
Page 1 of 43
Technical Annex
(version dated 26 December 2022)
Updated Appendix 3 of the
WHO Global NCD Action Plan 2013-2030
What is appendix 3
The global action plan for the prevention and control of noncommunicable diseases 2013-2020
1
was
endorsed by the Sixty-sixth World Health Assembly
2
in 2013 with an Appendix containing a menu of policy
options and cost-effective interventions for prevention and control of major noncommunicable diseases
(known as “Appendix 3”). The purpose of Appendix 3 is to support Member States in implementing, as
appropriate for national context (without prejudice to the sovereign rights of nations to determine taxation
among other policies), actions to achieve the nine voluntary global targets for NCD prevention and control
through the six objectives of the WHO global NCD action plan 2013‒2030. The first update of Appendix 3
in 2017, endorsed by the Seventieth World Health Assembly,
3
contained very cost-effective and affordable
interventions, as well as other cost-effective interventions for the prevention and control of NCDs. The list
of interventions contained in Appendix 3 is not exhaustive but is intended to provide information and
guidance on cost-effectiveness of population-based and individual interventions based on current evidence.
It also aims to act as the basis for future work to develop and expand the evidence base, taking into
consideration overarching/enabling policy actions as well as non-financial considerations.
The current updates to Appendix 3, formulated in response to decisions WHA72(11) (2019) and WHA75(11)
(2022), complement existing global strategies and action plans and several new technical products that
support the implementation road map 2023‒-2030 for the global action plan for the prevention and control
of noncommunicable diseases 2013‒2030,
4
including the WHO menu of cost-effectiveness interventions
for mental health,
5
the recommended interventions to address the health impact of air pollution
6,7
and the
menu of cost-effective interventions for oral health.
8
1
WHO. Global Action Plan for the Prevention and Control of NCDs 2013-2020/ Geneva: World Health Organization; 2013.
(https://www.who.int/publications/i/item/9789241506236)
2
See document WHA66/2013/REC/1, resolution WHA66.10.
3
See document WHA70/2017/REC/1, resolution WHA70.11.
4
Document A75/10 Add.8; noted by the Health Assembly, see also document WHA75/REC/3, summary records of first meeting,
section 3, fifth meeting, section 2, and sixth meeting of Committee A.
5
WHO. WHO menu of cost-effective interventions for mental health. Geneva: World Health Organization; 2021
(https://apps.who.int/iris/handle/10665/343074, accessed 1 December 2022).
6
WHO. Compendium of WHO and other UN guidance on health and the environment, 2022 update. Geneva: World Health
Organization; 2022 (https://apps.who.int/iris/handle/10665/352844, accessed 1 December 2022).
7
WHO. WHO global air quality guidelines: particulate matter (PM2.5 and PM10), ozone, nitrogen dioxide, sulfur dioxide and carbon
monoxide. Geneva: World Health Organization; 2021 (https://apps.who.int/iris/handle/10665/345329, accessed 1 December 2022)
8
See document WHA74/2021/REC/1, resolution WHA74.5.

Page 2 of 43
Why update appendix 3
The Appendix 3 has been updated in order to accelerate progress towards meeting the nine voluntary
global NCD targets and Sustainable Development Goal 3 target 3.4 and to support the implementation road
map 2023‒2030 with its new acceleration plan to support Member States in implementing the
recommendations for the prevention and management of obesity over the life course , by:
(a) considering interventions from new WHO normative and standard-setting products since the adoption
of the WHO global NCD action plan 2013‒2020;
(b) refining the existing formulation of some interventions based on lessons learned from the use of the
previous two versions and reflecting WHO’s new guidance;
(c) updating and adding interventions on the basis of agreed criteria and new and available scientific
evidence of impact.
The area of Appendix 3 where this is most relevant is under Objective 3 (risk factors) and Objective 4
(health systems). All of the “very cost-effective and affordable interventions for all Member States”
interventions in the original Appendices were listed under Objectives 3 and 4, and this remains the case in
the updated version.
What has changed?
There has been no change to the menu of options listed for Objectives 1 (raising the priority of prevention
and control of NCDs), 2 (strengthening leadership and governance), 5 (promote research and development)
and 6 (monitoring and evaluation) which are process-related recommendations. The Appendix 3 is related
to Objective 3 (risk factors) and 4 (health systems).
Within Objectives 3 and 4, in the 2017 appendix there were 16 interventions considered with a cost-
effectiveness ratio ≤I$100 per DALY averted
9
in low -and middle-income countries (referred to as the “best
buys”) and 20 interventions with a cost-effectiveness ratio >I$100/DALY (previously referred to as “good
buys”). In addition, 36 interventions without CEA but are part of WHO guidance were also provided. In the
2022 updated Appendix 3, there are now a total of 90 interventions and 22 overarching/enabling actions,
representing an expansion from the original list of 88 interventions (including overarching/enabling actions)
(Table 1). In the current update, the cost-effectiveness was examined for 58 interventions out of the 90
interventions using WHO’s Choosing interventions that are cost-effective (WHO-CHOICE) methodology
10
,
which was also used in 2017. The increase in the number of interventions between the 2017 and 2022
updates is due to the availability of new scientific evidence or WHO recommendations as proposed by as
proposed by the Secretariat’s technical units and/or expert groups linked to the global NCD action plan.
9
The international dollar is a hypothetical unit of currency that has the same purchasing power parity that the U.S. dollar had in the
United States at a given point in time.
10
https://www.who.int/teams/health-systems-governance-and-financing/economic-analysis/health-technology-assessment-and-
benefit-package-design/generalized-cost-effectiveness-analysis

Page 3 of 43
Out of the 58 interventions, 28 are considered to be the most cost-effective and feasible for
implementation
11
. In addition, 32 interventions that are part of WHO’s guidance were also included but
without WHO-CHOICE analysis. The absence of cost-effectiveness does not mean that the intervention is
not cost-effective, affordable or feasible but that the WHO-CHOICE analysis could not be completed in the
2022 update due to methodological or capacity reasons.
Table 1: Overarching/enabling actions and interventions included in the 2022 update of Appendix 3
Interventions
Overarching/enabling
actions
Interventions with
WHO-CHOICE
analysis
Interventions
without WHO-
CHOICE analysis
Objective 3
Tobacco 3 7 2
Harmful use of alcohol 4 5 6
Unhealthy diet 2 7 4
Physical inactivity 5 2 5
Objective 4
Cardio-vascular diseases
8
13 7
Diabetes 6 2
Chronic respiratory diseases 4 4
Cancer 14 2
Total 22 58 32
How to use this information
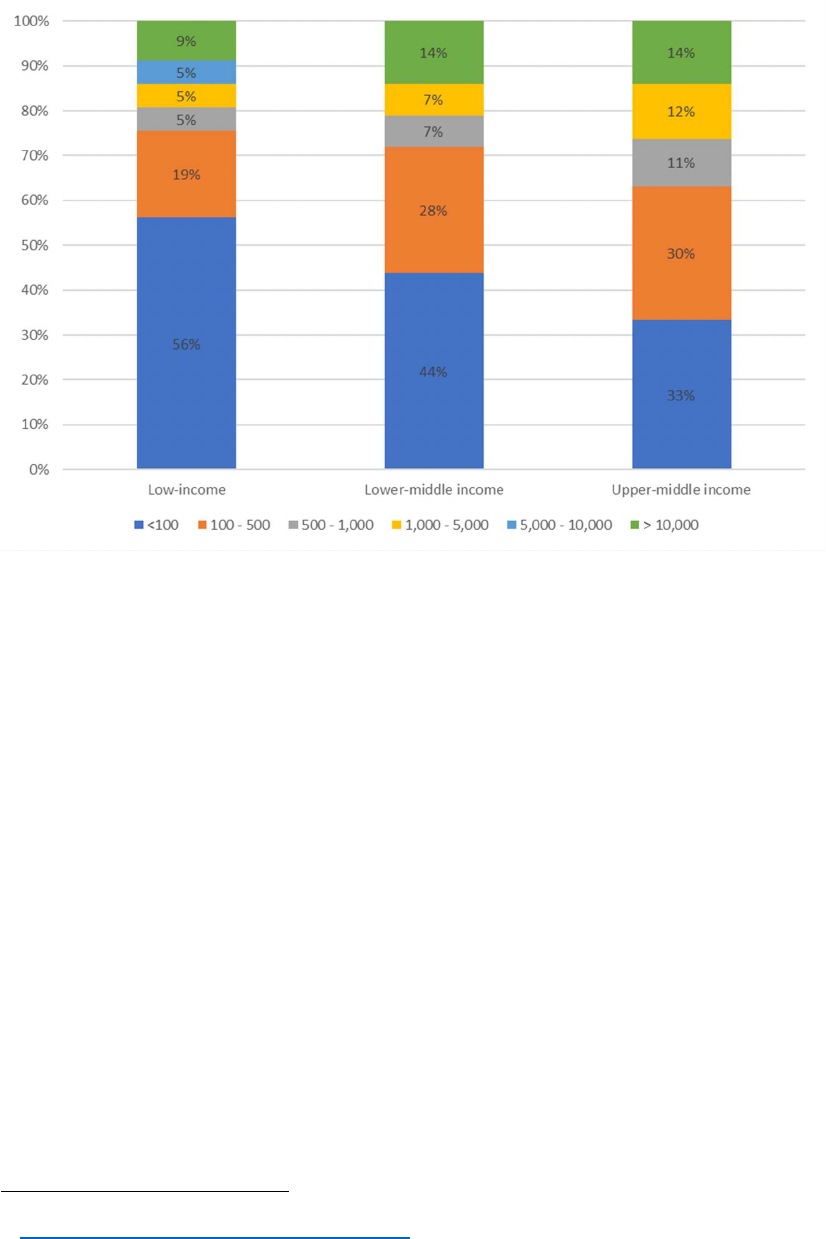
Figure 1 presents the percentage of interventions for which we conducted WHO-CHOICE analysis falling
within each band of cost-effectiveness ratio for low-income, lower-middle income and upper-middle income
countries. The cost-effectiveness threshold represents the maximum amount one is willing to pay per heath
outcome. The threshold is generally used to identify interventions that represent good value for money and
will be different depending on the national context. The figure shows that with a threshold of <I$100 per
healthy life year gained 56%, 44% and 33% of the interventions are considered very good value-for-money
in low-income, lower-middle income and upper-middle income countries respectively. As this threshold
increases, the proportion of interventions considered good value-for-money increases too. if the national
cost-effectiveness threshold chosen by a low-income country is Int$ 1000 per healthy life year gained, then
82% of the proposed 58 interventions in the 2022 update would represent good value for money in that
country.
11
With an average cost-effectiveness ratio of ≤I$ 100 per healthy life year gained in low and lower-middle income countries. The
international dollar is a hypothetical unit of currency that has the same purchasing power parity that the U.S. dollar had in the
United States at a given point in time.
Page 4 of 43
Figure 1: Percentage of interventions by cost-effectiveness band for the 3 income groups
The importance of non-economic considerations
The economic analyses give an assessment of cost-effectiveness, based on the health impact and the
economic cost of the intervention. Although the results provide a set of parameters for consideration by
Member States, however it must be emphasised that such global analyses should be accompanied by
analyses further tailored to the local context. The OneHealth Tool is available to help individual countries
to cost specific interventions in their national context. The Secretariat will also consider the development of
an interactive web-based tool for countries to visualize the impact on national NCD targets of prioritizing
and scaling up the implementation of a set of cost-effective interventions of the updated Appendix 3 as part
of the implementation roadmap for NCDs.
When considering interventions for prevention and management of any disease or condition, including
noncommunicable diseases, emphasis should be given to both economic and non-economic criteria, as
both will affect the implementation and impact of interventions. Non-economic aspects such as
acceptability, feasibility or health system capacity, sustainability, scalability, equity, and ethics
12
are
essential to consider as part of the prioritization and implementation of the proposed interventions, based
on the specific context of a country. Non-economic considerations that may affect the feasibility of certain
interventions in some settings have been included as a separate column in the tables on pages 7 to 24.
12
WHO. Principles of health benefit packages. Geneva: World Health Organization; 2021
(https://www.who.int/publications/i/item/9789240020689)
Page 5 of 43
Methodological annex
A methodological annex can be found at the end of this document. This annex provides more detailed
information about the methodology used to identify and analyse interventions, and includes the
assumptions used in the WHO-CHOICE economic modelling. The methodological Annex also contains
more detailed economic analyses for each intervention, with summary tables of costs, health impacts and
cost-effectiveness ratios in bands for all interventions. Table 2 presents the list of interventions for each of
the four risk factors and disease areas for three income categories of countries: low-income countries,
lower-middle income countries and upper-middle-income countries. Table 3 ranks all interventions for low
and lower-middle income countries by risk factor and disease area, with interventions with an average cost-
effectiveness ratio ≤ I$100 per health life year gained (HLYg) considered to be the most cost-effective and
feasible for implementation in all countries, i.e. the “Best Buys”. Interventions with an average cost-
effectiveness ratio > I$ 100 are listed next and may be considered depending on the country context.

