
For Patient Care Report/Handoffs
I-PASS
Nursing Professional Development

What do you think?
Approximately what percentage of
sentinel events involve some type of
miscommunication?
(Click on your answer)
(Starmer et al., 2012)
And over 50% of the miscomunnications are
related to handoffs!
89%
52%
67%
Try again
Try again
Correct

What do you think?
What is the dollar amount healthcare
institutions in the U.S. lose annually
due to communication-related
malpractice cases?
(Click for the answer)
Patient care handoffs are one area where
communication can be improved.
$1.1 Billion

Purpose
Ineffective handoff
communication is
recognized as a critical
patient safety challenge in
healthcare.

Texas Children’s is implementing an evidence-based,
standardized format for communicating
report/handoffs of patient care.
The Joint Commission (2017) defines a handoff as “a
transfer and acceptance of patient care responsibility
achieved through effective communication.”
This is a system-wide initiative inclusive of Inpatient
and Ambulatory areas in the Texas Medical Center,
West Campus, and The Woodlands Campus.
I-PASS is currently being used by the Advanced Practice
Providers at TCH and in the Emergency Center and
CICU.
Purpose

Learning Outcome
Describe the use of the I-PASS
mnemonic as a standardized format
for communicating report/handoffs of
patient care.
Following completion of this online course,
clinicians will be required to demonstrate use of
the I-PASS format while communicating
report/handoff of patient care. This will be
explained in greater detail at the end of this course.

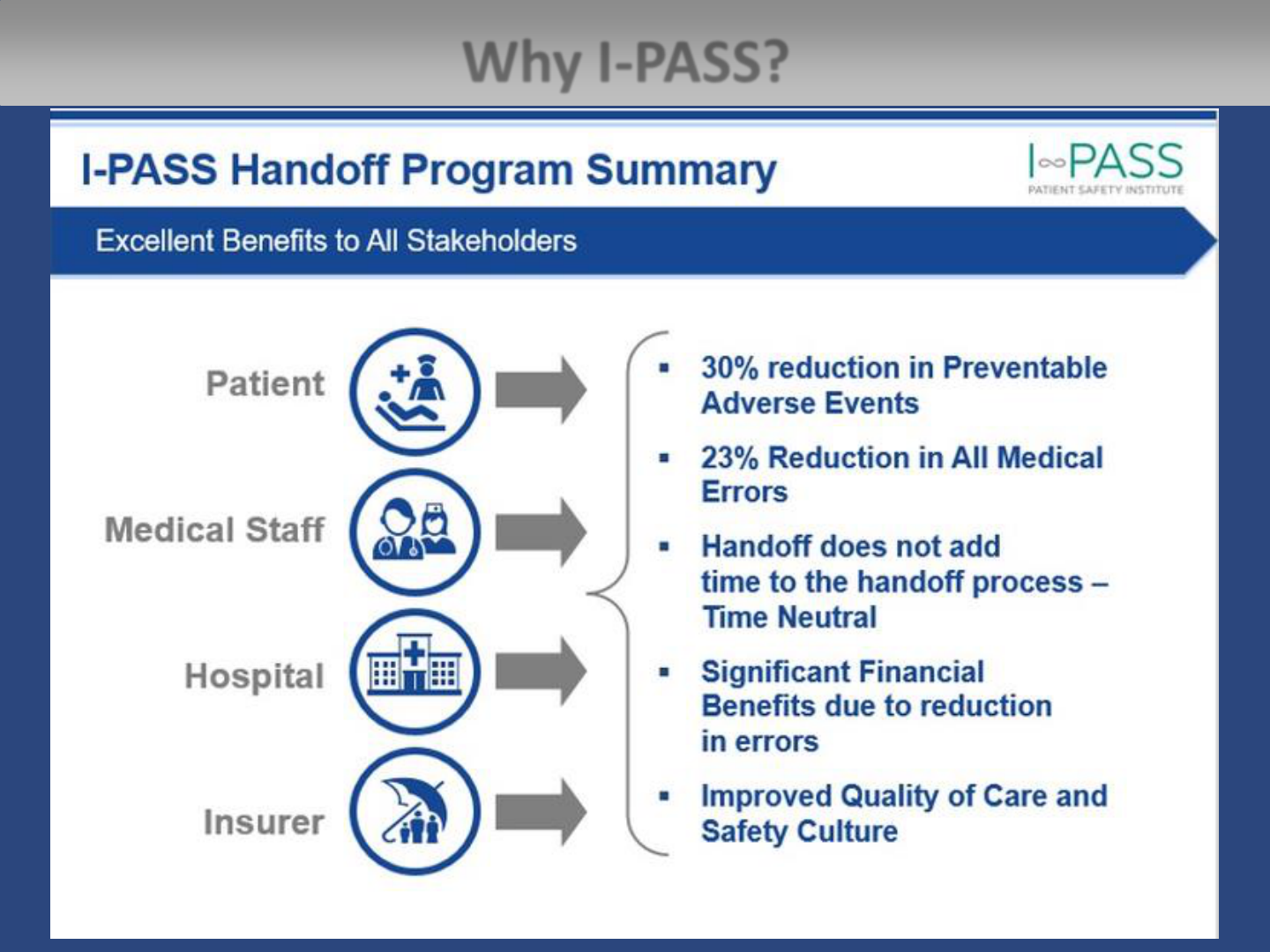
Why I-PASS?
I-PASS is an evidence-based package of
interventions created to reduce communication
failures during patient handoffs.
I-PASS is the most validated and effective method
for handoffs in the hospital. It was found to
substantially reduce injuries due to medical errors
in a major multicenter study published in 2014 in
the New England Journal of Medicine.
I-PASS is successfully being used by 70 leading
hospitals in the U.S.
No other handoff approach has such strong
evidence of effectiveness.
Why I-PASS?

