseh K, Munson B. Dentist income levels
slow to recover. Health Policy Institute Research Brief. American
Dental Association; 2013.
144. Budwig M. The fatherhood bonus and the motherhood penalty:
parenthood and the gender gap in pay. Washington (DC): Third
Way NEXT; 2014.
145. Sasser AC. Gender differences in physician pay: tradeoffs
between career and family. Journal of Human Resources.
2005;40(2):477–504.
146. Shih J. Circumventing discrimination: gender and ethnic
strategies in Silicon Valley. Gender and Society. 2006;20(2):177–
206.
147. Lo Sasso AT, Richards MR, Chou CF, Gerber SE. The $16,819 pay
gap for newly trained physicians: the unexplained trend of men
earning more than women. Health Affairs. 2011;30(2):193–201.
148. Fergusson D, Gibb SJ. Sources of the gender wage gap in a New
Zealand birth cohort. Australian Journal of Labour Economics.
12(3):281–98.
149. Watson I. Decomposing the gender pay gap in the Australian
managerial labour market. Australian Journal of Labour
Economics. 2010;13(1):49–79.
150. Blau FD, Kahn LM. The gender wage gap: extent, trends, and
explanations. Journal of Economic Literature. 2017;55(3):789–
865.
151. Figart DM. Gender as more than a dummy variable: feminist
approaches to discrimination. Review of Social Economy.
1997;55(1):1–32.
152. Whitehouse G. Gender and pay equity: future research directions.
Asia Pacific Journal of Human Resources. 2003;41(1):116–28.
153. Bishu SG, Alkadry MG. A systematic review of the gender pay
gap and factors that predict it. Administration and Society.
2017;49(1):65–104.
154. Llorens JJ, Wenger JB, Kellough JE. Choosing public sector
employment: the impact of wages on the representation of
women and minorities in state bureaucracies. Journal of Public
Administration Research and Theory. 2008;18:397–413.
155. Rubery J, Grimshaw D, Figueiredo H. How to close the gender
pay gap in Europe: towards the gender mainstreaming of pay
policy. Industrial Relations Journal. 2005;36(3):184–213.
55

156. The simple truth about the gender pay gap. AAUW (https://www.
aauw.org/research/the-simple-truth-about-the-gender-pay-gap/,
accessed 6 March 2019).
157. Van Der Meer PH. Is the gender wage gap declining in the
Netherlands? Applied Economics. 2008;40(2):149–160.
158. Eastough K, Miller PW. The gender wage gap in paid and
selfemployment in Australia. Australian Economic Papers.
2004;43(3):257–76.
159. Frank L. How the gender pay gap widens as women get
promoted. Harvard Business Review; 2015.
160. Miller PW. The role of gender among low paid and high paid
workers. Australian Economic Review. 2005;38(4):405–17.
161. Blau FD, Kahn LM. The gender pay gap: have women gone
as far as they can? Academy of Management Perspectives.
2007;21(1):7–23.
162. Globally, countries lose $160 trillion in wealth due to earnings
gaps between women and men. Washington (DC): World Bank;
2018.
163. Ravazzini L, Chesters J. Inequality and wealth: comparing
the gender wealth gap in Switzerland and Australia. Feminist
Economics. 2018;24(4):83–107.
164. Cooper M. Reviewed work. Shortchanged: why women have less
wealth and what can be done about it, by Mariko Lin Chang.
American Journal of Sociology. 2012;118(3):816–8.
165. Iyer A, Sen G, George A. The dynamics of gender and class in
access to health care: evidence from rural Karnataka, India.
International Journal of Health Services. 2007;37(3):537–54.
166. Semega JL, Fontenot KR, Kollar MA. Income and poverty in the
United States: 2016. Current Population Reports. Washington
(DC): United States Census Bureau; 2017.
167. Hartmann H, Hayes J, Clark J. How equal pay for working
women would reduce poverty and grow the American economy.
Washington (DC): Institute for Women’s Policy Research; 2014.
168. Raghavan D. How the gender pay gap harms women’s retirement:
lower earnings can lead to smaller nest eggs and social security
checks. NextAvenue; 2014 (https://www.nextavenue.org/how-
gender-pay-gap-harms-womens-retirement/, accessed 6 March
2019).
169. Reed R, Allen M, Castleman T, Coulthard D. “I mean, you want to
be there for them”: young Australian professionals negotiating
careers in a gendered world. Australian Journal of Labour
Economics. 2003;6(4):519–36.
170. Pocock B. The work/life collision: what work is doing to
Australians and what to do about it. Federation Press; 2003.
171. Frohman HA, Nguyen TH, Co F, Rosemurgy AS, Ross SB. The
nonwhite woman surgeon: a rare species. Journal of Surgical
Education. 2015;72(6):1266–71.
172. Fortune 500 CEOs (http://fortune.com/tag/fortune-500-ceos/,
accessed 6 March 2019).
173. Women in national parliaments. Inter-Parliamentary Union (http://
archive.ipu.org/wmn-e/world.htm, accessed 6 March 2019).
174. Our aims for 2020. Nursing Now campaign (https://www.
nursingnow.org/our-aims/, accessed 6 March 2019).
175. Ryan MK, Haslam SA, Morgenroth T, Rink F, Stoker J, Peters K.
Getting on top of the glass cliff: reviewing a decade of evidence,
explanations, and impact. Leadership Quarterly. 2016;27:446–
55.
176. Moyer CA, Abedini NC, Youngblood J, Talib Z, Jayaraman
T, Manzoor M et al. Advancing women leaders in global health:
getting to solutions. Annals of Global Health. 2018;84(4):743–52.
177. Manzoor M. Percentage of WHO Member States’ ministries
of health that are headed by women. Women in Global Health
[unpublished data].
178. Dhatt R, Theobald S, Buzuzi S, Ros B, Vong S, Muraya K et al. The
role of women’s leadership and gender equity in leadership and
health system strengthening. Global Health, Epidemiology and
Genomics. 2017;2:e8.
A literature review
56