Page 6 of 43
Objective 1: To raise the priority accorded to the prevention and control of
noncommunicable diseases in global, regional and national agendas and internationally
agreed development goals, through strengthened international cooperation and
advocacy
Overarching/enabling actions
Raise public and political awareness, understanding and practice about prevention and control of
NCDs
Integrate NCDs into the social and development agenda and poverty alleviation strategies
Strengthen international cooperation for resource mobilization, capacity-building, health workforce
training and exchange of information on lessons learnt and best practices
Engage and mobilize civil society and the private sector as appropriate and strengthen international
cooperation to support implementation of the action plan at global, regional and national levels
Im
plement other policy options in objective 1
Objective 2: To strengthen national capacity, leadership, governance, multisectoral
action and partnerships to accelerate country response for the prevention and control of
noncommunicable diseases
Overarching/enabling actions
Prioritize and increase, as needed, budgetary allocations for prevention and control of NCDs
without prejudice to the sovereign right of nations to determine taxation and other policies
Assess national capacity for prevention and control of NCDs
Develop and implement a national multisectoral policy and plan for the prevention of control of
NCDs through multi-stakeholder engagement
Implement other policy options in objective 2 to strengthen national capacity including human and
institutional capacity, leadership, governance, multisectoral action and partnerships for prevention
and control of noncommunicable diseases

Page 7 of 43
Objective 3: To reduce modifiable risk factors for noncommunicable diseases and
underlying social determinants through creation of health-promoting environments
Tobacco use
Overarching/enabling actions
For the Parties to the WHO Framework Convention on Tobacco Control (WHO FCTC):
Strengthen the effective implementation of the WHO FCTC and its guidelines for implementation,
as well as the Protocol to Eliminate Illicit Trade in Tobacco Products, if applicable
Establish and operationalize national coordinating mechanisms for the implementation of the WHO
FCTC as part of a national tobacco control strategy with specific mandates, responsibilities and
resources
For the Member States that are not Parties to the WHO FCTC:
Consider implementing the measures set out in the WHO FCTC and its guidelines for
implementation, as well as the Protocol to Eliminate Illicit Trade in Tobacco Products, if applicable,
as the foundational instruments in global tobacco control
Specific interventions with WHO-CHOICE analysis
N° Intervention Non-economic
considerations
WHO tools
T1 Increase excise taxes and prices on
tobacco products
The WHO FCTC, its guidelines
and its Protocol to Eliminate
Illicit Trade in Tobacco Products
MPOWER policy measures
WHO reports on the global
tobacco epidemic (2011, 2013,
2015, 2019)
WHO technical manual on
tobacco tax policy and
administration (2021)
IARC handbook on
effectiveness of tax and price
policies for tobacco control
(2011)
Plain packaging of tobacco
products: evidence, design and
implementation (2016)
T2 Implement large graphic health
warnings on all tobacco packages,
accompanied by plain/standardized
packaging
Requires capacity
for implementing
and enforcing
regulations and
legislation
T3 Enact and enforce comprehensive
bans on tobacco advertising,
promotion and sponsorship
T4 Eliminate exposure to second-hand
tobacco smoke in all indoor
workplaces, public places and public
transport
T5 Implement effective mass media
campaigns that educate the public
about the harms of smoking/tobacco
use and second hand smoke, and
encourage behaviour change
T6 Provision of cost-covered effective
population-wide support (including
Requires trained
providers in

Page 8 of 43
brief advice, national toll-free quit line
services and mCessation) for tobacco
cessation to all tobacco users.
sufficient numbers
and an effective
health system
T7 Provision of cost-covered effective
pharmacological interventions to all
tobacco users who want to quit,
through the use of nicotine
replacement therapy (NRT), Bupropion
and Varenicline.
Other interventions from WHO guidance (without WHO-CHOICE analysis)
N° Intervention
T8 Establish a tracking and tracing system to support the
elimination of illicit trade in tobacco products that is in line
with Article 8 of the Protocol to Eliminate Illicit Trade in
Tobacco Products
T9 Ban cross-border tobacco advertising, promotion and
sponsorship, including those through modern means of
communication

Page 9 of 43
Harmful use of alcohol
Overarching/enabling actions
Implement applicable recommendations in the WHO Global strategy to reduce harmful use of
alcohol through multisectoral actions in the recommended target areas
13
Implement WHO’s global action plan on alcohol 2022-2030 to support and complement policy
measures and interventions implemented at the national level in accordance with the 10 areas
recommended in the global strategy
14
Strengthen leadership and increase commitment and capacity to address the harmful use of
alcohol
Increase awareness and strengthen the knowledge base on the magnitude and nature of problems
caused by harmful use of alcohol by awareness programmes, operational research, improved
monitoring and surveillance systems
Specific interventions with WHO-CHOICE analysis
N° Intervention Non-economic
considerations
WHO tools
A1
Increase excise taxes on alcoholic beverages Levying taxes should
be combined with other
price measures, such
as bans on discounts
or promotions
The SAFER Technical
package (2019)
Resource book on
alcohol taxation (2017)
Manual on alcohol
taxation (in press)
Reducing the harm
from alcohol – by
regulating cross-border
alcohol marketing,
advertising and
promotion: a technical
report (2022)
Save lives: a road
safety technical
package (2017)
The WHO ASSIST
package for hazardous
and harmful substance
use (2010)
A2
Enact and enforce bans or comprehensive
restrictions on exposure to alcohol advertising
(across multiple types of media)
Requires capacity and
infrastructure for
implementing and
enforcing regulations
and legislation
A3
Enact and enforce restrictions on the physical
availability of retailed alcohol (via reduced
hours of sale)
A4
Enact and enforce drink-driving laws and
blood alcohol concentration limits via sobriety
checkpoints
A5
Provide brief psychosocial intervention for
persons with hazardous and harmful alcohol
use
Requires trained
providers at all levels
of health care
13
WHO. Global strategy to reduce the harmful use of alcohol; 2010
(http://www.who.int/substance_abuse/publications/global_strategy_reduce_harmful_use_alcohol/en/)
14
WHO. Political declaration of the third high-level meeting of the General Assembly on the prevention and control of non-
communicable diseases. Appendix: Draft action plan (2022-2030) to effectively implement the global strategy to reduce the
harmful use of alcohol as a public health priority. Document EB 150/7 add. 1; 2022
(https://apps.who.int/gb/ebwha/pdf_files/EB150/B150_7Add1-en.pdf)