Why I-PASS?
The last step in I-PASS is “Synthesis” where the “receiver” of the
patient care handoff repeats/reads back to summarize what was
heard; asks questions & restates key action/to do items.
So what is missing in the
SBAR format that makes
I-PASS more effective?
(click once)
Report
Giver
Report
Receiver/
Synthesizer

Joint Commission Standard
In 2010, Standard of Care PC.02.02.01 was created from a
2006 National Patient Safety Goal related to communication:
The organization coordinates the patient’s care, treatment,
and services based on the patient’s needs.
Element of Performance (EP) 2:
The organization’s process for hand-off communication
provides the opportunity for discussion between the giver
and receiver of patient information. Note: Such information
may included the patient’s condition, treatment, medications,
services, and any recent or anticipated changes of any of
these (Joint Commission, 2017).
The “Synthesis” in I-PASS facilitates this
discussion between the giver and receiver of
patient information.

What is the I-PASS Mnemonic?
I = Illness severity (Stable, “Watcher,” Unstable)
P = Patient Summary (Summary statement; events leading
up to admission; hospital course; ongoing assessment;
plan)
A = Action List (To do list; timeline and ownership)
S = Situation Awareness (Know what’s going on; plan for
what might happen)
S = Synthesis by Receiver (Receiver summarizes what was
heard; asks questions; restates key action/to do items)

I-PASS as Compared to SBAR
I =
Illness Severity
• How sick is the patient?
• Stable, Improving, Watch closely. Code
status
S = Situation
P = Patient Summary
• Brief patient overview
B
= Background
A = Action List
• Pending tasks
A
= Assessment
S = Situation Awareness & Contingency Plan
• Know what’s going on
• Plan for what might happen using if/then
statements
• Suggestions
R = Recommendations
S = Synthesis
• Receiver summarizes what was heard;
asks questions; restates key action/to do
items.
Addition of the receiver
summarizing/clarifying with
the messenger

• Stable: patients you are not worried about
• Improving: Not acutely unstable but have
potential to worsen
A good example is a patient that looks comfortable
on a high level of oxygen support. They are stable
now, but given the degree of support, they have
the potential to worsen.
• Watch Closely: patients that are acutely
ill/unstable
• Code Status
I – Illness Severity

