
Medicaid Expansion in Missouri - Economic
Implications for Missouri and Interviews
Reflecting Arkansas, Indiana, and Ohio
Experiences
R
ELEASED BY MISSOURI NURSES ASSOCIATION, MISSOURI ASSOCIATION OF
RURAL HEALTH CLINICS, MISSOURI EMERGENCY MEDICAL SERVICES
ASSOCIATION, MISSOURI AMBULANCE ASSOCIATION,
A
MBULANCE DISTRICT ASSOCIATION OF MISSOURI,
M
ISSOURI RURAL HEALTH ASSOCIATION, MISSOURI PRIMARY CARE
ASSOCIATION, MISSOURI HOSPITAL ASSOCIATION, GREENE COUNTY
MEDICAL SOCIETY, MISSOURI CHAPTER, AMERICAN ACADEMY OF
PEDIATRICS
B
Y
M
ATT POWERS
S
HARON SILOW-CARROLL
J
ACK
M
EYER

Health Management Associates 1
Executive Summary
Health Management Associates (HMA) conducted a targeted analysis of the economic impact of an ACA
Medicaid Expansion in Missouri, with an emphasis on the effects on the state budget. As Missouri
considers the costs and benefits of adopting the ACA Medicaid Expansion, state officials and private sector
leaders should consider the experience of other similarly situated states that have implemented
Expansion in the past few years. HMA examined the literature on states’ experience with Medicaid
Expansions, and took a deeper look at three largely Republican states that had robust discussions about
the potential impact of an Expansion prior to its implementation — Ohio, Indiana, and Arkansas. We
interviewed leaders with first-hand experience in those states and asked them to reflect upon what did
and did not work in their state.
Both our review of carefully conducted research studies and our interviews with state leaders from nearby
states lead to a conclusion that the full cost of a well-designed and well-synchronized program in Missouri
can be covered by the offsets from replacing state-only funding with a 90 percent federal match, current
Medicaid programs that would be matched at higher rate, and other policy and operational adjustments.
When considering the multiple policy and budgetary implications of Medicaid Expansion, states are wise
to proceed both strategically and cautiously. Synchronizing an Expansion with the appropriate policy and
operational adjustments is imperative to designing a cost-effective program that ultimately reflects the
goals, vision and priorities of the state. An Expansion program in Missouri can be designed to budget for
savings and revenue opportunities that significantly exceed the state’s cost of implementation. An
Expansion can be designed to free general revenue funds for other priorities, such as K-12 education,
transportation, and law enforcement. Our report’s key findings are:
General Findings
No State has Reversed its Expansion Decision. Despite significant initial concerns in the states
interviewed for this report, as well as other Expansion states, no state has reversed its decision to adopt
the Medicaid Expansion in the more than six years since this program was first authorized on a national
scale. In fact, additional states continue to choose the Expansion option. More importantly, no state has
reversed its decision because of “out of control” costs. It is far more likely that states regard the Expansion
as having a positive impact on the state’s general revenue budget.
Arkansas, Indiana, and Ohio Expansion Costs Have Been Controlled. Each state meticulously worked to
customize its program to keep costs under control and to capture state dollars that were then used to
fund the state’s share of the Expansion.
Costs and Offsets
Costs
Confirming Reasonable Cost and Enrollment Estimates. Although there are costs to the state for the
required ten percent match, these costs can be offset through a variety of mechanisms, as demonstrated
by the experience of other states that synchronized program changes and revenue matching initiatives as
part of the Expansion design. After a thorough review of data, our research and estimates are in line with

Health Management Associates 2
the enrollment and cost assumptions from the May 2019 Missouri State Auditor’s Office Fiscal Note. The
estimated costs of Expansion would include the State’s 10 percent share of the new program costs, new
administrative costs, and the “woodwork effect,” which results when the Expansion enrollment process
draws in people previously eligible for Medicaid but not participating.
Offsets
Expansion Benefits the Mental Health, Substance Use Disorders, and Incarcerated Populations. Large
state-only outlays could be used to draw down a 90% federal match. Not only are matching funds
available for populations currently served with state-only outlays, funding opportunities expand for opioid
and addiction prevention programs. Federal money also becomes available to help combat recidivism for
incarcerated populations.
Subsets of the Medicaid Population Will be Positively Affected. Pregnant women, women eligible for the
Breast and Cervical Cancer program, the Medically Needy, and individuals with disabilities will potentially
move from a lower matching Medicaid eligibility category to the higher matching rate available through
Expansion. This creates direct financial benefits for the state.
Revenue opportunities
Provider Taxes Offer Additional Offset Opportunities. A potential Managed Care Organization (MCO) tax
and the option to re-visit other provider taxes present opportunities to offset the costs of Expansion.
State Sales Tax Will Grow. Missouri could expect an increase in sales taxes as a result of the Medicaid
Expansion, as other states have experienced.
Other State Economic Benefits
Gains in Employment Are Expected. Experience from other Expansion states demonstrates that
Expansion has had a positive impact on people’s ability to seek work, obtain jobs, and engage in volunteer
work.
The Health Care Infrastructure Will be Enhanced. Improvements in the health care delivery system and
quality of care are likely to occur. A reduction in uncompensated care can be expected as well.
Lessons from HMA Interviews with Arkansas, Indiana and Ohio
HMA conducted in-depth interviews with leaders directly involved in the Medicaid Expansions in Ohio,
Arkansas, and Indiana. Lessons learned included:
Leverage the flow of new federal money to implement reforms to Missouri’s health care delivery
and payment systems, potentially as part of a more systemic transformation initiative
Keep financing straightforward, building on existing mechanisms when possible
Recognize that some costs will be incurred up front while the full effect of the offsets and other
benefits may take some time to emerge
A number of policy accomplishments were achieved as these states rolled out their Medicaid
Expansions. For example, Arkansas simultaneously enacted a state income tax cut during the
Medicaid Expansion implementation.

Health Management Associates 3
Compelling messages from the interviews include: newly eligible people include veterans and
“people we know”; Expansion reduces cost-shifting and loss of federal tax dollars to other states;
Expansion data shows better outcomes for enrollees with substance use disorders and mental
illness; consumer education is important; and if you run a responsible program that helps people,
the majority of state residents will support it.

Health Management Associates 4
Introduction
This paper examines the most common concerns expressed about the potential negative effects of
Medicaid Expansion in Missouri, and in other states, with a focus on the financial and budgetary impact.
Section 1 estimates the cost of Expansion in Missouri and identifies cost offsets and other sources of state
savings. These calculations are based on a large body of research evidence as well as the experiences of
states that have adopted the Medicaid Expansion.
A key focus of the paper is to explain state budget savings and financial opportunities created by the
Expansion and identify the proven strategies used by other states to offset the state’s required 10-percent
share as well as other Expansion-related administrative costs. These offsets include reductions in non-
Medicaid state spending on mental health and substance use disorder services and on health services
provided to people who are incarcerated because they gain access to coverage through the Expansion. In
addition, there will likely be savings resulting from access to additional treatment options covered under
Expansion to address the opioid crisis, reduced uncompensated care outlays, and reductions in spending
for existing state programs. Ninety percent of state-only dollars used to fund these critical services would
be replaced by federal dollars, freeing up general revenue funds for other priorities, such as K-12
education, transportation, and law enforcement.
Section 2 of this paper examines the experience of three states - Ohio, Indiana, and Arkansas - with
government leadership largely in Republican hands, that have implemented Medicaid Expansion and that
have multiple years of experience with the program expansion. We conducted in-depth interviews with
key leaders and experts with direct knowledge of the impact of the Medicaid Expansion in these
comparison states and examined:
Key stakeholders’ perceptions of some of the most prominent concerns expressed by opponents
of the Expansion
Strategies used to address these concerns
The consequences of Expansion
Our report identifies multiple policy options that were concurrently enacted with Expansions in other
states to support the states’ share of the cost of Expansion. State policymakers frequently find themselves
in difficult situations, presented with options that “save” money on the back end with significant
investment on the front end. We attempt to provide a balanced, fact-based set of assumptions designed
to inform decision-makers and the general public and foster constructive dialogue as they consider this
important policy step. If our assumptions can be improved as new or more refined data emerges, this new
information can further inform the decision-making process.