Page 10 of 43
Brief intervention for
hazardous and harmful
drinking: a manual for
use in primary care
(2001)
mhGAP intervention
guide 2.0 (2016)
Other interventions from WHO guidance (without WHO-CHOICE analysis)
N°
Intervention
A6 Carry out regular reviews of prices in relation to level of inflation and
income
A7 Establish minimum prices for alcohol where applicable
A8 Enact and enforce an appropriate minimum age for purchase or
consumption of alcoholic beverages and reduce density of retail outlets
A9 Restrict or ban promotions of alcoholic beverages in connection with
sponsorships and activities targeting young people
A10
Provide prevention, treatment and care for alcohol use disorders and
comorbid conditions in health and social services
A11
Provide consumers with information, including labels and health
warnings, about content of alcoholic beverages and the harms
associated with alcohol consumption

Page 11 of 43
Unhealthy diet
Overarching/enabling actions
Implement WHO’s Global Strategy on Diet, Physical Activity and Health
15
, the Global strategy for
infant and young child feeding jointly developed by WHO and UNICEF
16
and the WHO
Comprehensive implementation plan on maternal, infant and young child nutrition
17
Develop and implement national nutrient- and food-based dietary guidelines, as well as nutrient
profile models
18
for different applications as appropriate
Specific interventions with WHO-CHOICE analysis
N° Intervention Non-economic
considerations
WHO tools
H1
Reformulation policies for healthier
food and beverage products (e.g.
elimination of trans-fatty acids and/or
reduction of saturated fats, free
sugars and/or sodium)
Requires multisectoral
actions with relevant
ministries and support
by civil society.
Regulatory capacity
along with
multisectoral action is
needed.
Reformulation (H1)
WHO policy brief on
reformulation of food and
beverage products (2022)
WHO global sodium
benchmarks for different food
categories (2021)
REPLACE technical document
on eliminating industrially-
produced trans fat from the
global food supply (2021)
TFA and sodium country score
cards (2012)
Front-of-pack labelling (H2)
Policy brief on nutrition
labelling (2022)
Codex Alimentarius standards
and guidelines on food
labelling (2007)
Guiding principles and
framework manual for front-of-
H2
Front-of-pack labelling as part of
comprehensive nutrition labelling
policies for facilitating consumers’
understanding and choice of food for
healthy diets
H3
Public food procurement and service
policies for healthy diets (e.g. to
reduce the intake of free sugars,
sodium, unhealthy fats, and to
increase the consumption of
legumes, wholegrains, fruits and
vegetables)
H4
Behaviour change communication
and mass media campaign for
healthy diets (e.g. to reduce the
intake of energy, free sugars,
sodium, unhealthy fats, and to
increase the consumption of
legumes, wholegrains, fruits and
vegetables)
15
WHO. Global strategy on diet, physical activity and health; 2004 (https://www.who.int/publications/i/item/9241592222)
16
WHO/UNICEF. Global strategy for infant and young child feeding; 2003 (https://www.who.int/publications/i/item/9241562218)
17
WHO. Comprehensive implementation plan on maternal, infant and young child nutrition; 2014
(https://www.who.int/publications/i/item/WHO-NMH-NHD-14.1)
18
WHO. Nutrient profile model. Copenhagen: World Health Organization Regional Office for Europe; 2015
(https://www.euro.who.int/data/assets/pdf_file/0005/270716/Nutrient-children_web-new.pdf)

Page 12 of 43
H5
Policies to protect children from the
harmful impact of food marketing on
diet
pack labelling for promoting
healthy diet (2019)
Handbook on food labelling to
protect consumers (2016)
Implementing nutrition
labelling policies: a review of
contextual factors (2021)
Front-of-package labelling as
a policy tool for the prevention
of NCDs in the Americas
(2021)
Health evidence network
support synthesis report on
effectiveness of FOPL policies
in the WHO European region
(2018)
Guideline in nutrition labelling
policies (forthcoming)
Public food procurement and
service policies (H3)
Action framework for
developing and implementing
public food procurement and
service policies for a healthy
diet (2021)
Implementing school food and
nutrition policies: a review of
contextual factors (2021)
Guideline school food and
nutrition policies (forthcoming)
Behaviour change (H4)
SHAKE the salt habit:
technical package for salt
reduction (2016)
Marketing restrictions (H5)
Protecting children from the
harmful impact of food
marketing: policy brief (2022)
Set of recommendations on
the marketing of foods and
non-alcoholic beverages to
children (2010)
Marketing of food and non-
alcoholic beverages to
children (2010)
Framework for implementing
the set of recommendations
H6
Protection, promotion and support of
optimal breastfeeding practices
H7
Taxation on sugar-sweetened
beverages as part of comprehensive
fiscal policies to promote healthy
diets

Page 13 of 43
on the marketing of foods and
non-alcoholic beverages to
children (2012)
Tackling food marketing to
children in a digital world:
trans-disciplinary perspectives
(2021)
Regional action framework on
protecting children from the
harmful impact of food
marketing in WPRO (2020)
WHO guideline on policies to
protect children from the
harmful impact of food
marketing (forthcoming)
Breastfeeding practices (H6)
WHO website on
breastfeeding
Fact sheet on infant and
young child feeding
Implementation manual on
ending the inappropriate
promotion of foods for infants
and young children (2017)
NetCode toolkit for ongoing
monitoring and periodic
assessment of the Code
(2017)
Ten steps to successful
breastfeeding
Guideline on counselling of
women to improve
breastfeeding practices (2018)
Implementation guidance on
counselling women to improve
breastfeeding practices (2021)
Advocacy guidance brief on
enacting paid family leave and
workplace breastfeeding
policies (2019)
Advocacy brief on
breastfeeding and family-
friendly policies (2019)
Advocacy brief on increasing
funding for breastfeeding
(2019)

Page 14 of 43
SSB taxation (H7)
Policy brief on fiscal policies to
promote healthy diets (2022)
WHO manual on sugar-
sweetened beverage taxation
policies to promote healthy
diets (2022)
Implementing fiscal and
pricing policies to promote
healthy diets: a review of
contextual factors (2021)
Fiscal policies for diet and the
prevention of NCDs (2016)
Global database on the
Implementation of Nutrition
Action (GINA): SSB taxation
Sugar-sweetened beverage
taxation in the region of the
Americas (2020)
SSB taxes in the WHO
European region: success
through lessons learned and
challenges faced (2022)
Guideline on fiscal policies to
promote healthy diets
(forthcoming)
Other interventions from WHO guidance (without WHO-CHOICE analysis)
N°
Intervention
H8 Subsidies on healthy foods and beverages (e.g. fruits and vegetables) as part of fiscal policies
for healthy diets
H9 Menu labelling in food service for healthy diets (e.g. to reduce the intake of energy, free sugars,
sodium and/or unhealthy fats)
H10
Limiting portion and package size for healthy diet (e.g. to reduce the intake of energy, free
sugars, sodium and/or unhealthy fats)
H11
Nutrition education and counselling for healthy diets in different settings (e.g. in preschools,
schools, workplaces and hospitals)

Page 15 of 43
Physical inactivity
Overarching/enabling actions
WHO’s global action plan on physical activity 2018–2030: more active people for a healthier
world
19
ACTIVE: a technical package for increasing physical activity
20
WHO guidelines on physical activity and sedentary behaviour
21
Leadership and whole of government commitment to address physical inactivity using a life course
approach
22
Strong advocacy to increase awareness and knowledge on the cross cutting benefits of increasing
physical activity, operational research and knowledge translation and improved monitoring and
surveillance systems
23
Specific interventions with WHO-CHOICE analysis
N° Intervention Non-economic
considerations
WHO tools
P1
Provide physical activity
assessment, counselling, and
behaviour change support as part of
routine primary health care services
through the use of a brief
intervention
Requires sufficient
capacity, and staff with
sufficient training in
primary care
Global action plan on
physical activity 2018–2030:
more active people for a
healthier world (2018)
Promoting physical activity
through primary health care:
a toolkit (2021)
P2
Implement sustained, population
wide, best practice communication
campaigns to promote physical
activity, with links to community-
based programmes and
environmental improvements to
enable and support behaviour
change.
Requires multisectoral
actions with relevant
ministries and support by
civil society
Other interventions from WHO guidance (without WHO-CHOICE analysis)
N°
Intervention
P3 Implement urban and transport planning and urban design, at all
levels of government, to provide compact neighbourhoods
providing mixed-land use and connected networks for walking
19
WHO. Global Action Plan on Physical activity 2018-2030: More active people for a healthier world; 2018
https://apps.who.int/iris/bitstream/handle/10665/272722/9789241514187-eng.pdf)
20
WHO. ACTIVE: a technical package for increasing physical activity; 2018 (https://apps.who.int/iris/handle/10665/275415)
21
WHO. WHO guidelines on physical activity and sedentary behaviour; 2020
(https://www.who.int/publications/i/item/9789240015128)
22
WHO. Fair play: building a strong physical activity system for more active people; 2021
(https://apps.who.int/iris/handle/10665/346169)
23
WHO. Global status report on physical activity 2022; 2022 (https://apps.who.int/iris/handle/10665/363607)