• Summary statement or “one-liner”
• Identification Statement, weight, allergies, code
status
• Events leading to admission: Surgery, Surgeon,
Date, Intra-Op complications
• Hospital course by systems, including:
• Cardiac
• Respiratory
• Fluid, Electrolyte, Nutrition/GI
• Neuro
• Genetics
• Scheduled Medications
• Access/Vascular
• Consultations
• Social: Language, Support, Concerns
P – Patient Summary

The specific action items you are
handing off to the person taking over
care of your patient.
• What needs to be done?
• When to do it/What time?
• What to do about it?
• Pending results/studies to follow up
A – Action List

S - Situation Awareness & Contingency Planning
• Provides the receiver with specific instructions
for what might go wrong
• List interventions that HAVE/HAVE NOT worked
• Contingency Planning - Problem solving before
things go wrong:
• “If this happens, then…”
• Provides the receiver with specific instructions for
what might go wrong
• Ensures accepting team is prepared to anticipate
changes in patient status and respond accordingly
• Identify resources and chain of command
• For stable patients:
“I don’t anticipate that anything will go wrong.”

• Receiver should allow the person giving handoff to
get through the first 4 elements (IPAS) first without
interruptions.
• Opportunity for the receiver to ask questions, clarify
and then synthesize what they heard
• Brief re-statement/summary of essential information and
written documentation
• Demonstrates information is received and understood
• Receiver may synthesize the facts differently
• Keeps the receiver more engaged
S – Synthesis
By closing the loop, we solidify the shared
mental model we are trying to establish.

Synthesis – Receive and Read/Repeat Back

Documentation of Synthesis
• Documentation of Synthesis consists of:
1. The receiver’s notes from verbal handoff
2. EPIC documentation
• The receiver reads back their written notes taken
during report
• Report giver and receiver review EPIC
documentation and indicate IPASS given.
• These supplement the verbal handoff
• Helps receiver to follow report
• Facilitates active participation by receiver
• Provides more comprehensive & efficient
information transfer

I-PASS Examples

I-PASS Example 1
Simple Admission

I-PASS Example 2
Complex Admission

Pediatric Provider Example

I =
Illness severity
Patient is stable
P =
Patient summary
7 day old male dosing weight 3 kg full code no allergies
Dx: HLHS
MA/AA s/p Norwood BT Shunt POD 1 by Dr. McKenzie. Can follow
with a review by systems (CV,
Resp, Neuro, Gi/GU, Heme etc.)
A =
Action list
The patient’s MAP has been elevated, so
Nipride was increased. You
need a new syringe and I put a Pharmacy request in at 0545. You have
an ABG due at 0700 for a vent change I made at 0630. The
foley was
removed at 0500 and you are due to void.
S =
Situation
Awareness &
Contingency Plan
If the
Nipride doesn’t arrive in 30 minutes, then call the pharmacist.
If there is no urine output by 1100, then the patient will need to be
straight
cathed
S =
Synthesis
You said the BP was elevated but what are our goals? Is the order up
to date?
What vent change was made at 0630?
Ok
I will notify the MD if I have no urine output by 1100 and obtain
my ABG at 0700.
RN Example – Pediatric 1

RN Example – Pediatric 2
I =
Illness severity
Anthony is a 14 year old, stable patient with history of sickle cell
P =
Patient summary
He is here with chest pain for three days. Denies fever or shortness of
breath. We have drawn labs drawn, given a 20ml/kg NS bolus, and
administered three doses of Morphine 4mg. The last dose was at
1200.
A =
Action list
Anthony is waiting on x
-ray, and MIFV to come from Pharmacy
S =
Situation
Awareness &
Contingency Plan
He is complaining of pain 8/10, and can be remediated in one hour. If
his pain is not controlled with the next does he will be admitted.
Mom is at the bedside and has been updated with the plan of care.
S =
Synthesis
4 year old, stable sickle cell patient here with chest pain. Denies fever
or SOB. Waiting on x
-ray, MIVF, and can be medicated for pain now.
RN 1
Correction, he cannot have another dose of morphine for one hour.
RN2
Ok,
thank you for correcting me.