Health Management Associates 5
Section 1: Financial Analysis
The Economic Impact of Medicaid Expansion in Missouri.
Background
The Affordable Care Act (ACA), passed in 2010, and later modified through a June 2012 U.S. Supreme
Court ruling, made Medicaid Expansion optional for states. At this point in time, 37 states have adopted
the Expansion. Non-Expansion states include southern states such as Florida, Georgia, Mississippi and
Texas, and several states in the central United States, including Missouri. Multiple Non-Expansion states
are actively considering expansion proposals at the time of this writing.
Medicaid currently enrolls about 75 million people nationwide. The program features comprehensive
health benefits, and a wide range of social support services. Traditional populations served include low-
income parents and their children, pregnant women, the elderly, and individuals with disabilities. States
not adopting the Medicaid Expansion have widely varying income limits for parents’ eligibility, ranging
from 17 percent to 100 percent of the FPL. Most states did not cover adults without dependent children
prior to the ACA, and this population remains ineligible for Medicaid in states that have not adopted the
Medicaid Expansion. Parents with incomes below 100 percent of the FPL (which is $25,750 for a family of
four) and above the eligibility limit, which in Missouri is 19 percent of the FPL or $4,893,
1
as well as adults
without dependent children, are in what is called the “coverage gap”. This means that their incomes are
too low to obtain subsidized health coverage through the ACA Marketplaces, but too high to qualify for
Medicaid under their states’ eligibility limit. Individuals not otherwise eligible for Medicaid (e.g., those
with disabilities, pregnant women) are currently ineligible for both Medicaid and the Marketplace. To put
this in perspective, a worker with a family of four who earns the Missouri minimum wage of $9.45 an hour
and works half-time (20 hours a week) for a full year (50 weeks) earns $9,450, well above the eligibility
threshold for this adult to enroll in Medicaid. Even if that worker had a full-time job at 40 hours a week,
he or she would still be ineligible for Marketplace premium and cost-sharing subsidies.
Nationally, approximately 69% of Medicaid beneficiaries are enrolled in in risk-based managed care
organizations (MCOs) that provide care management and receive “capitation rates”; in turn the MCOs are
held accountable for risk and the cost of health care. Medicaid payments to hospitals, physicians and
other providers are typically substantially less than Medicare payment rates and even further below
commercial insurance payment rates. This is particularly magnified after provider taxes are netted out of
the equation.
Because of its significant budget and large scope of coverage, Medicaid impacts the state economy, the
state budget, the job market, other insurance carriers, most health care providers, and the state’s most
vulnerable residents. Of Missouri’s population of 6.2 million, Medicaid insures just over 800,000
individuals at a total annual cost of just over $10 billion in 2019.
2
About two-thirds of this $10 billion is
paid by the federal government through Federal matching funds using the Federal Medical Assistance
Percentage (FMAP) used to determine the amount of the match. The other one-third is, in terms of gross
dollars, paid by the state. A substantial proportion of that gross state share, however, is offset by provider

Health Management Associates 6
taxes such as the hospital tax, bringing the net Missouri share of the total cost to a much lower level of
state funding.
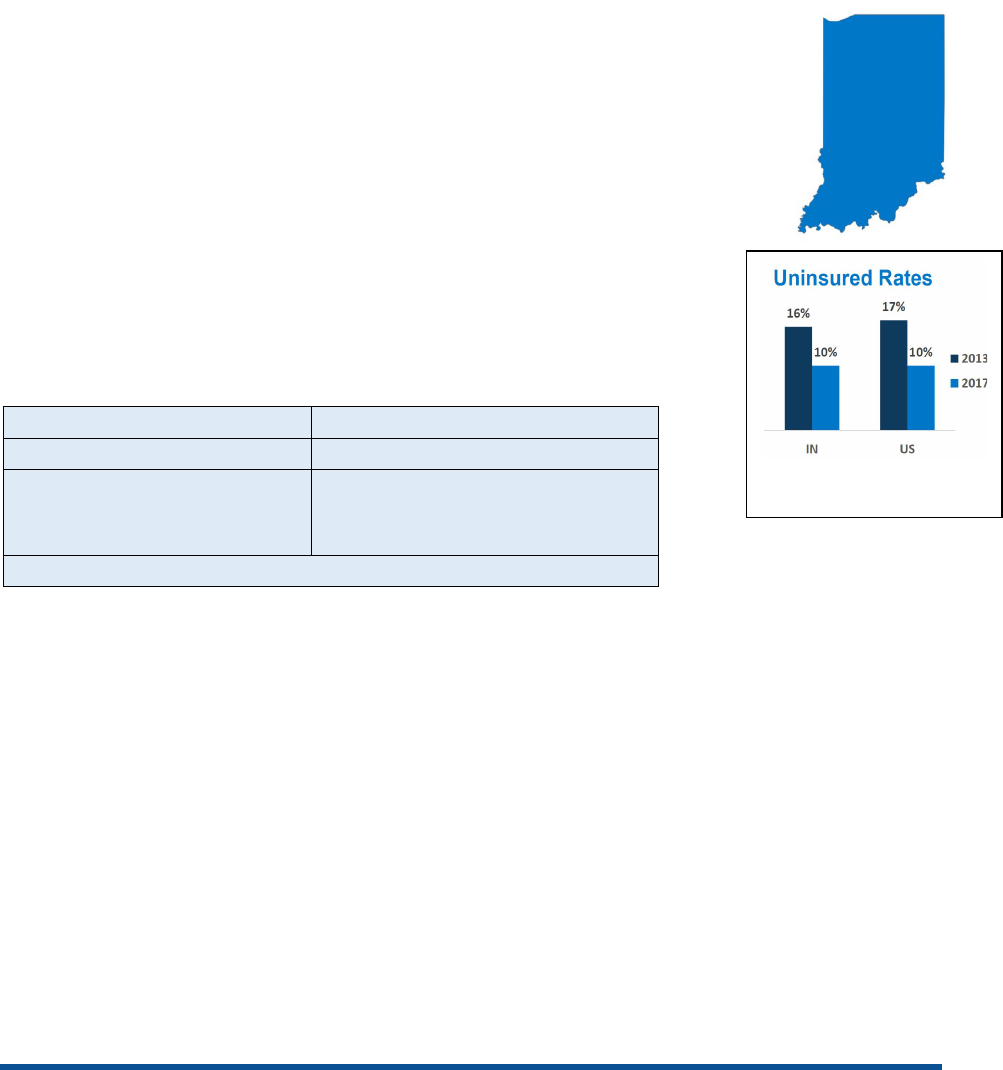
While Medicaid has a very large presence in Missouri, and all states, Figure 1 illustrates the importance of
other payers. Half of Missouri residents have employer-sponsored coverage, including Missouri state
employees. One in five insured Missourians are enrolled in Medicare, including some individuals who are
also enrolled in Medicaid (the dual eligible population). It is noteworthy that Missouri’s unemployment
rate in October 2019 was one of the lowest in the nation at 3.1 percent, and the workforce participation
was 65.1 percent.
3
This affects insurance coverage opportunities across the board. None the less,
Missouri’s rate of uninsured citizens of 9.4% is higher than the national average. Thirty-three states have
uninsured rates lower than Missouri.
4
Figure 1: Missouri Health Insurance Coverage (2018)
5
Note: Percent covered by Medicare was rounded up to 17 percent for total coverage to equal 100 percent.
Costs Related to Medicaid Expansion
States face many pressures and challenges when attempting to balance their budgets. Unlike the federal
government, states cannot use deficit financing to cover current obligations. Many states are
appropriately wary of new financial commitments, particularly if they are long-term commitments. When
states consider a substantial program expansion, especially one that includes entitlement provisions such
as Medicaid, state policymakers have an obligation to consider the risks and benefits carefully.
States must also consider the timing of costs and savings. Among states that have adopted Medicaid
Expansion, the costs related for the state’s share of benefit payments starts immediately when enrollment
begins, and the administrative costs are “front-loaded” to fund needed staff and IT systems. As a result,
the costs in the first year, and perhaps to a lesser extent in the second year, may not be fully offset by the
early savings. Over time, however, Expansion states have realized numerous offsets and savings that
exceed the program costs, as described further below.
Employer
52%
Medicaid
15%
Medicare
17%
Individual
6%
Military
1%
Uninsured
9%