Page 16 of 43
and cycling and equitable access to safe, quality public open
spaces that enable and promote physical activity and active
mobility
P4 Implement whole-of-school programmes that include quality
physical education, and adequate facilities, equipment and
programs supporting active travel to/from school and support
physical activity for all children of all abilities during and after
school
Promoting physical activity
through schools: a toolkit (2021)
P5 Improve walking and cycling infrastructure ensuring universal
and equitable access to enable and promote safe walking,
cycling, other forms of micro mobility (e.g. wheelchairs, scooters
and skates) by people of all ages and abilities
P6 Implement multi-component workplace physical activity
programmes
P7 Provide and promote physical activity through provision of
community-based (grass roots) sport and recreation
programmes and conduct free mass participation events to
encourage engagement by people of all ages and abilities

Page 17 of 43
Objective 4: To strengthen and orient health systems to address the prevention and
control of noncommunicable diseases and the underlying social determinants through
people-centred primary health care and universal health coverage
Overarching/enabling actions
Integrate very cost-effective noncommunicable disease interventions into the basic primary health
care package with referral systems to all levels of care to advance the universal health coverage
agenda
Explore viable health financing mechanisms and innovative economic tools supported by evidence
Scale up early detection and coverage, prioritizing very cost-effective high-impact interventions
including cost-effective interventions to address behavioural risk factors
Train the health workforce and strengthen capacity of health system particularly at primary care
level to address the prevention and control of noncommunicable diseases
Improve the availability of the affordable basic technologies and essential medicines, including
generics, required to treat major noncommunicable diseases, in both public and private facilities
Implement other cost-effective interventions and policy options in objective 4 to strengthen and
orient health systems to address noncommunicable diseases and risk factors through people-
centered health care and universal health coverage
Develop and implement a palliative care policy, including access to opioids analgesics for pain
relief, together with training for health workers
Expand the use of digital technologies to increase health service access and efficacy for NCD
prevention, and to reduce the costs in health care delivery

Page 18 of 43
Cardiovascular disease
Specific interventions with WHO-CHOICE analysis
N°
Intervention
Non
-
economic
considerations
WHO tools
CV1 Pharmacological treatment of
hypertension in adults using either
of the following: thiazide and
thiazide-like agents; angiotensin-
converting enzyme inhibitors (ACE-
Is)/angiotensin-receptor blocker
(ARBs); calcium channel blockers
(CCBs).
Feasible to implement in all
settings and aligned to latest
WHO guidelines (2021)
Simple protocols can be
followed by non-physician
workers depending on the
country context
Guideline for the
pharmacological treatment of
hypertension in adults (2021)
Guideline for the
pharmacological treatment of
hypertension in adults:
summary (2022)
CV2a
Drug therapy (treatment with an
antihypertensive agent and a statin)
to control cardiovascular disease
risk using a total risk approach and
counselling to individuals who have
had a heart attack or stroke and to
persons with a high risk (≥20%) of
a fatal and non-fatal cardiovascular
event in the next 10 years using
WHO’s updated cardiovascular
disease risk charts
Feasibility and practicality of
implementation needs to be
assessed and determined.
Glucose control not included in
this intervention, but in the
diabetes intervention “Control of
blood pressure in people with
diabetes”
HEARTS technical package for
cardiovascular disease
management in primary health
care: risk based CVD
management (2020)
CV2b
Drug therapy (treatment with an
antihypertensive agent) to control
CVD risk using a total risk
approach and counselling to
individuals who have had a heart
attack or stroke and to persons with
high risk (≥10%) of a fatal and non-
fatal cardiovascular event in the
next 10 years using WHO’s
updated cardiovascular disease
risk charts
Feasibility and practicality of
implementation needs to be
assessed and determined.
Glucose control not included in
this intervention, but in the
diabetes intervention “Control of
blood pressure in people with
diabetes”
CV3 Treatment of new cases of acute
myocardial infarction with either:
acetylsalicylic acid, or
acetylsalicylic acid and
thrombolysis, or acetylsalicylic acid,
thrombolysis and clopidogrel, or
primary percutaneous coronary
interventions (PCI), with patients
initially treated in a hospital setting
with follow up carried out through
primary health care facilities at a
95% coverage rate
Selection of option depends on
health system capacity
CV4a
Treatment of acute ischemic stroke
with intravenous thrombolytic
therapy
Feasibility and practicality of
implementation needs to be
assessed and determined

Page 19 of 43
according to health systems
capacity.
CV4b
Treatment of acute ischemic stroke
with mechanical thrombectomy
within an experienced facility
Feasibility and practicality of
implementation needs to be
assessed and determined
according to health systems
capacity. Requires a surgical
facility with appropriately trained
workforce.
CV5a
Primary prevention of rheumatic
fever and rheumatic heart diseases
by increasing appropriate treatment
of streptococcal pharyngitis at the
primary care level
CV5b
Secondary prevention of rheumatic
fever and rheumatic heart disease
by developing a register of patients
who receive regular prophylactic
penicillin
CV6 Low-dose acetylsalicylic acid within
24 to 48 hours for secondary
prevention of ischemic stroke
CV7 Comprehensive* care of acute
stroke patients in stroke units
*Comprehensive care includes
strategies such as staffing by a
specialist stroke multidisciplinary
team, access to equipment for
monitoring and rehabilitation.
Early multidisciplinary approach
to be determined and depending
on country context. Composition
of rehabilitation workforce as an
integral part of multidisciplinary
team depends on health system
capacity.'
Other interventions from WHO guidance (without WHO-CHOICE analysis)
N°
Intervention
CV8 Treatment of congestive cardiac failure with angiotensin-converting-enzyme inhibitor, beta-
blocker and diuretic
CV9 Cardiac rehabilitation post myocardial infarction
CV10
Anticoagulation for medium-and high-risk non-valvular atrial fibrillation and for mitral stenosis
with atrial fibrillation
CV11
Treatment of hypertension using single pill combination anti-hypertensives
CV12
Secondary prevention of coronary heart disease with a statin, angiotensin-converting-enzyme
-inhibitor (ACE-I), beta-blocker and acetylsalicylic acid (low dose)
CV13
Seasonal influenza vaccination for people with cardiovascular diseases
CV14
COVID-19 vaccination for people with cardiovascular diseases

Page 20 of 43
Diabetes
Specific interventions with WHO-CHOICE analysis
N° Intervention Non-economic
considerations
WHO tools
D1
Foot care to prevent amputation in people
with diabetes (including educational
programmes, access to appropriate
footwear, multidisciplinary clinics)
HEARTS D: diagnosis
and management of type
2 diabetes (2020)
Classification of diabetes
mellitus (2019)
WHO package of
essential
noncommunicable (PEN)
disease interventions for
primary health care
(2020)
D2
Diabetic retinopathy screening for all
diabetes patients and laser photocoagulation
for prevention of blindness
Requires health staff
capacity for retinal
assessment and
photocoagulation
D3
Glycaemic control for people with diabetes,
along with standard home glucose
monitoring for people treated with insulin to
reduce diabetes complications
D4
Screening of people with diabetes for
albuminuria and treatment with angiotensin-
converting enzyme inhibitor for the
prevention and delay of renal disease
D5
Control of blood pressure in people with
diabetes
D6
Statin use in people with diabetes > 40years
old
Other interventions from WHO guidance (without WHO-CHOICE analysis)
N°
Intervention
D7 Seasonal influenza vaccination for people with diabetes
D8
COVID-19 vaccination for people with diabetes

Page 21 of 43
Chronic respiratory diseases
Specific interventions with WHO-CHOICE analysis
N° Intervention Non-economic
considerations
WHO tools
CR1
Acute treatment of asthma exacerbations
with inhaled bronchodilators and oral
steroids
Requires trained
providers at all levels of
healthcare
WHO package of essential
noncommunicable (PEN)
disease interventions for
primary health care (2020)
CR2
Acute treatment of chronic obstructive
pulmonary disease (COPD) exacerbations
with inhaled bronchodilators and oral
steroids
CR3
Long-term management of asthma with
inhaled bronchodilator and low-dose
beclometasone
CR4
Long-term management of COPD with
inhaled bronchodilator
Other interventions from WHO guidance (without WHO-CHOICE analysis)
N°
Intervention
CR5
Seasonal influenza vaccination for people with chronic respiratory
diseases
CR6
Access to improved stoves and cleaner fuels to reduce indoor air
pollution
CR7
Cost-effective interventions to prevent occupational lung diseases, for
example, from exposure to silica, asbestos
CR8
COVID-19 vaccination for people with chronic respiratory diseases