RN Example – Obstetric 1
I =
Illness
severity
Ms. Smith is a stable female
P =
Patient
summary
35 year old admitted yesterday around 1pm, G3P2 at 33. 4 weeks gestation with placenta
previa
presenting with bright red vaginal bleeding, not in active labor.
During the day & the overnight shift, she had no vaginal bleeding. An ultrasound was
completed and admission labs were drawn. Labs and ultrasound came back normal.
Dr. Wilson is planning to watch her for now. She will be a repeat C
-
section, anesthesia and
neonatology has been notified.
She received betamethasone 12 mg IM yesterday at 3pm, with her second dose due this
afternoon.
Fetal heart rate has been a category 2, positive for accelerations with little to no uterine
contractions on the monitor or by palpation.
She has no complaint of fluid leaking or additional bleeding. She is awake and alert with
no complaint of pain at this time.
She remains afebrile and her GBS came back negative. Respirations and pulse are within
normal range, clear lungs on auscultation. Her blood pressures are normal as well, ranging
from 125/76 to 110/62.
Her hemoglobin did drop this morning from 12.1 to 9.9. Her abdomen remains soft and
non
-tender. She has been on clear liquids since yesterday with LR infusing at 125ml/hr.
Access is an 18G IV to her left forearm infusing LR. Her blood type is A+.
No bowel movement overnight, and her last void was at 6:45am
The father of the baby went home last night on his way back now.

RN Example – Obstetric 1 continued
A =
Action list
No new orders have been received. Follow up on additional labs, continue LR, and
consider requesting a normal diet if no bleeding noted.
S=
Situation
Awareness &
Contingency
Plan
If the bright red bleeding comes back, notify the physician, Neonatology Team,
Anesthesia, and Labor & Delivery Charge Nurse. Prep for C
-section, and type and
cross II units.
S =
Synthesis
Ok
, so Ms. Smith is a stable 35 year old female, G3P2
33. 4 weeks gestation admitted
yesterday with placenta
previa presenting with bright red vaginal bleeding, not in
active labor.
She’s had no additional vaginal bleeding. Labs and ultrasound came back normal. I
will follow up on additional
labs.and request normal diet if no bleeding.
Her last dose
of betamethasone is due this afternoon. What time?
Fetal heart rate has been a category 2, positive for accelerations with little to no
uterine contractions on the monitor or by palpation.
Her hemoglobin dropped from 12.1 to 9.9.
I
f the bright red bleeding comes back, I will notify the physician, Neonatology Team,
Anesthesia, and Labor & Delivery Charge Nurse. Prep for C
-section, and type and
cross II units.

RN Example – Obstetric 2
Listen to this OB report and identify what
I-PASS element is missing…
(Click on the speaker to listen and then click to see if you correctly
identified what is missing.)
There was no synthesis by the report receiver at the end.
How would you synthesize this report?

Respiratory Example
I =
Illness severity
Stable; Full Code
P =
Patient summary
29 week old male born this shift at 13:09. Placed on BCPAP +8, 40% in
delivery room. Intubated an hour after delivery, then given CUROSURF®
at 15:30 due to decreasing
sats. Sats improved post CUROSURF®.
Current weight is 1.375 kg. Chest X
-ray taken after intubation. Patient is
intubated with a 3.0 taped at 7.25 cm at the lip. Current vent settings:
AC/VG 40,
Vt 6.9, +6, 0.35, pmax 25, FIO2 30-35%.
A =
Action list
Second CUROSURF® due at 03:30. If CUROSURF® is not in the drawer at
03:00, call the pharmacy. Continue to wean the FIO2 as tolerated. Try
weaning the
Vt down to 4 – 4.5 mL/kg to begin meeting extubation
criteria.
S =
Situation
Awareness &
Contingency Plan
If the patient continues to do well after the second dose of CUROSURF®,
ask the team about
extubation. If the tabs of the neobar
start to rise up
slightly, replace the
neobar.
S =
Synthesis
How low were the
sats and how high was the FIO2 before the dose of
CUROSURF® was given? Have you tried weaning the FIO2 below 30%?
Is the patient breathing over the vent? To summarize, patient is a 29
weeker
, born today. Next CUROSURF® is due at 03:30. I will talk to the
team about weaning and possibly extubating.