179. Toledo P, Duce L, Adams J, Ross VH, Thompson KM, Wong CA.
Diversity in the American Society of Anesthesiologists leadership.
Anesthesia and Analgesia. 2017;124(5):1611–6.
180. WFSA Gender Balance working group (WFSA/GB-wg). WFSA In
The Road To Gender Equality In Anaesthesiology. 2017.
181. Downs JA, Reif LK, Hokororo A, Fitzgerald DW. Increasing
women in leadership in global health. Academic Medicine.
2014;89(8):1103–7.
182. Newman C, Kimeu A, Shamblin L, Penders C, McQuide PA, Bwonya
J. Making non-discrimination and equal opportunity a reality in
Kenya’s health provider education system: results of a gender
analysis. World Health and Population. 2011;13(2):23–33.
183. The power of parity: how advancing women’s equality can add
$12 trillion to global growth. McKinsey Global Institute; 2015.
184. Eagly A, Johannesen-Schmidt MC. The leadership styles of
women and men. Journal of Social Issues. 2001;57(4):781–97.
185. Triple impact: how developing nursing will improve health,
promote gender equality and support economic growth. London,
United Kingdom: All-Party Parliamentary Group on Global Health;
2016.
186. Eagly A, Carli LL. Women and the labyrinth of leadership. Harvard
Business Review; 2007.
187. Borg S. Interview with Sania Nishtar, President, Heartfile,
and short-listed nominee for Director-General, World Health
Organization. Women in Global Health; 2017.
188. Larson E, George A, Morgan R, Poteat T. 10 Best resources on
… intersectionality with an emphasis on low- and middle-income
countries. Health Policy and Planning. 2016;31(8):964–9.
189. Hankivsky O, Intersectionality 101. Institute for Intersectionality
Research and Policy, SFU; 2014.
190. Newman C, Chama PK, Mugisha M, Matsiko CW, Oketcho V.
Reasons behind current gender imbalances in senior global
health roles and the practice and policy changes that can
catalyze organizational change. Global Health, Epidemiology and
Genomics. 2017;2: e19.
191. Allen I. Women doctors and their careers: what now? BMJ.
2005;331:569–72.
192. Hyde S, Buzuzi S. How gender roles and relations affect health
workers’ training opportunities and career progression in post-
crisis rural Zimbabwe. Building Back Better/Research in gender
and ethics: building stronger health systems (RinGs).
193. Najafizada SAM, Bourgeault IL, Labonté R. A gender analysis of
a national community health workers program: a case study of
Afghanistan. Global Public Health. 2019;14(1):23–36.
194. Modra LJ, Yong SA, Austin DE. Women in leadership in intensive
care medicine. ICU Management & Practice. 2016;16(3).
195. Medew J. Surgeon Caroline Tan breaks silence over sexual
harassment in hospitals. The Age; 2015 (https://www.theage.
com.au/national/victoria/surgeon-caroline-tan-breaks-silence-
over-sexual-harassment-in-hospitals-20150311-141hfi.html,
accessed 7 March 2019).
196. HRH 2030 Consortium. Motivation and retention of health
workers in Ministry of Health facilities in four governorates in
Jordan: findings from a mixed methods study. HRH 2030: Human
Resources for Health in 2030. USAID; 2016.
197. Morgan R, Dhatt R, Muraya K, Buse K, George AS. Recognition
matters: only one in ten awards given to women. Lancet.
2017;389:2469.
198. Morgan R, Ayiasi RM, Barman D, Buzuzi S, Ssemugabo C, Ezumah
N et al. Gendered health systems: evidence from low- and
middle-income countries. Health Research Policy and Systems.
2018;16(1):58.
199. Mumtaz Z, Salway S, Nykiforuk C, Bhatti A, Ataullahjan A,
Ayyalasomayajula B. The role of social geography on lady health
workers’ mobility and effectiveness in Pakistan. Social Science
and Medicine. 2013;91:48–57.
200. Rao A, Miller C, Kelleher D, Sandler J. Gender at work: theory and
practice for 21st century organizations. Routlege Taylor & Francis
Group; 2015.
201. Decent work. International Labour Organization (https://www.ilo.
org/global/topics/decent-work/lang--en/index.htm, accessed 7
March 2019).
57