Page 22 of 43
Cancer
Specific interventions with WHO-CHOICE analysis
N° Intervention Non-economic
considerations
WHO tools
CA1 Vaccination against human papillomavirus
(1-2 doses) of 9–14-year-old girls
General
WHO report on cancer
(2020)
Cancer country profiles
Cancer control: six
modules (2014)
National cancer control
programmes core
capacity self-
assessment tool (2011)
Cervical cancer
Global strategy to
accelerate the
elimination of cervical
cancer as a public
health problem (2020)
Human papillomavirus
self-sampling as part of
cervical cancer
screening (2020)
Guideline for screening
and treatment of
cervical pre-cancer
lesions for cervical
cancer prevention
(2021)
WHO guidelines for the
use of thermal ablation
for cervical pre-cancer
lesions (2019)
Policy brief with
recommendations on
screening and treatment
to prevent cervical
cancer among women
living with HIV (2021)
Framework for
strengthening and
scaling-up services for
the management of
invasive cervical cancer
(2020)
CA2 Cervical cancer: HPV DNA screening,
starting at the age of 30 years with regular
screening every 5 to 10 years (using a
screen-and-treat approach or screen,
triage and treat approach)
CA3 Cervical cancer: early diagnosis programs
linked with timely diagnostic work-up and
comprehensive cancer treatment
CA4 Breast cancer: early diagnosis programs
linked with timely diagnostic work-up and
comprehensive cancer treatment
CA5 Breast Cancer: screening with
mammography (once every 2 years for
women aged 50-69 years) linked with
timely diagnostic work-up and
comprehensive breast cancer treatment in
setting where mammographic screening
programme is recommended
Requires systems
for organised,
population-based
screening
CA6 Colorectal cancer: early diagnosis
programs linked with timely diagnostic
work-up and comprehensive cancer
treatment
CA7 Basic palliative care for cancer: home-
based and hospital care with multi-
disciplinary team and access to opiates
and essential supportive medicines
Requires access to
controlled
medicines for pain
relief
CA8 Liver cancer: prevention of liver cancer
through hepatitis B immunization
24
CA9 Oral cancer: early detection programme of
oral cancer, including, as appropriate,
targeted screening programme for high-risk
groups in selected settings, according to
disease burden and health system
capacities, linked with comprehensive
cancer management
Requires systems
for organised,
population-based
screening
CA10
Colorectal cancer screening: population-
based programme, including through stool-
based tests, as appropriate, at age >50
Requires systems
for organised,
24
Cost effectiveness in prevention of liver cancer is optimal in countries with high hepatitis B prevalence and especially with
vaccination in early childhood and at birth, taking into account the feasibility and cost of vaccination

Page 23 of 43
years, linked with timely treatment in
settings where screening programme is
recommended
population-based
screening
Framework for
strengthening and
scaling-up services for
the management of
invasive cervical cancer
(2020)
WHO Position Paper on
HPV vaccines (2022)
Breast cancer
WHO position paper on
mammography
screening (2014)
Childhood cancer
Global initiative for
childhood cancer (2020)
CureAll framework:
WHO global initiative for
childhood cancer (2021)
Oral cancer
IARC Perspective on
Oral Cancer Prevention
(2022)
Global oral health status
report: towards
universal health
coverage for oral health
by 2030 (2022)
Other
Technical specifications
of radiotherapy
equipment for cancer
treatment (2021)
Guidelines for the
pharmacological and
radiotherapeutic
management of cancer
pain in adults and
adolescents (2019)
Practices to improve
coverage of the
hepatitis B birth dose
vaccine (2013)
Planning and
implementing palliative
care services: a guide
for programme
managers (2016)
CA11
Childhood cancer: early diagnosis
programs linked with timely diagnostic
work-up and comprehensive cancer
treatment, focusing on 6 index cancers of
WHO Global Initiative for Childhood
Cancer
CA12
Head and neck cancers including oral
cancers: early diagnosis programs linked
with timely diagnostic work-up and
comprehensive cancer treatment
CA13
Prostate cancer: early diagnosis programs
linked with timely diagnostic work-up and
comprehensive cancer treatment
CA14
Early detection and comprehensive
treatment of cancer for those living with
HIV

Page 24 of 43
Global atlas of palliative
care (2020)
WHO list of Priority
Medical Devices for
Cancer Management
(2017)
Other interventions from WHO guidance (without WHO-CHOICE analysis)
N°
Intervention
CA15
Seasonal influenza vaccination for people with cancer
CA16
COVID-19 vaccination for people with cancer

Page 25 of 43
Objective 5: To promote and support national capacity for high-quality research and
development for the prevention and control of noncommunicable diseases
Overarching/enabling actions
Develop and implement a prioritized national research agenda for noncommunicable diseases
Prioritize budgetary allocation for research on noncommunicable disease prevention and control
Strengthen human resources and institutional capacity for research
Strengthen research capacity through cooperation with foreign and domestic research institutes
Implement other policy options in objective 5 to promote and support national capacity for high-
quality research, development and innovation
Objective 6: To monitor the trends and determinants of noncommunicable diseases and
evaluate progress in their prevention and control
Overarching/enabling actions
Develop national targets and indicators based on global monitoring framework and linked with a
multisectoral policy and plan
Strengthen human resources and institutional capacity for surveillance and monitoring and
evaluation
Establish and or strengthen a comprehensive noncommunicable disease surveillance system,
including reliable registration of deaths by cause, cancer registration, periodic data collection on
risk factors and monitoring national response
Integrate noncommunicable disease surveillance and monitoring into national health information
systems
Implement other policy options in objective 6 to monitor trends and determinants of
noncommunicable diseases and evaluate progress in their prevention and control

Page 26 of 43
Methodological annex to Appendix 3
Detailed methodological information
Identification of interventions
The following criteria used for identifying interventions in 2017 were applied for the 2022 update:
(a) an intervention must have a demonstrated and quantifiable effect size, established in at least one
published study in a peer-reviewed journal;
(b) an intervention must have a clear link to one of the global NCD targets.
Additional interventions were considered using the same criteria as above. The proposed menu of
interventions for the newly updated Appendix 3 comprises the following (all the interventions presented in
the 2017 update have been re-analysed):
(a) interventions that have been unchanged from the last updated version (2017);
(b) interventions from the 2017 update that have been reworded or revised to reflect updates in WHO
policy or scientific evidence;
(c) interventions included in the 2017 update that had no analysis carried out at the time and for which
cost-effectiveness analysis has now been done for the 2022 update;
(d) new interventions deriving from WHO’s new guidance and technical products (Table 4).
Table 4: List of interventions for 2022 update and comparison with 2017 update
Interventions
Update of
original 2017
interventions (i)
Revised 2017
interventions (ii)
2017 intervention
with new CEA (iii)
New
interventions
with CEA (iv)
Objective 3
Tobacco 6 1
Harmful use of alcohol 5
Unhealthy diet 1 4 2
Physical inactivity 2
Objective 4
Cardio-vascular diseases 7 2 2 2
Diabetes 3 1 2
Chronic respiratory
diseases
3 1
Cancer 7 3 4
Total 31 9 8 10
CEA: cost-effectiveness analysis

Page 27 of 43
Choice of economic parameters
Economic parameters are listed below:
1. A menu of interventions for NCDs based on WHO-CHOICE methodology (see below) and presented
as a ratio of international dollars (I$) per healthy life year gained (HLYg)
25
.
a. Cost-effectiveness ratios are presented in bands, ranging from < I$100/HLYg to
>I$50,000/HLYg
26
. The decision to band cost-effectiveness was based on the consensus that
the data represent global estimates, therefore banding cost-effectiveness emphasises the
relative magnitude of cost-effectiveness rather than a specific amount.
2. Size of health gain: the expected size of population health impact for each intervention was calculated
based on total HLY gained per year in a standardized
27
population of 1 million people. HLY gained due
to an intervention are calculated over a 100-year time frame and evaluated at 95% coverage.
3. Economic cost of implementation: The total cost required per year to implement each intervention was
estimated, based on cost in I$ millions to implement in a standardized population of 1 million people
(i.e. I$ per capita)
While the same methodology has been used for the assessment of the cost-effectiveness of the
interventions ensuring comparability of results across areas, different modelling frameworks and
assumptions have been used for the modelling of each risk factor and disease. Detailed information on
methods, the evidence and assumptions underlying the interventions by disease and risk factor area are
provided in separate technical briefs. The evidence used for the modelling of interventions will be
periodically revised and updated, and changes in the estimates may occur in the future.
Country selection
Economic parameters were assessed for 3 country income-groups: low-income countries, lower-middle
income countries and upper-middle income countries and this is different compared to the 2017 update
where results were presented for 2 country income groups (low -and lower middle-income countries as one
group and upper-middle- and high-income countries as the second group). The current update includes
selected low -and middle-income countries (LMICs) only since the results from the updated Appendix 3 are
most relevant for these countries. Countries were selected so that a significant proportion of the total
population and health burden would be represented.
Sixty-two countries were considered in the analysis and listed in Table 5 below
28
. The list of countries
included all low-income countries, the 20 most populous lower-middle-income countries and the 20 most
populous upper-middle-income countries. Combined, they represent nearly 80% of the total population and
80% of the global burden of disease. For some type of interventions (e.g. harmful use of alcohol), the
analysis was based on a smaller subset of countries.
Table 5: Classification of countries by World Bank income level (2019)
25
The HLY is the equivalent of the Disability Adjusted Life Years (DALYs) used in the 2017 update but framed in a positive way.
DALYs are averted while HLY are gained.
26
Cost-effectiveness bands (in I$) are: <100, 100-$500, 500-1,000, 1,000-5,000, 5,000-10,000, 10,000-20,000, 20,000-50,000,
>50,000.
27
Standardized over the total population of the analysed countries per income grouping
28
The 2017 update included 20 countries.