Health Management Associates 7
Estimating Changes in Medicaid Enrollment
Based on the May 2019 Missouri State Auditor’s Office Fiscal Note, approximately 250,000 Missourians
could be potentially covered if the state expands Medicaid. Washington University projects a total eligible
count of 271,500. Table 1 displays the number newly eligible through Expansion, whose costs would be
matched at 90 percent by the federal government, and those newly identified as eligible for traditional
Medicaid during Expansion enrollment, the “woodwork” eligible (whose costs would be matched at
Missouri’s Medicaid matching rate of 65 percent). Table 1 estimates the size of the populations affected
by the Expansion. These numbers would likely take several years to reach.
Table 1: Estimated Expansion Population
(includes minor HMA interpretation)
6
Population Category
Washington University
Estimates
Uninsured Adults (19-64)
139,000
Adults (19-64) with Individually Purchased Private Insurance
72,000
Adults (19-64) with Employer Sponsored Insurance (ESI) Coverage
20,000
Total Estimated Adults (19-64)
231,000
Uninsured Children (0-18)
20,000
Children (0-18) with Individually Purchased Private Insurance through Parents
13,500
Children (0-18) with Employer Sponsored Insurance (ESI) through Parents
7,000
Total Estimated Children (0-18), “Woodwork Children”
40,500
ACA 90% Match Population (Total Adult Population Less “Woodwork Adults”)
190,500
ACA 65% Match Population (“Woodwork Children” Plus “Woodwork Adults”)
81,000
Total Expansion Population
271,500
The “Woodwork Effect”
In other states that implemented Expansion, some uninsured individuals who were already eligible for
traditional Medicaid came “out of the woodwork” to enroll, likely as a result of the public awareness
created by the Expansion. An estimated 81,000 uninsured children and adults in Missouri are already
eligible for Medicaid under existing eligibility categories but not enrolled. Newly eligible Missourians
would include primarily parents with income above the current limit and childless adults with income up
to 138 percent of the FPL (or $17,236 for an individual and $35,535 for a family of four annually).
Estimating Changes in Medicaid Costs
According to national studies, Medicaid Expansions did not lead to significant increases in spending from
state funds. Solid research has also shown that there were no significant reductions in state spending on
education, transportation, or other state programs as a result of the Medicaid Expansion during a five-
year period. Single-state studies, discussed below, in Louisiana, Kentucky, Arkansas, Michigan, and
Montana have shown that the Medicaid Expansions resulted in significant state savings.
7
Of course, each
state is different and national studies need to be looked at carefully with respect to the application to
individual states. Below we discuss how our interviewees responded to these legitimate concerns. It is
also critical to explore state costs and to carefully consider an Expansion with all variables clearly identified
– both costs and benefits. Some of the savings resulting from state-only programs discussed below (e.g.
mental health, substance abuse) will phase-in over time, given the operational issues involving eligibility,
state appropriations, and moving from state-only resources to Medicaid matched resources.
Health Management Associates 8
With respect specifically to Missouri, the main costs of a Medicaid Expansion are explained below and
summarized in Table 2.
Table 2: ACA State-Only Expansion Costs in Missouri
(HMA analysis)
Category
Cost
State Share for Full Participation (10%) $97 million
State Share for Woodwork Effect (35%) $94 million
State Share Administrative Costs
$10 million
TOTAL State-Only Expansion Costs
$201 million
Ongoing State Share of Medicaid Expansion
Effective this year (2020), federal law requires that states fund 10 percent of the cost of the Medicaid
Expansion population. In Missouri, the state share is estimated to cost $97 million in 2020. The Missouri
Auditor and Washington University report similar total enrollment and expenditure costs. We believe the
estimates for both the newly eligible and the “woodwork effect” populations to be realistic and they
certainly do not understate costs.
“Woodwork Effect” Costs
New enrollment in the traditional program resulting from the “woodwork effect” is estimated to cost
Missouri $94 million for the state share applying the state’s Medicaid FMAP of 65.65 percent.
New Administrative Costs
Significant resources will be required to implement a Medicaid Expansion. These would include additional
resources for eligibility/adjudication, provider education (particularly education for behavioral health and
substance abuse providers regarding billing issues and transition from state-only resources), Medicaid
Management Information System (MMIS) programming, and other administrative expenditures.
The Missouri State Auditor’s Fiscal Note on the Medicaid Expansion projects that the Missouri Family
Support Division will need fifty-six Eligibility Specialists, six Eligibility Supervisors, and one Social Services
Manager to assist in enrolling new participants at an estimated cost of $4.6 million. The Family Support
Division also estimates an increased cost of $9.1 million for additional staffing of the call center to answer
eligibility questions. Another $5 million cost is projected for MMIS changes, and MO HealthNet estimates
a needed increase of $4.1 million to fund additional staff for customer support, tracking, and claims data
reporting.
8
Using a conservative approach, we estimate a cost of $10 million for the state share. The
combination of state and federal matching funds would provide over $20 million in funding. Some of
these costs would be one time (non-recurring) costs. To put this in perspective, an additional 100 FTEs
could be supported within this estimate.
Crowd-Out
Crowd-Out refers to a process in which an expansion of public coverage displaces, or “crowds out” private
health insurance. Our analysis suggests that crowd out under a Medicaid Expansion would have a
relatively small impact over time. The Washington University study concluded that: “According to Kaiser
Family Foundation, studies exploring the potential for Medicaid Expansion to crowd out private insurance
have found mixed results, with most showing no evidence of crowd out and some showing slight declines