Social Work Example
I =
Illness severity
Unstable
P =
Patient summary
Jane Doe: DOB… MRN …. Pt is a 5 month old who was admitted for prematurity, she has
other diagnosis due to prematurity. Pt was exposed to illicit substances in utero. CPS is in
the process of taking custody because of the following reasons: positive drug screen,
parent’s behavior at bedside which includes hindering care and threatening staff, lack of
comprehension of
pt’s dx and plan of care etc. Parents are NOT allowed at bedside. All
medical interventions have been on hold because parents do not want to give consent for
any medical intervention recommended by the team. The medical team is waiting for CPS
to get custody so they can move forward with the treatment plan (trach and g
-tube
placement). Custody hearing is scheduled for today at 3pm.
A =
Action list
CPS will contact SW via page operator when they get custody of the baby. Inform the team
once you confirm CPS has custody so they can obtain consent for surgery. Please place a
copy of the paperwork in the paper chart at bedside.
S =
Situation
Awareness &
Contingency Plan
If you do not hear from CPS, Please call and inquire the status of case.
S =
Synthesis
NICU patient who is critically ill. CPS is involved and is in the process of getting custody. CPS
will contact SW once custody is granted. Once I receive confirmation, I will communicate
with the team. If I don’t hear anything, then I will call the CPS worker for update.

• Shift-to-shift hand-offs
• Transfer of care from one unit/clinical area to
another or to another facility
• SBAR will still be used for concerns or
escalations
• SBAR will remain available in EPIC in same
location – now below IPASS
When Will I-PASS Be Used?

Patient Experience Reminders
• Report still needs to occur at the bedside.
• Always start by introducing yourself to
patient & family when entering the room.
• Update the whiteboard as a reference point
for the patient and family.
• Before leaving the room after report, ask
the patient and family what questions or
concerns they have regarding the plan of
care.

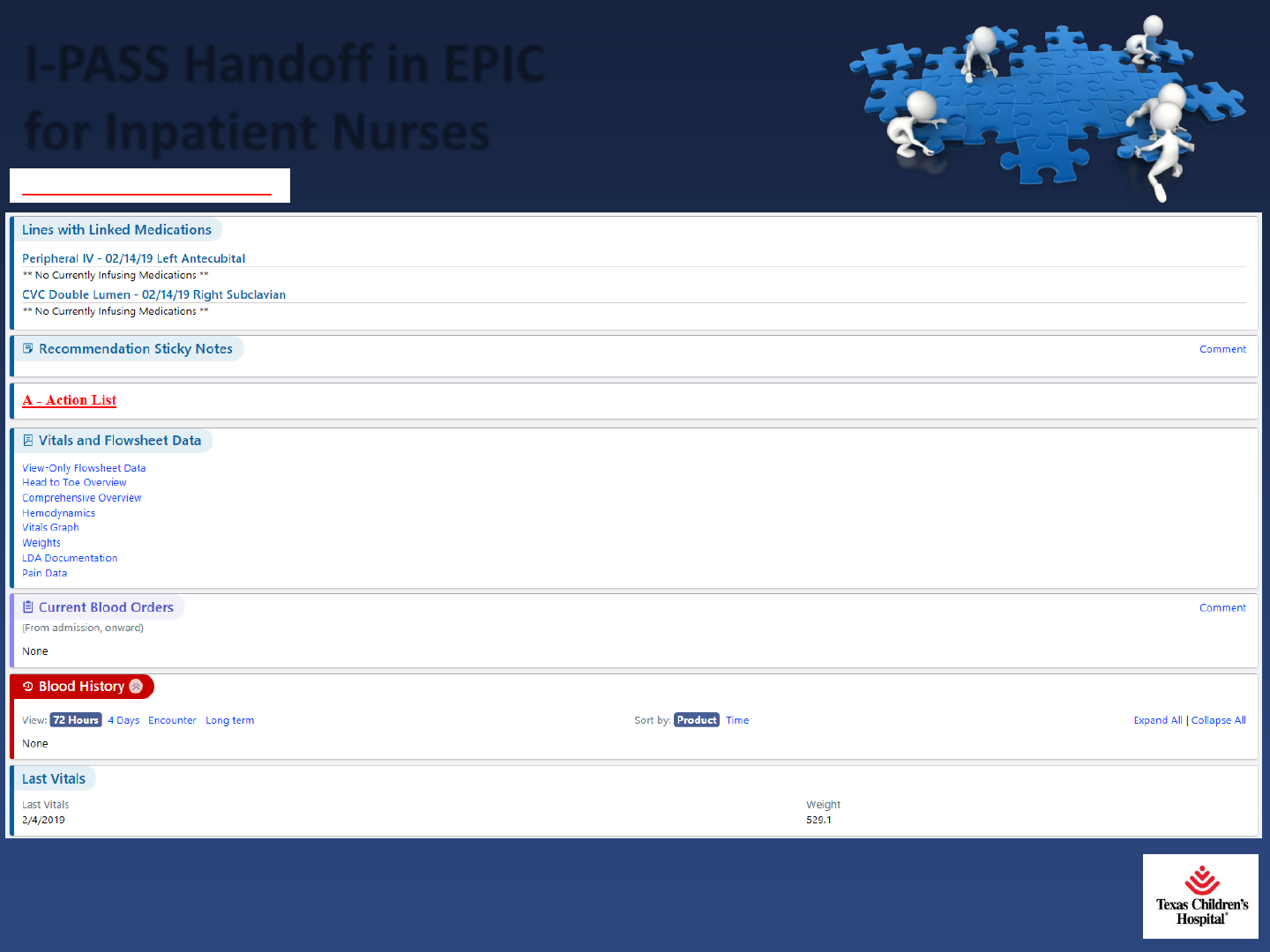
I-PASS Handoff in EPIC for
Inpatient Nurses
Note: I-PASS screen will be located in
a different location for Outpatient.