202. Adams TL. Gender and feminization in health care professions.
Sociology Compass. 2010;4(7):454–65.
203. Gender equality glossary. UN Women (https://
trainingcentre.unwomen.org/mod/glossary/view.
php?id=36&mode=letter&hook=G&sortkey=&sortorder=,
accessed 7 March 2019).
204. Newman C. Gender equality in human resources for health: what
does this mean and what can we do? Chapel Hill, NC: IntraHealth
International; 2010.
205. Gender mainstreaming for health managers: a practical approach.
Geneva: World Health Organization; 2011.
206. Gender integration continuum. Interagency Gender Working
Group (https://www.igwg.org/wp-content/uploads/2017/05/
FG_GendrIntegrContinuum.pdf, accessed 7 March 2019).
207. Monitoring the building blocks of health systems: a handbook
of indicators and their measurement strategies. Geneva: World
Health Organization; 2010.
208. Richards C, Bouman WP, Seal L, Barker MJ, Nieder TO, T’Sjoen
G. Non-binary or genderqueer genders. International Review of
Psychiatry. 2016;28(1):95–102.
209. What is sexual harassment? Equal Employment Opportunity
Commission (http://www.un.org/womenwatch/osagi/pdf/
whatissh.pdf, accessed 7 March 2019).
210. Kanter RM. Men and women of the corporation. New York: Basic
Books; 1977.
211. Liu WM. How Trump’s “toxic masculinity” is bad for other men.
Time, 14 April 2016 (http://time.com/4273865/donald-trump-
toxic-masculinity/, accessed 7 March 2019).
212. Fisseha S, Hildebrand M. Toxic masculinity: a poor excuse for
poor global health. BMJ Global Health Blog; 2018.
213. Wedgwood N. Connell’s theory of masculinity: its origins and
influences on the study of gender. Journal of Gender Studies.
2009;18(4):329–39.
214. Beijing Declaration and Platform for Action. Fourth World
Conference on Women: Action for Equality, Development and
Peace, Beijing, China, 1995.
A literature review
58

Co-Chairs:
Women in Global Health
World Health Organization
Organizational members:
Canadian Institute for Health Information
Canadian Health Human Resources Network
Chemonics/HRH2030
DAI Global, LLC
The George Institute for Global Health
Global Association of Student and Novice Nurses (GASNN)
Frontline Health Workers’ Coalition (FHWC)
International Pharmaceutical Federation (FIP)
International Federation of Medical Students’ Associations (IFMSA)
IntraHealth International
Jhpiego
The Net Community
Public Services International (PSI)
Research in Gender Ethics (RinGs)
Save the Children
Wemos
Women Deliver
Annex 1. Membership of the Gender Equity Hub in
the Global Health Workforce Network
59

SR# Submission
Lessons Learned
Policy/Implications (how will the study/initiative
findings or outcomes be used in the
Limitations
Strengths
Key Results/Findings
Methods of Analysis
Input Variable(s)
Output Variable
Research Design
A) Qualitative
B) Quantitative
C) Mixed Methods
Interventions
Study Participants
A) Students in education and training
B) Graduations and early
Context
Reasearch/Program Objectives
Research Area
A) Leadership
B) Gender
C) Decent work/harassment/violence
Study Title
Year Published
2. Co-authors
1. Lead author
Type of submission
Insert your name as a reviwer
Annex 2. Literature matrix
GENDER EQULTY EVIDENCE MAPPING EXTRACTION TOOL
A literature review
60

Health Workforce Department
World Health Organization
20 Avenue Appia
CH1211 Geneva 27 Switzerland
www.who.int/hrh
ISBN 978-92-4-151546-7