Health Management Associates 9
in private coverage in Expansion states following Expansion.”
9
Crowd-out is a more serious issue for
coverage programs targeting population with substantially higher income levels, as can occur in the
Children’s Health Insurance (CHIP) program, where some states increased their CHIP eligibility levels
above the original 200 percent of the FPL threshold.
It is also important to note that Medicaid enrollment nationwide declined in 2018 and 2019. While certain
states and certain studies may show different experiences, overall enrollments have not been surprises
to states in recent years and states project less than one percent growth in 2020 nationally.
CMS Flexibility
Our state-based interviews identified considerable evidence that CMS and states have created customized
Expansion programs that feature flexibility – particularly when CMS authorizes the use of waivers. We
discuss state experience in Section 2 of this report.
Economic Benefits Related to Medicaid Expansion
The evidence shows that a large part, if not perhaps all, of the cost of the Expansion would be offset by
multiple sources of state budget savings and revenue enhancement options unrelated to any traditional
tax increase.
Louisiana reported extensively on a variety of economic benefits, including local government savings,
benefits to the state’s economy related to the infusion of federal dollars, and the restructuring of
programs resulting from fewer people being uninsured. Other states had a similar experience, deriving
savings from Expansion, including Virginia (which saved $421.6 million in the first year of Expansion)
10
,
Arkansas ($444 million total from 2018-2021)
11
, Michigan ($1 billion from 2018-2021)
12
, and Montana
(over $50 million).
13
Nebraska projects savings of $360 million over five years and a reduction of 4.3
percent annually in Medicaid outlays under a Medicaid Expansion that will add 94,000 people to Medicaid
on October 1, 2020.
14
These sizeable savings are both important and instructive. One cautionary note is that some of the state
experiences cited here occurred over the time period in which the federal match under the Medicaid
Expansion was higher than the 90 percent match that took effect on January 1, 2020. Yet, the offsets
noted above are real, measurable, and have been validated by the states in question.
We will focus on two items that are available to fund and/or offset costs of the Medicaid Expansion –
funding from existing state programs that do not receive federal match currently and revenue
opportunities that other states have coordinated with an Expansion. We will first explain the policy
approaches and then calculate estimates for Missouri.
State Savings and Revenue Opportunities
Most states historically covered the costs for the majority of mental health and substance abuse services,
as well as health care services for justice-related populations, solely from state and local resources and
federal grants. Over the years, and with the increased need for mental health and substance abuse
programs and support, these state-only resources have become quite substantial. Almost all of the
individuals served in these programs will become Medicaid eligible under Expansion. As a result, there are

Health Management Associates 10
opportunities to pay for certain benefits previously funded solely from state funds through Expansion
funding which will be matched at the federal matching rate of 90 percent. We have not itemized the
savings and revenue opportunities in this report because we do not have access to the extensive data we
would need to reflect that amount of detail. We can say, however, that based upon other states’
experiences and our own experiences, we fully expect that an Expansion program in Missouri can be
designed that leverages savings and revenue opportunities and significantly exceeds the state’s costs for
the Expansion. For states facing significant budget pressures, this Medicaid Expansion funding source can
provide substantial and lasting savings as described below:
Medicaid Spenddown. People in the Medically Needy or “Spenddown” population are incurring
large medical bills that will eventually qualify them for Medicaid through the “spenddown
window.” Many of these people with high out-of-pocket costs will ultimately lower their incomes
to qualifying levels, where the state would receive the traditional federal match. The Center for
Health Economics and Policy at Washington University projects savings of $17.4 million in 2020
as a portion of this population enters Medicaid through the Expansion and Missouri would receive
the 90 percent match.
15
Disabled. A portion of people with disabilities who applied for Supplemental Security Income
(SSI) have not yet met the SSI disability standard (47 percent of applicants in Missouri) and in
addition some people with disabilities elect not to apply for SSI through seeking disability status.
A portion of these groups would enter Medicaid through the Expansion. Many would have
eventually entered Medicaid through SSI, but with a standard federal match rate. Savings to
Missouri from enrolling these people in the Expansion have been estimated at $55 million in
2020.
16
Medicaid for Pregnant Women Living in Poverty. An estimated 94 percent of this population
(19,000 women) would be eligible to be rolled into the Medicaid Expansion, allowing Missouri to
obtain the higher federal match for this population and to provide uninterrupted health care
coverage.
17
Opioid Epidemic. With overdoses now the leading cause of death for Americans under 50 years
old, finding both prevention and treatment solutions for addiction is a huge priority for states.
Medicaid Expansion allows the state to use 90 percent federal funds to pay for treatment that
would otherwise frequently be funded with state dollars, thus freeing these state funds to go
toward prevention and other state priorities.
Other substance use disorders. In addition to the opioid crisis, states face a growing demand for
treatment and prevention in other areas, including for treatment of alcohol, fentanyl and heroin
addiction.
Mental Health Gaps. Gaps in the mental health systems are frequently cited as an area that both
political parties agree need more resources and fundamental reform. Federal Medicaid expansion
funds can be used for newly covered populations needing a wide range of mental health services
in lieu of limited state dollars.
Cost of care for incarcerated individuals. Medicaid expansion can provide ongoing healthcare
support to individuals transitioning from incarceration. This is critical to ensuring that ongoing
medication and mental health services are immediately available to individuals once they are back

Health Management Associates 11
in the community. Achieving a high federal match for inpatient discharges for this population is a
critical opportunity.
Breast and Cervical Cancer Treatment. State Medicaid programs cover women whom CDC-
affiliated clinics have diagnosed with breast or cervical cancer. Under a Medicaid Expansion, a
state could cover all adults with the 90 percent federal match with incomes under 138 percent of
the FPL, regardless of their diagnosis or where this diagnosis was made. In Missouri, uninsured
women who receive such diagnoses at a Missouri Show Me Healthy Women Project provider are
eligible to enroll in Medicaid and receive services for their disease. If Missouri adopted the
Expansion, the women now in these programs with incomes less than 138 percent of the FPL
could be treated as newly eligible under the Expansion, and Missouri would receive a 90 percent
federal match for them.
Provider Taxes. Many states impose a tax on managed care organizations (MCOs), and this is a
possible financing option for Missouri. Medicaid expansion would increase the potential revenue
derived from an MCO tax as the eligible population enrolled in MCOs would increase, thus
increasing MCO payments. Missouri already has well established provider taxes on hospitals and
pharmacies, and increased provider revenue resulting from a Medicaid expansion will result in
increased state revenues derived from these taxes. In the case of the hospital provider tax, the
state is estimated to receive an additional $30 million in revenue at the current tax rate as a result
of increased payments to hospitals for services provided to expansion patients.
State Sales Tax. Missouri could expect an increase in sales taxes as a result of the Medicaid
Expansion, as other states have experienced. As noted above, the infusion of billions of dollars in
new money from outside the state, enhanced through the “multiplier effect,” will generate a
chain of new spending in the state. While there will be some loss of sales tax, as occurs when
consumers and businesses make online purchases from out-of-state companies, much of the new
spending will be subject to the Missouri sales tax.
The bottom line is that, based upon states experiences and our experiences, we fully expect that an
Expansion program in Missouri could be designed to budget for savings and revenue opportunities that
significantly exceed the state’s costs of the Expansion. It is critical to note that these offset savings do
not occur without considerable organizational and operational adjustments. Many providers who may be
previously accustomed to receiving grants with less complicated billing requirements, will most likely have
to convert to billing for a Medicaid service for a Medicaid beneficiary as well as working with an MCO
billing organization. Lastly, in November 2019, CMS officially proposed a comprehensive regulation on
Medicaid fiscal accountability. The rule addresses a variety of issues including Medicaid supplemental
payments, methods of financing the nonfederal share (including provider taxes and donations), and state
reporting requirements. While this is separate matter relative to Expansion, it is an important variable
that can be managed within the context of an Expansion consideration.
Other State Economic Benefits
Up to this point, we have concentrated on “hard” savings that can be calculated and included in fiscal
notes as part of the state’s budget process. We now turn to other important benefits that are more
indirect but still critical.