Page 28 of 43
Low-income countries
Lower middle-income
countries
Upper middle-income
countries
29
Afghanistan Algeria Argentina
Burkina Faso Angola Brazil
Burundi Bangladesh China
Central African Republic Cameroon Colombia
Chad Côte d'Ivoire Dominican Republic
Democratic Republic of the Congo Egypt Ecuador
Eritrea Ghana Guatemala
Ethiopia India Indonesia
Gambia Kenya Iran (Islamic Republic of)
Guinea Morocco Iraq
Guinea-Bissau Myanmar Jordan
Haiti Nepal Kazakhstan
Madagascar Nigeria Malaysia
Malawi Pakistan Mexico
Mali Philippines Peru
Mozambique Sri Lanka Russian Federation
Niger Ukraine South Africa
Rwanda United Republic of Tanzania Thailand
Sierra Leone Uzbekistan Turkey
Sudan Viet Nam
Tajikistan
Togo
Uganda
WHO-CHOICE: A brief methodological overview
General approach
Value for money and efficiency are fundamental considerations guiding investment in health, and WHO-
CHOICE provides a way to measure them. This is true in settings where lack of finance is no longer the
greatest barrier to achieving better health outcomes; it is also true in less well-resourced settings, where
inefficiency is measured in lives lost and human suffering. Cost-effectiveness analysis supports priority
setting by defining areas of action where the greatest health gains can be achieved.
Generalized cost-effectiveness analysis (WHO-CHOICE) also allows the definition of an optimal set of
interventions, taking into account setting-specific factors such as the burden of disease, health system
practice, and economic conditions. Tools to facilitate country-level cost-effectiveness analysis of a wide
29
One upper-middle income country was excluded during analysis due to lack of data

Page 29 of 43
range of health activities are available. In parallel, WHO-CHOICE publishes and disseminates online a
knowledge base of regional-level cost-effectiveness information
30
.
The use of cost-effectiveness analysis within decision making processes in health is increasingly common
globally. However, a series of methodological shortcomings may limit the practical application of cost-
effectiveness analysis results. Two examples of this are methodological differences between studies that
limit comparability, and use of the current practice as a comparator, which implicitly assumes current
resource use is efficient. Generalized Cost-Effectiveness Analysis (GCEA) was developed to overcome
such shortcomings of traditional cost-effectiveness analysis.
The GCEA approach enables both existing and new interventions to be evaluated simultaneously. The
comparator used in GCEA is a hypothetical “null” scenario, where the impacts of all currently implemented
interventions are removed. Uniquely, this method allows existing and new interventions to be analysed at
the same time.
Previous cost-effectiveness analyses have been restricted to assessing the efficiency of adding a single
new intervention to the existing set or replacing one existing intervention with an alternative. Using WHO-
CHOICE, the analyst is no longer constrained by what is already being done, and policymakers can revisit
and revise past choices if necessary and feasible. They will have a rational basis for deciding to reallocate
resources between interventions to achieve social objectives.
WHO-CHOICE:
Uses a standardized method for cost-effectiveness analysis that can be applied to all interventions in
different settings
All interventions are evaluated compared to the “null”, a scenario in which we model the absence of
health care interventions
Impact models are developed using a population-based approach, and healthy life years gained due
to an intervention are calculated over a 100-year time frame. Health impacts are not discounted.
Costs for each intervention are developed using an ingredient based economic costing methodology.
Costs are expressed in international dollars (I$) to ensure comparability across countries and country
income groups. Costs are calculated over a 100-year time frame and discounted at 3% per year.
All interventions are evaluated at 95% coverage.
30
World Health Organization Choosing Interventions that are Cost-Effective (WHO-CHOICE) programme:
https://www.who.int/teams/health-systems-governance-and-financing/economic-analysis

Page 30 of 43
Table 2: Summary of WHO-CHOICE economic analyses for interventions for NCD prevention and control
Notes: The tables below list all interventions for which WHO-CHOICE economic analysis is available. In this example, separate tables are provided for each of the
four main risk factors and four main diseases covered by Objectives 3 and 4 of the WHO Global NCD Action Plan. The intervention name contains more exact detail
about the intervention that was modelled -note that these may differ slightly from the wording of the WHO recommended interventions. This Annex is provided for
background scientific information only and should not be used as a specific menu for implementation.
Low-income
Lower-middle-income
Upper-middle-income
N° Intervention
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health impact
per year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Tobacco use
T1
Increase excise taxes and prices on
tobacco products
<100 1,717 <0.01 <100 2,674 0.01 <100 3,093 0.01
T2
Implement large graphic health
warnings on all tobacco packages,
accompanied by plain/standardized
packaging
<100 1,212 <0.01 <100 2,181 0.01 <100 2,319 0.01
T3
Enact and enforce comprehensive
bans on tobacco advertising,
promotion and sponsorship
<100 933 <0.01 <100 1,490 0.01 <100 1,535 0.01
T4
Eliminate exposure to second-hand
tobacco smoke in all indoor
workplaces, public places, public
transport
<100 1,475 <0.01 <100 2,845 0.01 <100 3,077 0.02
T5
Implement effective mass media
campaigns that educate the public
about the harms of smoking/tobacco
use and second hand smoke, and
encourage behaviour change
<100 1,345 0.01 <100 2,516 0.03 <100 2,701 0.10
T6
Provision of cost-covered effective
population-wide support (including
brief advice, national toll-free quit
line services and mCessation) for
tobacco cessation to all tobacco
users.
<100 1,028 0.02 <100 1,724 0.05 <100 1,800 0.09
T7
Provision of cost-covered effective
pharmacological interventions to all
tobacco users who want to quit
,
<100
1,761
0.08
100 – 500
3,583
0.71
100 – 500
3,924
1.32

Page 31 of 43
Low-income
Lower-middle-income
Upper-middle-income
N° Intervention
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health impact
per year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
through the use of nicotine
replacement therapy (NRT),
Bupropion and Verenicline.
Harmful use of alcohol
A1
Increase excise taxes on alcoholic
beverages
<100 155 0.01 <100 445 0.02 <100 797 0.04
A2
Enact and enforce bans or
comprehensive restrictions on
exposure to alcohol advertising
(across multiple types of media)
<100 121 <0.01 <100 377 0.01 100 - 500 158 0.03
A3
Enact and enforce restrictions on
the physical availability of retailed
alcohol (via
reduced hours of sale)
<100 132 0.01 <100 383 0.03 100 - 500 190 0.05
A4
Enact and enforce drink-driving laws
and blood alcohol concentration
limits via sobriety checkpoints
100 - 500 104 0.01 100 - 500 321 0.04 1,000 - 5,000 44 0.11
A5
Provide brief psychosocial
intervention for persons with
hazardous and harmful alcohol use
<100 244 0.02 100 - 500 647 0.07 100 - 500 691 0.29
Unhealthy diet
H1
Reformulation policies for healthier
food and beverage products (e.g.
elimination of trans-fatty acids
and/or reduction of saturated fats,
free sugars and/or sodium)
<100 2,449 0.01 <100 4,038 0.02 <100 4,704 0.06
H2
Front-of-pack labelling as part of
comprehensive nutrition labelling
policies for facilitating consumers’
understanding and choice of food
for healthy diets
<100 4,042 <0.01 <100 7,441 0.01 <100 9,069 0.02
H3
Public food procurement and
service policies for healthy diets
(e.g. to reduce the intake of free
sugars, sodium, unhealthy fats, and
to increase the consumption of
<100 449 0.01 <100 472 0.02 <100 441 0.04

Page 32 of 43
Low-income
Lower-middle-income
Upper-middle-income
N° Intervention
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health impact
per year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
legumes, wholegrains, fruits and
vegetables)
H4
Behaviour change communication
and mass media campaign for
healthy diets (e.g. to reduce the
intake of energy, free sugars,
sodium, unhealthy fats, and to
increase the consumption of
legumes, wholegrains, fruits and
vegetables)
<100 2,257 0.01 <100 3,152 0.03 <100 3,506 0.12
H5 Policies to protect children from the
harmful impact of food marketing on
diet
<100 297 <0.01 <100 446 0.01 <100 610 0.02
H6
Protection, promotion and support
of optimal breastfeeding practices
<100 2,052 0.07 <100 3,049 0.11 <100 2,964 0.16
H7
Taxation on sugar-sweetened
beverages as pat of fiscal policies
for healthy diets
100 - 500 7 <0.01 100 - 500 12 <0.01 100 - 500 41 <0.01
Physical inactivity
P1
Brief counselling intervention on
physical activity in primary health
care
100 - 500 246 0.07 100 - 500 732 0.30 1,000 - 5,000 296 0.90
P2
Physical activity public education
and awareness campaign
<100 185 <0.01 <100 617 0.01 100 - 500 162 0.04
Cardiovascular diseases
CV1
Pharmacological treatment of
hypertension in adults using either
of the following: thiazide and
thiazide-like agents; angiotensin-
converting enzyme inhibitors (ACE-
Is)/angiotensin-receptor blocker
(ARBs); calcium channel blockers
(CCBs).
100 - 500 5,281 2.12 500 - 1,000 1,435 0.78 500 - 1,000 3,002 1.97
CV2a
Drug therapy (treatment with an
antihypertensive and statin) to
100 - 500 435 0.21 1,000 - 5,000 274 0.29 500 - 1,000 1,166 0.82