I-PASS Handoff in EPIC
for Inpatient Nurses
P - Patient Summary (continued)
I-PASS Handoff in EPIC
for Inpatient Nurses
P - Patient Summary (continued)

I-PASS Handoff in EPIC
for Inpatient Nurses
Note: SBAR is still available to document
escalations and concerns.

I-PASS
Implementation Timeline
January-February
2019
•Collaborate with
interprofessional
stakeholders
•Finalize training
plan
•EPIC modifications
February-April
2019
• Launch pre-survey
and e-learning
course
• Peer Assessments
• 100% - reports
logged in
HealthStream
• Monitor plan
May 2019
• Appraisers
conduct unit-
level audits
• 25% - reports
to be placed on
I-PASS webpage
• Stakeholder
feedback
June 2019
I-PASS
GO
LIVE!


I-PASS Peer Assessments
Following completion of this online course,
clinicians will be required to demonstrate use
of the I-PASS format while communicating
report/handoff of patient care.
• Validations will be captured through a web-based I-
PASS Peer Assessment Tool in REDcap.
• A QR code on the badge cards goes to the I-PASS
Resources website where there is a link to the
“I-PASS Peer Assessment Tool” in REDcap.

I-PASS Peer Assessments
Encourage and hold peers accountable to complete all elements of I-PASS. Some
elements may need to be repeated before you feel confident indicating it was
observed. Please let educator know if peer needs additional remediation.
Clinician receiving report opens REDCap by clicking on link to “I-PASS Peer
Assessment Tool” from the I-PASS Resources website. A QR Code to the I-PASS
Resources website will be available on the badge cards.
Employee ID # for person reporting handoff entered & clinician receiving report
indicates that he/she observed clinician giving report using I, P, A & S.
Both clinicians agree & attest that “Synthesis” was effectively completed.

Peer Assessment Tool in REDCap

References
The Joint Commission. (2017) Sentinel Event Alert. Retrieved
from https://ipassinstitute.com/2017/09/13/joint-
commission-releases-sentinel-event-alert-related-handoff-
communication/
The IPASS Patient Safety Institute. (2019). The IPASS Handoff
Program. Retrieved from
https://ipassinstitute.com/evidence/
Starmer, A. J., Spector, N. D., Srivastava, R., Allen, A. D.,
Landrigan, C. P., & Sectish, T. C. (2012). I-PASS, a mnemonic
to standardize verbal handoffs. Pediatrics, 129, 201-204.

Thank you!