Health Management Associates 12
Health Care In-State Investment. As health care providers and insurers receive the new
payments, they can be encouraged to invest in reforms in the delivery and payment systems. This
investment could be directed to promising new approaches to care management for individuals
with complex medical and social needs. As people with multiple chronic illnesses, which
frequently involve both physical and behavioral health conditions, receive better medication
management, receive care from a health home that fosters both clinical and community-based
prevention, and receive follow-up care after an inpatient stay, avoidable ER visits, hospital
admissions, and readmissions will decline. Real-time alerts sent to primary care physicians when
their patients enter the ER, or are admitted to a hospital, can also improve care management. All
of these best practices translate into substantial savings for both public and private payers.
Jobs and Earnings. Several studies found that enrollment in Medicaid Expansion had favorable
effects on an individual’s ability to seek and sustain work, as well as on-job growth, and a growth
in volunteer work.
18
In Louisiana the Expansion funding created and supported 19,195 jobs while
creating and supporting personal earnings of $1.12 billion.
19
In Colorado the infusion of new
federal money associated with the Expansion supported over 31,000 additional jobs in the FY
2015-2016 period.
20
In Ohio, an in-depth statewide survey of Medicaid Expansion enrollees found
that:
o Among employed enrollees in the Expansion population, 83.5 percent said that access
to Medicaid makes it easier to work.
o Among the unemployed enrollees in the Expansion population, 60 percent said that
access to Medicaid makes it easier to look for work.
o Among the Expansion population, the proportion employed rose from 43.2 percent in
2016 to 49.6 percent in 2018.
o Among those employed, 50.9 percent had full-time jobs; 31.9 percent worked between
20 and 35 hours per week.
o Some 49.1 percent said that having access to Medicaid also made it easier to pay for
necessities, including groceries, rent, or mortgage payments, or to pay down debt.
o Just under 30 percent said their financial situation improved after enrolling in Medicaid,
almost four times the proportion who said it got worse (7.7 percent); 61.6 percent said
it was the same.
21

Health Management Associates 13
Section 2: Case Studies
The Impact of Medicaid Expansion in Arkansas, Indiana and Ohio.
The remaining section of this report presents evidence from the experience of states that have adopted
the Medicaid Expansion. Our findings below are based upon HMA’s interviews with state leaders with
direct experience with the Expansions in their states. The literature search is national in scope and the
interviews focus on three states—Ohio, Indiana, and Arkansas.
Introduction
To understand how Missouri may fare under Medicaid Expansion, HMA examined the experience of three
states with government leadership largely in Republican hands that have adopted Expansion—Arkansas,
Indiana, and Ohio. We examined key stakeholders’ perceptions of the most prominent concerns
expressed by Expansion opponents, strategies to address these concerns, actual experience, and lessons
that emerged. We conducted in-depth semi-structured interviews with key leaders and experts with
direct knowledge of how the Medicaid Expansion played out in these comparison states.
Table 3 list interviewees by state.
Table 3: Interviewees by State
State
Interviewees
Arkansas
Ray Hanley, CEO, Arkansas Foundation for Medical Care; former Arkansas
Medicaid Director
Andy Allison, Deputy Director for Strategic Planning, IL Department of Healthcare
and Family Services; former Arkansas Medicaid Director
Indiana
Senator Luke Kenley, former Chairman of the Indiana Senate Appropriations
Committee and State Budget Committee Chairman
Rob Damler, Principal and Consulting Actuary -
Milliman, Inc. (involved in
financial projections and analyses in Indiana and other states)
Joe Moser, former Indiana Medicaid Director; Principal at Health Management
Associates
Ohio
Tim Keen, Senior Advisor to the Ohio Auditor of State; former Director, Ohio
Office of Budget and Management
Greg Moody, Executive in Residence, Ohio State University John Glenn College of
Public Affairs; former Director, Ohio Governor’s Office of Health Transformation
Tracy Plouck, Assistant Clinical Professor, Ohio University; former Director, Ohio
Medicaid Department and former Director, Ohio Department of Mental Health
and Addiction Services

Health Management Associates 14
Arkansas Medicaid Expansion: the “Private Option”
In 2013, with the first Republican legislature in 140 years, then-Governor Mike
Beebe (D) signed the state’s Medicaid Expansion into law. Through an 1115 waiver,
Arkansas accepts federal funds through the Affordable Care Act for eligible low-
income residents to buy private insurance through the state’s Marketplace. The
plan initially included Health Savings Accounts (HSAs), which ended in 2016 after
limited implementation. The state added work requirements that were halted by a
federal court in March 2019. Continuing to fund the expansion requires support
from 75 percent of the legislature every year, which has been achieved since
implementation.
Expansion Implemented
2014
Total Medicaid Enrollment
967,200
Expansion Group Enrollment
Newly Eligible: 318,300
Not Newly Eligible: 10,200
(FY 2017) Source: Kaiser Family Foundation
Key Stakeholders involved in Expansion in Arkansas shared the following lessons about strategies,
expectations, and experience:
Early Concerns and How They Were Addressed
‘Don’t expand a broken system’ - Arkansas engaged in comprehensive provider payment reform in
advance of and in conjunction with Expansion, introducing financial incentives to “fix” the Medicaid
system. Also, supporters led by the Governor and Medicaid Director developed the Private Option that
built on private insurance rather than expanding the existing fee-for-service Medicaid program.
“[Expansion was an opportunity to] rethink who you pay for what, and how to introduce financial
incentives into Medicaid.”-AA
‘It’s too expensive and will divert funds from truly needy people’ - Before the cost concern could get
traction, the administration conducted and released fiscal impact analyses using conservative
assumptions (e.g., inflating national estimates of expected new enrollment) that still projected significant
savings to the state. To help finance the state share, Arkansas used premium taxes, largely on the
Marketplace plans enrolling the Expansion population.
‘It’s Obamacare, it’s socialism’ - After initially offering a traditional Expansion, the Beebe administration
proposed a model with elements that were politically acceptable to most conservatives. The Expansion
involved purchasing private health plans, using HSAs, and work requirements (HSAs later ended as
administrative expenses were too high).
‘It creates dependency among able-bodied people’ - The administration and proponents focused on the
message that the state needs the healthiest workforce it can get. Expansion is not welfare but creates the
ability for people to access primary care and other care to be healthy and able to work.
Key Strategies and Supports
Leverage Support from Key Legislators. Certain legislators worked very hard to make Expansion happen;
they engaged in long conversations with the administration to understand the design features and to
make sure they could “own” and advocate for every aspect of the model. Their support reportedly played
an important role in the ultimate passage. Elements that helped bring conservative legislators on board
included purchasing private health plans, using HSAs and work requirements.
Source: Kaiser Family Foundation
ARKANSAS