Page 33 of 43
Low-income
Lower-middle-income
Upper-middle-income
N° Intervention
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health impact
per year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
control CVD risk using a total risk*
approach and counselling to
individuals who have had a heart
attack or stroke and to persons with
high risk (≥ 20%) of a fatal and non-
fatal cardiovascular event in the
next 10 years using the updated
WHO CVD risk charts
CV2b
Drug therapy (treatment with an
antihypertensive) to control CVD
risk using a total risk* approach and
counselling to individuals who have
had a heart attack or stroke and to
persons with high risk (≥ 10%) of a
fatal and non-fatal cardiovascular
event in the next 10 years using the
updat
ed WHO CVD risk charts
500 - 1,000 2,389 1.24 500 - 1,000 762 0.64 500 - 1,000 2,107 1.79
CV3a
Treatment new cases of acute
myocardial infarction with
acetylsalicylic acid initially treated in
a hospital setting with follow up
carried out through primary health
care facilities at a 95% coverage
rate
10,000 -
15,000
7.9 0.08
15,000 -
20,000
2.7 0.04
20,000 -
50,000
3.9 0.08
CV3b
Treatment new cases of acute
myocardial infarction with
acetylsalicylic acid and
thrombolysis, with patients initially
treated in a hospital setting with
follow up carried out through
primary health care facilities at a
95% coverage rate
5,000 -
10,000
13.0 0.13
15,000 -
20,000
3.7 0.06
15,000 -
20,000
6.1 0.12
CV3c
Treatment of new cases of acute
myocardial infarction with
acetylsalicylic acid, thrombolysis
and clopidogrel, with patients
initially treated in a hospital setting
with follow up carried out through
5,000 -
10,000
15.4 0.14
15,000 -
20,000
4.2 0.06
15,000 -
20,000
7.2 0.12
Page 34 of 43
Low-income
Lower-middle-income
Upper-middle-income
N° Intervention
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health impact
per year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
primary health care facilities at a
95% coverage rate
CV3d
Treatment of new cases of
myocardial infarction with primary
percutaneous coronary
interventions (PCI), acetylsalicylic
acid and clopidogrel, with patients
initially treated in a hospital setting
with follow up carried out through
primary health care facilities at a
95% coverage rate
>50,000 7.8 1.00 >50,000 2.6 0.24 >50,000 3.9 0.56
CV4a
Treatment of acute ischemic stroke
with intravenous thrombolytic
therapy
5,000 -
10,000
18.3 0.17
10,000 -
15,000
5.3 0.07
15,000 -
20,000
16.9 0.27
CV4b
Treatment of acute ischemic stroke
with mechanical thrombectomy
within an experienced facility
20,000 -
50,000
8.0 0.40
20,000 -
50,000
2.9 0.10 >50,000 7.6 0.48
CV5a
Primary prevention of rheumatic
fever and rheumatic heart diseases
by increasing appropriate treatment
of streptococcal pharyngitis at the
primary care level
100 - 500 3,430.0 0.44 100 - 500 989.0 0.14 100 - 500 622.4 0.28
CV5b
Secondary prevention of rheumatic
fever and rheumatic heart disease
by developing a register of patients
who receive regular prophylactic
penicillin
<100 722.2 0.03 <100 200.0 0.01 <100 121.9 0.01
CV6
Low-dose acetylsalicylic acid within
24 to 48 hours for secondary
prevention of ischemic stroke
20,000 -
50,000
0.8 0.03
10,000 -
15,000
1.2 0.02 >50,000 1.0 0.06
CV7
Comprehensive care of acute stroke
patients in stroke units
>50,000 1.6 0.22 >50,000 1.4 0.11 >50,000 1.8 0.39
Diabetes
D1 Foot care to prevent amputation in
people with diabetes (including
educational programmes, access to
100 - 500 80 0.03 1,000 - 5,000 99 0.10 1,000 - 5,000 176 0.20

Page 35 of 43
Low-income
Lower-middle-income
Upper-middle-income
N° Intervention
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health impact
per year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
appropriate footwear,
multidisciplinary clinics)
D2
Diabetic retinopathy screening for
all diabetes patients and laser
photocoagulation for prevention of
blindness
1,000 - 5,000 32 0.04 1,000 - 5,000 48 0.17 1,000 - 5,000 133 0.34
D3
Glycaemic control for people with
diabetes, along with standard home
glucose monitoring for people
treated with insulin to reduce
diabetes complications
500 - 1,000 1,091 0.75 1,000 - 5,000 1,996 2.51 1,000 - 5,000 2,784 3.96
D4
Screening of people with diabetes
for albuminuria and treatment with
angiotensin-converting enzyme
inhibitor for the prevention and
delay of renal disease
100 - 500 526 0.12 100 - 500 1,012 0.44 500 - 1,000 1,192 0.78
D5
Control of blood pressure in people
with diabetes
100 - 500 274 0.04 100 - 500 532 0.17 500 - 1,000 824 0.50
D6
Statin use in people with diabetes >
40years old
<100 515 0.05 100 – 500 1,271 0.22 100 – 500 1,559 0.61
Chronic Respiratory Diseases
CR1
Acute treatment of asthma
exacerbations with inhaled
bronchodilators and oral steroids
<100 1,220 0.05 100 - 500 1,051 0.13 500 - 1,000 828 0.43
CR2
Acute treatment of COPD
exacerbations with inhaled
bronchodilators and oral steroids
<100 183 <0.01 100 - 500 378 0.04 100 - 500 389 0.16
CR3
Long-term management of asthma
with inhaled bronchodilator and low-
dose beclometasone
<100 1,204 0.10 100 - 500 1,123 0.16 100 - 500 733 0.32
CR4
Long-term management of COPD
with inhaled bronchodilator
<100
920
0.03
<100
1,811
0.16
100 - 500
1,723
0.39

Page 36 of 43
Low-income
Lower-middle-income
Upper-middle-income
N° Intervention
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health impact
per year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Cancer
CA1
Vaccination against human
papillomavirus (1-2 doses) of 9–14
year old girls
<100 2,170 0.04 <100 1,878 0.05 <100 2,524 0.05
CA2
Cervical cancer: HPV DNA
screening, starting at the age of 30
years with regular screening every 5
to 10 years (using a screen-and-
treat approach or screen, triage and
treat approach)
<100 1,012 0.02 <100 940 0.05 <100 1,686 0.14
CA3
Cervical cancer: early diagnosis
programs linked with timely
diagnostic work-up and
comprehensive cancer treatment
<100 621 0.02 <100 605 0.02 <100 578 0.03
CA4
Breast cancer: early diagnosis
programs linked with timely
diagnostic work-up and
comprehensive cancer treatment
<100 929 0.05 <100 1,405 0.11 100 - 500 2,721 0.30
CA5
Breast Cancer: Screening with
mammography (once every 2 years
for women aged 50-69 years) linked
with timely diagnostic work-up and
comprehensive breast cancer
treatment in setting where
mammographic screening
programme is recommended
100 - 500 990 0.17 100 - 500 1,492 0.39 100 - 500 2,900 0.94
CA6
Colorectal cancer: early diagnosis
programs linked with timely
diagnostic work-up and
comprehensive cancer treatment
<100 356 0.02 <100 643 0.04 100 - 500 2,877 0.34
CA7
Basic palliative care for cancer:
home-based and hospital care with
multi
-
disciplinary team and access
<0.01
<0.01
0.02

Page 37 of 43
Low-income
Lower-middle-income
Upper-middle-income
N° Intervention
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health impact
per year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
to opiates and essential supportive
medicines
31
CA8
Prevention of liver cancer through
hepatitis B immunization
32
<100 213 0.01 100 - 500 175 0.02 <100 684 0.01
CA9
Oral cancer: early detection
programme of oral cancer,
including, as appropriate, targeted
screening programme for high-risk
groups in selected settings,
according to disease burden and
health system capacities, linked with
comprehensive cancer
management
1,000 - 5,000 43 0.12 100 - 500 1,371 0.38 1,000 - 5,000 227 0.90
CA10
Colorectal cancer screening:
population-based programme,
including through stool-based tests,
as appropriate, at age >50 years,
linked with timely treatment in
settings where screening
programme is recommended
100 - 500 564 0.11 100 - 500 1,036 0.29 100 - 500 4,613 1.13
CA11
Childhood cancer: early diagnosis
programs linked with timely
diagnostic work-up and
comprehensive cancer treatment,
focusing on 6 index cancers of
WHO Global Initiative for Childhood
Cancer
<100 262 0.02 <100 1,148 0.10 <100 354 0.03
CA12
Head and neck cancers including
oral cancers: early diagnosis
programs linked with timely
diagnostic work-up and
comprehensive cancer treatment
500 - 1,000 18 0.01 500 - 1,000 102 0.08 1,000 - 5,000 47 0.05
31
Impact model not available for palliative care
32
Cost effectiveness in prevention of liver cancer is optimal in countries with high hepatitis B prevalence and especially with vaccination in early childhood and at birth, taking into
account the feasibility and cost of vaccination

Page 38 of 43
Low-income
Lower-middle-income
Upper-middle-income
N° Intervention
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health impact
per year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
Banded cost-
effectiveness
ratio
Health
impact per
year (HLY
gained per 1
million)
Economic
cost per
year (I$ in
millions per
1 million)
CA13
Prostate cancer: early diagnosis
programs linked with timely
diagnostic work-up and
comprehensive cancer treatment
100 - 500 224 0.03 100 - 500 272 0.05 100 - 500 1,040 0.19
CA14
Early detection and comprehensive
treatment of cancer for those living
with HIV
<100 247 0.01 <100 84 <0.01 100 - 500 34 <0.01