Health Management Associates 15
Work with CMS. Planners worked closely with CMS to design a model that would be approved both by
the federal government and the courts. “We had real-time, up-to-the-minute conversations with [CMS]
so that legislation would promise everything but not more than could be granted and upheld”-AA
Engage a Broad Coalition. “AR Works” included 35 provider, advocacy, and faith-based groups
supporting Expansion, including AARP’s large volunteer network. Some had relationships and would
engage with policymakers. “It was not hard to get stakeholders on board”-RH
Post-Implementation Opposition
Some state leaders attempted to roll back Expansion, but CMS rejected a proposed cut in eligibility to 100
percent of the FPL. The current Governor and most legislators continue to support Expansion (achieving
a supermajority to continue funding it each year) and understand the negative impact its revocation
would have on the state budget, and on the state itself.
Impacts
Despite more participants and higher early monthly per person insurance payments than expected, the
state experienced significant savings.
Initial savings came largely from transferring pregnant women -- insuring them before they got
pregnant -- and the medically needy population to the Expansion program, which draws a much
higher federal match
Direct offsets/savings to the state included a reduction in the uncompensated care
appropriation for the university hospital; a cut in the Medicaid medically needy program; and a
reduction in funds formerly allocated for the uninsured (e.g., community health and mental
health centers, health department, hospital DSH)
Interviewees noted that rather than the Expansion necessitating pulling funds from other areas
(such as education) or increasing state income taxes, Arkansas was able to use savings from
Expansion toward cutting state income taxes (e.g., a 2015 middle class income tax cut was
estimated to provide relief of $33.7M in FY16 and more than $100M per year from FY17-FY20)
The indirect effects of the large infusion of federal funds are harder to quantify but reportedly
have had myriad benefits to the state
“Each federal dollar turns over two to three times…jobs created, income tax, sales, tax…benefits to rural
infrastructure…”-RH
Rural Hospitals and Infrastructure
Expansion supported rural hospitals and broader rural infrastructure; Arkansas experienced fewer
hospital closures than non-expansion states.
Provider Workforce
Using MCOs in the Marketplace for the Expansion enrollment meant contracted providers were paid
market rates, addressing concerns about potential provider shortages.
Lessons
Be prepared to address Expansion opponents’ concerns by providing facts and examples from
other states’ experience to make valid projections and counter myths based on anecdotes.
It is possible to find political common ground and ideological compromise ––all sides may have to
accept some elements they deem less than ideal.
Health Management Associates 16
Establish a very broad coalition that favors expansion and is willing to talk to policymakers, then
maintain that coalition to support implementation.
Be honest about the weaknesses in the Medicaid program, and address how Expansion will be
used to improve the financing or health care delivery system. Expansion is an opportunity for a
tremendous infusion of federal dollars.
Work with CMS to get what you can, but do not let state legislative language promise more than
could be upheld in the courts.
Indiana’s HIP 2.0 Expansion Model
Indiana expanded its Medicaid program in February 2015 under then-Governor Mike
Pence through a Section 1115 waiver called the Healthy Indiana Plan (HIP) 2.0, based
on the redesign of an earlier, pre-ACA Medicaid expansion. “Consumer driven”
features include member contributions to an HSA-like Personal Wellness and
Responsibility (POWER) Account whereby members decide how to use their account
to meet their $2,500 deductible and get a refund of dollars not spent, encouraging
them to utilize health care services wisely. “Personal responsibility” incentives include
penalties for contribution nonpayment (loss of certain benefits for those below
100 percent of the FPL and a “lock out” of coverage for six months for those above
100% FPL), and higher copays for non-emergent use of the ER. The 2018 waiver
added new incentives to promote healthy behaviors. Indiana began phasing in a
work/community engagement reporting requirement in July 2019, but
enforcement was suspended in Oct 2019 until a federal lawsuit is resolved.
Expansion Implemented
2015
Total Medicaid Enrollment
1,362,300
Expansion Group Enrollment
Newly Eligible: 322,700
Not Newly Eligible: 161,800
(FY 2017) Source: Kaiser Family Foundation
Early Concerns and How They Were Addressed
Key stakeholders involved in Expansion in Indiana shared the following about strategies, expectations,
and experience:
‘How would it be viewed if we, as a Conservative administration and legislature, expand an
entitlement?’ - Faced with concerns over the renewal of the existing HIP program, the Governor’s plan
built on HIP’s conservative principles. The initial 100 percent federal match, and support from
conservatives in Washington, DC, also helped to promote the plan at home.
“Monthly contributions and lockout for non-payment –these types of guardrails were necessary to get a
lot of conservative Republicans to go along with the program.” -LK
Also, Indiana’s Governor has more authority and discretion to design and pursue waivers than in many
other states. With support from a five-person State Budget Commission, the Governor was able to pursue
Expansion without overwhelming support from legislators. Later established in statute at the request of
Governor Pence, the program is not re-debated with each legislature and would be difficult for future
Source: Kaiser Family Foundation
INDIANA

Health Management Associates 17
governors to dismantle unilaterally. “In Indiana, once issues are in the budget and an accepted program,
unless it is failing dramatically, it is not a point of contention again”-LK
‘Will the federal government approve the consumer-driven model?’ CMS pushed back on some proposed
restrictions but was eager to get more Republican-led states on board with Expansion. Despite much
conflict over details, CMS ultimately approved the model.
“Politically, we were able to keep our homegrown Healthy Indiana program and allow the Governor to call
it a model for other states.” -JM
‘How to come up with the state financing share in perpetuity without increasing individual income
taxes?’ - Planners used the cigarette tax from HIP 1.0, supplemented by an increase in the hospital
provider tax structured to increase (up to the cap) or decrease based on the program’s costs. The hospital
association was a willing partner, given that the large losses from uncompensated care were threatening
the existence of some of the hospitals.
‘Fear the federal government will pull out of financing and leave Indiana with an “uncontrollable
mandate”’ - HIP 2.0 designers included protections whereby the state can terminate the waiver
immediately if the FMAP changes or the state’s ability to collect the hospital assessment changes.
‘There is inadequate provider capacity for a large influx of covered people’ - To ensure provider
participation and expand capacity, HIP 2.0 would pay providers Medicare rates, and the traditional
Medicaid program’s rates would increase to 75% of Medicare rates. FQHCs were able to absorb more
primary and preventive visits.
Key Strategies and Supports
“People in decision making power had to find a practical solution.” - LK.
Compelling Messages from the Governor:
There was a group of low-wage workers just above the Medicaid eligibility line without employer
coverage
With HIP 2.0, enrollees have skin in the game—they are incentivized to be more engaged in their
personal health, exhibit healthy behaviors and take ownership over their health care decisions
HIP 2.0 helps educate enrollees on the concepts of private coverage (premiums, benefit structure,
etc.) to prepare them for moving off Medicaid and into employer coverage
Without Expansion, Hoosiers’ federal tax dollars would continue to be redistributed to Expansion
states
Broad support: Because Indiana is a conservative state, Expansion advocates knew they would have to
accept some of the HIP features they otherwise would not support in order to see Expansion passed.
Consumer advocates got on board and were very helpful in relaying their support to the Obama
administration.
Consumer Education: The state invested a few million dollars and engaged all stakeholders in advertising
and educating people about HIP 2.0. The hospital association was instrumental in getting the message out
in communities. Still, along about half of Expansion enrollees reportedly understood the POWER account,
and fewer understood the entire model.
Impacts
Take-up Rates. Early enrollment was faster than expected (reflecting a 73% take-up rate among those
eligible
22
) but then leveled off, with lower growth in recent years associated with a strong economy and
low unemployment.

Health Management Associates 18
Financing and Offsets. The program had no substantial impact on the state budget or General Fund
because the state share was funded through the cigarette tax (continued from HIP 1.0) and hospital
provider tax that was increased from 4.5 percent to 5.5 percent, calculated to cover the new costs. The
cigarette tax covers about 42 percent, and the hospital tax 58 percent of the costs. Both the hospital
assessments and the revenues have been lower than expected due to lower than anticipated annual
enrollment increases.
Behavioral health expenditures: general revenue only payments to Community Mental Health
Clinics (CMHCs) declined; and a Substance Use Disorder (SUD) waiver allowed short-term IMD
stays under Medicaid aligned with Expansion (as many individuals with SUD are childless adults
and were covered through Expansion)
Indigent Fund expenditures: the state reduced this line item by $50 million per year
Correctional Health expenditures: incarcerated individuals hospitalized beyond 24 hours were
enrolled in Medicaid temporarily via the Expansion, resulting in some savings to the state
Administrative Costs. The health plans are conducting many of the administrative tasks, and
administrative costs are built into the fees charged to the hospitals (capped at $170 per member per year).
The state estimated that the POWER account, copays and contributions result in about a five percent
savings vs. traditional Medicaid, and these savings outweigh the additional administrative costs of these
components.
Premiums and Individual Responsibilities. Most of the Expansion population were already employed and
reportedly were willing to pay into the POWER account and the scaled ER copays, especially knowing that
the alternative was no coverage or fewer benefits. Throughout the life of the program, between 60- and
70 percent of program enrollees have made their monthly required contributions.
23
“Anyone who has
financial accountability will take in interest in how it works… you could point to the shared responsibility
of government, hospitals, and patients.”- LK
Healthier workforce. Interviewees felt that expansion made Indiana more competitive for employers who
want to locate to states with a healthy workforce versus some states in the south that have not
implemented Expansion, such as Texas or Florida.
Health system stabilization. Expansion reportedly allowed for investments in the health care workforce
and stabilized revenues for hospitals; Indiana has not had hospital closures until one rural hospital closed
last year.
Lessons
The loud voices at either end of the spectrum represent relatively small numbers of people. If you
run a responsible program that helps people, the majority are willing to go along.
Leverage the influx of federal dollars from the Expansion to reform the health care delivery and
payment systems – e.g., negotiating better payment models with providers. (Indiana did not
reportedly take advantage of this opportunity.)
Late expanders have the advantage of looking at data from early expanders in the region to
support more accurate projections on take-up, costs, etc.
Consider and plan for mechanisms to enable the state to afford its share of costs in the short and
long term, or to pull back if the federal share goes away.
Expansion and related programs are easier to implement when the economy is good, when there
is low unemployment and low demand for social services. But be aware that during a strong

Health Management Associates 19
economy, Medicaid enrollment may be down but cost per person will be higher because enrollees
are more likely to have high medical needs.
Ohio’s Medicaid Expansion
In 2013, the federal government approved then-Governor John Kasich’s (R) State Plan
Amendment laying out Medicaid Expansion for Ohio. The state’s General Assembly’s
Controlling Board
24
voted 5-2 to increase the appropriation necessary to receive
Expansion funds, leading to implementation on January 1, 2014. The Republican House
and Senate approved budgets that included the Expansion in 2015, 2017 and 2019. In
2017, the legislature passed work requirements (with some exemptions) that CMS
approved in 2019 and which are scheduled to begin in 2021.
Expansion Implemented
2014
Total Medicaid Enrollment
3,087,800
Expansion Group
Enrollment
Newly Eligible: 655,000
Not Newly Eligible: 64,900
(FY 2017) Source: Kaiser Family Foundation
Early Concerns and How They Were Addressed
Key stakeholders involved in Expansion in Ohio shared the following about
strategies, expectations, and experience:
‘Expansion would further ‘swamp’ the Medicaid system’ -The Governor initially opposed expanding what
he considered an inefficient Medicaid program, so the administration spearheaded an initiative that cut
the number of managed care contracts and saved about one billion dollars of administrative overhead –
reducing the spending growth rate from about nine percent to three percent per year.
“It was critical to get the fiscal shop in order and then when it became an option to expand, the Governor
was much more comfortable.- GM
‘The Republican majority in the state legislature will not vote for Expansion’ -
Administration planners spoke with each legislator and learned that most supported Expansion but feared
losing the primary if they voted for it. So, the Governor took a different path: he pursued a State Plan
Amendment and worked with Ohio’s Controlling Board to secure votes for the necessary appropriation,
sparing the legislature from directly voting on Expansion. The administration did ask legislators to not
oppose Expansion, which helped limit the level of opposition. In the next budget, the legislature enacted,
and the Governor did not veto, work requirements, which are due to go into effect in 2021.
‘The federal government will pull back on its commitment’-To help address conservatives’ concerns, the
administration incorporated protections, including a trigger that would force the Ohio legislature to vote
on whether to keep the Expansion if federal funding went away.
Source: Kaiser Family Foundation
OHIO

Health Management Associates 20
Key Strategies and Supports
Coverage Gap. Governor Kasich reportedly became an
ardent Expansion supporter when he saw the injustice of
the coverage gap: people with incomes between 100 and
400 percent of the FPL were receiving exchange subsidies,
while those with incomes below 100 percent were getting
nothing. The Governor had the power to address this, and
he also reportedly foresaw that voters would favor
Expansion.
Compelling Messages:
People who would be eligible for Expansion
coverage include 29,000 veterans and their
families, as well as “people we know.” “We looked specifically for ‘real’ Ohioans … to make clear
this is your neighbors, people who are in your family’- TP
Expansion would help avoid cost-shifting, as well as loss of federal tax dollars to other states. “If
you don’t spend the money in Ohio, it will go elsewhere.”
Data shows better health outcomes for people with substance use disorders and mental illness
who have insurance
Expansion would enable people to enter and stay in the workforce. “Expansion gives people the
opportunity to be healthy, look for a better job that might offer health care, and move off
Medicaid.” - TK
Sheriffs were effective advocates. Despite a broad coalition favoring Expansion and providing monetary
and organizational support, certain people who “spoke” to a conservative audience were most influential.
County sheriffs, seeing untreated mental illness and substance use disorder for those in and leaving jails,
were effective in arguing that there is insufficient behavioral health capacity in the community without
the Expansion. “We knew that Medicaid expansion would save money for the system but the community
capacity argument was the more compelling one.”- GM
Financing Secured. The administration worked with CMS to guarantee financing for the state’s portion
(relying on an existing 1 percent health insurance tax and converting an existing state sales tax to an open-
ended 5.5 percent managed care plan per member per month tax, most on Medicaid MCOs). “ We made
the determination [Expansion] would be affordable in out years…and that has been borne out, in contrast
to beliefs of some legislators ”- TK
Impacts
Detractors claimed that Expansion ‘blew up the budget,’ but analyses revealed savings that helped
solidify the state’s finances and support other initiatives:
The aggregate projected enrollment was close to projections, balancing an underestimate of
newly eligible people enrolling and overestimate of the woodwork effect. Enrollment then
declined by 11 percent in the first year and has been stable, with Expansion leading to a significant
decrease in per member per month costs overall as new enrollees were typically lower cost than
the existing Medicaid population.
The state benefited financially (more than $300 million annually) from revenue and savings
generated by the Expansion, including savings from prison expenditures ($18 million/year). “Free
money for a number of years is hard to pass up.”- GM
Figure 2: Ohio Income Eligibility Limits and Coverage