Page 39 of 43
Table 3: Ranking of interventions by average cost-effectiveness ratio for NCD risk factors and non-communicable diseases based on
analysis in low and lower-middle income countries
N°
Intervention
Banded cost-
effectiveness
ratio
Health impact
per year (HLY
gained per 1
million)
Economic cost
per year (I$ in
millions per 1
million)
Tobacco use
T1 Increase excise taxes and prices on tobacco products
<100 2,400 0.01
T2 Implement large graphic health warnings on all tobacco packages, accompanied by
plain/standardized packaging
<100 1,904 0.01
T3 Enact and enforce comprehensive bans on tobacco advertising, promotion and
sponsorship
<100 1,331 0.01
T4 Eliminate exposure to second-hand tobacco smoke in all indoor workplaces, public places,
public transport
<100 2,453 0.01
T5 Implement effective mass media campaigns that educate the public about the harms of
smoking/tobacco use and second hand smoke, and encourage behaviour change
<100 2,182 0.02
T6 Provision of cost-covered effective population-wide support (including brief advice,
national toll-free quit line services and mCessation) for tobacco cessation to all tobacco
users.
<100 1,525 0.04
T7 Provision of cost-covered effective pharmacological interventions to all tobacco users who
want to quit, through the use of nicotine replacement therapy (NRT), Bupropion and
Varenicline.
100 - 500 3,062 0.53
Harmful use of alcohol
A1 Increase excise taxes on alcoholic beverages
<100 362 0.02
A2 Enact and enforce bans or comprehensive restrictions on exposure to alcohol advertising
(across multiple types of media)
<100 304 0.01
A3 Enact and enforce restrictions on the physical availaility of retailed alcohol (via reduced
hours of sale)
<100 311 0.02
A4 Enact and enforce drink-driving laws and blood alcohol concentration limits via sobriety
checkpoints
100 - 500 259 0.03
A5 Provide brief psychosocial intervention for persons with hazardous and harmful alcohol
use
100 – 500
532
0.05
Page 40 of 43
Unhealthy diet
H1 Reformulation policies for healthier food and beverage products (e.g. elimination of trans-
fatty acids and/or reduction of saturated fats, free sugars and/or sodium)
<100 3,584 0.02
H2 Front-of-pack labelling as part of comprehensive nutrition labelling policies for facilitating
consumers’ understanding and choice of food for healthy diets
<100 6,470 0.01
H3 Public food procurement and service policies for healthy diets (e.g. to reduce the intake of
free sugars, sodium, unhealthy fats, and to increase the consumption of legumes,
wholegrains, fruits and vegetables)
<100 465 0.02
H4 Behaviour change communication and mass media campaign for healthy diets (e.g. to
reduce the intake of energy, free sugars, sodium, unhealthy fats, and to increase the
consumption of legumes, wholegrains, fruits and vegetables)
<100 2,897 0.03
H5 Policies to protect children from the harmful impact of food marketing on diet
<100 403 0.01
H6 Protection, promotion and support of optimal breastfeeding practices
<100 2,764 0.10
H7 Taxation on sugar-sweetened beverages as pat of fiscal policies for healthy diets
100 - 500 11 <0.01
Physical inactivity
P2 Implement sustained, population wide, best practice communication campaigns to
promote physical activity, with links to community-based programmes and environmental
improvements to enable and support behaviour change.
<100 451 0.01
P1 Provide physical activity assessment, counselling, and behaviour change support as part
of routine primary health care services through the use of a brief intervention
500 - 1,000 573 0.38
Cardiovascular diseases
CV5b Secondary prevention of rheumatic fever and rheumatic heart disease by developing a
register of patients who receive regular prophylactic penicillin
<100 349 0.01
CV1 Pharmacological treatment of hypertension in adults using either of the following: thiazide
and thiazide-like agents; angiotensin-converting enzyme inhibitors (ACE-Is)/angiotensin-
receptor blocker (ARBs); calcium channel blockers (CCBs).
100 - 500 2,535 1.16
CV5a Primary prevention of rheumatic fever and rheumatic heart diseases by increasing
appropriate treatment of streptococcal pharyngitis at the primary care level
100 - 500 1,687 0.23
CV2a Drug therapy (treatment with an antihypertensive and statin) to control CVD risk using a
total risk approach and counselling to individuals who have had a heart attack or stroke
and to persons with high risk (≥ 20%) of a fatal and non-fatal cardiovascular event in the
next 10 years using the updated WHO CVD risk charts
500 - 1,000 320 0.27

Page 41 of 43
CV2b Drug therapy (treatment with an antihypertensive) to control CVD risk using a total risk
approach and counselling to individuals who have had a heart attack or stroke and to
persons with high risk (≥ 10%) of a fatal and non-fatal cardiovascular event in the next 10
years using the updated WHO CVD risk charts
500 - 1,000 1,227 0.81
CV3a Treatment new cases of acute myocardial infarction with acetylsalicylic acid, initially
treated in a hospital setting with follow up carried out through primary health care facilities
at a 95% coverage rate
10,000 - 15,000 4 0.05
CV3b Treatment of new cases of acute myocardial infarction with acetylsalicylic acid and
thrombolysis, with patients initially treated in a hospital setting with follow up carried out
through primary health care facilities at a 95% coverage rate
10,000 - 15,000 6 0.08
CV3c Treatment of new cases of acute myocardial infarction with acetylsalicylic acid,
thrombolysis and clopidogrel, with patients initially treated in a hospital setting with follow
up carried out through primary health care facilities at a 95% coverage rate
10,000 - 15,000 7 0.09
CV4a Treatment of acute ischemic stroke with intravenous thrombolytic therapy
10,000 - 15,000 9 0.10
CV6 Low-dose acetylsalicylic acid within 24 to 48 hours for secondary prevention of ischemic
stroke
15,000 - 20,000 1 0.02
CV4b Treatment of acute ischemic stroke with mechanical thrombectomy within an experienced
facility
20,000 - 50,000 4 0.19
CV3d Treatment of new cases of myocardial infarction with primary percutaneous coronary
interventions (PCI), acetylsalicylic acid and clopidogrel, with patients initially treated in a
hospital setting with follow up carried out through primary health care facilities at a 95%
coverage rate
>50,000 4 0.46
CV7 Comprehensive care of acute stroke patients in stroke units
>50,000 1 0.14
Diabetes
D4 Screening of people with diabetes for albuminuria and treatment with angiotensin-
converting enzyme inhibitor for the prevention and delay of renal disease
100 - 500 873 0.35
D5 Control of blood pressure in people with diabetes
100 - 500 459 0.14
D6 Statin use in people with diabetes > 40years old
100 - 500 1,055 0.17
D1 Foot care to prevent amputation in people with diabetes (including educational
programmes, access to appropriate footwear, multidisciplinary clinics)
500 - 1,000 93 0.08
D2 Diabetic retinopathy screening for all diabetes patients and laser photocoagulation for
prevention of blindness
1,000 - 5,000 44 0.13

Page 42 of 43
D3 Glycaemic control for people with diabetes, along with standard home glucose monitoring
for people treated with insulin to reduce diabetes complications
1,000 - 5,000
1,737
2.01
Chronic respiratory diseases
CR1 Acute treatment of asthma exacerbations with inhaled bronchodilators and oral steroids
<100 1,100 0.11
CR2 Acute treatment of COPD exacerbations with inhaled bronchodilators and oral steroids
<100 322 0.03
CR4 Long-term management of COPD with inhaled bronchodilator
<100 1,556 0.12
CR3 Long-term management of asthma with inhaled bronchodilator and low-dose
beclometasone
100 - 500 1,146 0.14
Cancer
CA1 Vaccination against human papillomavirus (1-2 doses) of 9–14 year old girls <100 1,962 0.05
CA2 Cervical cancer: HPV DNA screening, starting at the age of 30 years with regular
screening every 5 to 10 years (using a screen-and-treat approach or screen, triage and
treat approach)
<100 961 0.04
CA3 Cervical cancer: early diagnosis programs linked with timely diagnostic work-up and
comprehensive cancer treatment
<100 610 0.02
CA4 Breast cancer: early diagnosis programs linked with timely diagnostic work-up and
comprehensive cancer treatment
<100 1,269 0.09
CA6 Colorectal cancer: early diagnosis programs linked with timely diagnostic work-up and
comprehensive cancer treatment
<100 561 0.04
CA8 Prevention of liver cancer through hepatitis B immunization
33
<100 186 0.02
CA11 Childhood cancer: early diagnosis programs linked with timely diagnostic work-up and
comprehensive cancer treatment, focusing on 6 index cancers of WHO Global Initiative for
Childhood Cancer
<100 895 0.08
CA14 Early detection and comprehensive treatment of cancer for those living with HIV <100 131 <0.01
CA5 Breast Cancer: Screening with mammography (once every 2 years for women aged 50-69
years) linked with timely diagnostic work-up and comprehensive breast cancer treatment
in setting where mammographic screening programme is recommended
100 - 500 1,349 0.33
33
Cost effectiveness in prevention of liver cancer is optimal in countries with high hepatitis B prevalence and especially with vaccination in early childhood and at birth, taking into
account the feasibility and cost of vaccination

Page 43 of 43
CA9 Oral cancer: early detection programme of oral cancer, including, as appropriate, targeted
screening programme for high-risk groups in selected settings, according to disease
burden and health system capacities, linked with comprehensive cancer management
100 - 500 991 0.31
CA13 Prostate cancer: early diagnosis programs linked with timely diagnostic work-up and
comprehensive cancer treatment
100 - 500 258 0.04
CA10 Colorectal cancer screening: population-based programme, including through stool-based
tests, as appropriate, at age >50 years, linked with timely treatment in settings where
screening programme is recommended
100 - 500 901 0.24
CA12 Head and neck cancers including oral cancers: early diagnosis programs linked with
timely diagnostic work-up and comprehensive cancer treatment
500 - 1,000 78 0.06
CA7 Basic palliative care for cancer: home-based and hospital care with multi-disciplinary team
and access to opiates and essential supportive medicines
34
<0.01
34
Impact model not available for palliative care