Health Management Associates 21
A very small group of legislators have tried to repeal or scale back Expansion for political reasons,
but they would need to fill a large budget hole; opposition has reportedly decreased each year.
Hospital “community benefit” reports indicated uncompensated care declined as a result of the
Expansion.
Even though the state match for Expansion increased to 10 percent for 2020, the projected
effective match in Ohio will actually be 3 percent due to cost offsets (e.g., drug rebates for
Expansion members, enhanced FMAP for hospital upper payment limits (UPLs), health insurance
premium taxes on larger
number of insured). In 2021,
Ohio’s expansion is estimated
to cost $5.3B ($534M state
share) and generate Ohio
general fund savings/revenue
of $373M. The net cost of the
expansion for Ohio is $161M,
which is 3 percent of the total
cost, according to the Ohio
Office of Budget and
Management analysis (July
2018).
Behavioral Health Restructured. Expansion helped to increase Ohio’s behavioral health system capacity
by about 60 percent over five years.
25
General Fund spending in clinical services that would be covered under Medicaid Expansion was
shifted to fill in gaps, including in recovery housing subsidies, suicide prevention/community-
based crisis intervention, addiction staff in prisons, programs for individuals diverted from or
released from jails, and transportation. The prison system partnered with Medicaid and MCOs to
enroll people before they left prison. “It really helped to have the criminal justice system
represented in our advocacy.” – TP
Over 70 percent of people enrolled in Expansion had at least one mental health or addiction
service paid through Medicaid, reflecting pent up demand; with waiting lists for services two years
post-Expansion, the state provided grants to expand capacity, including clinical supervision for
practitioners trying to achieve licensure, and training to increase their scope of practice
Medicaid “professionalized” behavioral health rates, which expanded capacity in general
(hospitals, primary care) though some small providers struggled to hire practitioners with higher
skills needed to benefit from the new rates
Health and Productivity: Emergency department use stabilized, and enrollees were better able to get and
keep jobs as their chronic health conditions were more likely to be under control. Enrollees reported it
was easier to work (84 percent) or if unemployed, easier to look for work (60 percent). A 2018 assessment
found that 71 percent of members who moved off Expansion coverage had found work that offered health
insurance.
26
Figure 3: Ohio’s Share of Medicaid Expansion Costs (in Millions)

Health Management Associates 22
Rural Hospitals and Infrastructure: Expansion supported rural hospitals and broader rural infrastructure.
Ohio experienced fewer hospital closures than non-expansion states. “Not only did Expansion not cause
an access problem, it was the key to starting to address access problems in critical areas.”- GM
Provider workforce: Expansion was accomplished through MCOs that were required (through standard
network requirements in state contracts) to ensure enrollees had access to providers, which meant the
MCOs paid market rates to ensure there was no shortage of providers.
Administrative efficiencies: Expansion was leveraged to build a new online eligibility system connected
to income-based data (TANF, SNAP, child welfare), eliminating much county-level casework and improving
efficiency.
Lessons
Take advantage of the experience in other states
Start with a solid fiscal foundation, and examine how Expansion could fit into transforming and
improving Medicaid payment and health care delivery, and redirect funds to address longstanding
gaps
Discuss the policy and budget impact simultaneously. Ohio’s budget office, Governor’s office, and
agencies involved all worked very closely together.
Be strategic in who is out front during the campaign. Consider what kind of advocacy makes it
easier for people to vote “yes” (or remain quiet if they are a “no”) – e.g., local respected officials,
local hospital leaders
More complicated “bells and whistles” (e.g., 1115 waiver) can drag the process out, adding time
and risks
Keep financing straight-forward, building on existing mechanisms when possible
Work to increase community-based provider capacity, so that when you expand you can meet
demand

Health Management Associates 23
Summary and Conclusions
This study provides a targeted analysis of the economic impact of an ACA Medicaid Expansion in Missouri,
with an emphasis on the effects on the state budget. As Missouri considers the costs and benefits of
adopting the ACA Medicaid Expansion, state officials and private sector leaders should consider the
experience of other similarly situated states that have taken this step in the past few years. HMA has
examined the experience in three such states—Ohio, Indiana, and Arkansas--through interviews with
leaders in those states. We have also conducted a literature search and reviewed numerous published
reports and articles containing research findings on the impact of the Medicaid Expansion on state
budgets, the economy, the work force, uncompensated care, and a wide range of state-only program
savings that could offset some of the state costs of the Medicaid Expansion.
Our study found that a large portion of the states’ share of the cost of enrolling and serving the new
population, as well as other state costs that are affected by the Expansion, have been offset by savings in
previously state-only outlays, existing Medicaid spending diverted to the higher match rate of the
expansion, and existing revenue streams. Substantial savings have emerged in mental health and
substance use disorder spending. Another important source of state savings involves the incarcerated
population, including health spending while they are in prisons and assistance with making the transition
back into the community. Further savings can be expected as people in the “Spenddown” window,
awaiting the day when their very high out-of-pocket medical costs make them eligible for Medicaid
through that path, are instead enrolled in the Expansion population with a higher federal match.
We learned the law enforcement community supported expansion (contrary to expectations). County
sheriffs, who see first-hand the impact of untreated mental illness and substance use disorders for those
in and leaving jails, effectively argued there is insufficient behavioral health capacity in the community
without Expansion. The Expansion is perceived as facilitating redesign of a health care infrastructure that
promotes effectiveness, the right balance between public and private insurance, and Medicaid program
integrity.
Our study also found that, contrary to some predictions, Medicaid spending per capita did not soar
following Expansion in the three states. Medicaid spending increases were mostly in line with nationwide
trends. There was also a perception among state leaders, and supporting research evidence, that as poor
and near-poor uninsured adults gained affordable health coverage through Medicaid, their ability both to
search for work and to obtain and retain jobs increased, which provides a pathway to financial
independence and some added state revenues.
A Medicaid Expansion in Missouri would bring a substantial infusion of new federal outlays into the state,
with a positive impact on the state’s economy. Many of the Expansion states have found that, if carefully
designed, the state’s 10 percent cost share can be responsibly financed, and provisions can be
implemented to manage spending increases. Even setting aside the savings and revenue opportunities
relative to the state cost, it is important to note that among all states that have expanded, none have
voted to repeal Expansion, despite many opportunities to do so, strongly indicating that the Expansion
creates positive effects on state budgets. The Expansion can help lift many adults out of poverty, reduce

Health Management Associates 24
the public-to-private cost shift, facilitate health system transformation, and improve health outcomes for
large numbers Missourians.
1
(Missouri State Auditor's Office 2019)
2
(Centers for Medicare & Medicaid 2019)
3
(Federal Reserve Bank of St. Louis 2019)
4
(United States Census Bureau 2019)
5
(Census Bureau's American Community Survey 2018)
6
(Center for Health Economics and Policy 2019)
7
(Antonisse, et al. 2019)
8
(Missouri State Auditor's Office 2019)
9
(Center for Health Economics and Policy 2019)
10
(Commonwealth of Virginia Senate Finance Committee 2018)
11
(The Stephen Group 2016)
12
(Ayanian, et al. 2017)
13
(Bureau of Business and Economic Research, University of Montana 2018)
14
(Stoddard 2019)
15
(Center for Health Economics and Policy 2019)
16
(Center for Health Economics and Policy 2019)
17
(Center for Health Economics and Policy 2019)
18
(Antonisse, et al. 2019)
19
(Richardson, Llorens and Heidelberg 2018)
20
(The Colorado Health Foundation 2016)
21
(The Ohio Department of Medicaid 2018)
22
(The Lewin Group 2016)
23
(The Lewin Group 2017)
24
(Ohio Office of Budget and Management 2019)
25
(Ohio Departments of Medicaid and Mental Health and Addiction Services 2017)
26
(The Ohio Department of Medicaid 2018)

Health Management Associates
References
Antonisse, Larisa, Rachel Garfield, Robin Rudowitz, and Madeline Guth. 2019. "The Effects of Medicaid
Expansion under the ACA: Updated Findings from a Literature Review." Kaiser Family
Foundation. https://www.kff.org/medicaid/issue-brief/the-effects-of-medicaid-expansion-
under-the-aca-updated-findings-from-a-literature-review-august-2019/.
Ayanian, John Z., Gabriel M. Ehrlich, Donald R. Grimes, and Helen Levy. 2017. "Economic Effects of
Medicaid Expansion in Michigan." The New England Journal of Medicine.
Bureau of Business and Economic Research, University of Montana. 2018. "The Economic Impact of
Medicaid Expansion in Montana." The Montana Healthcare Foundation. April. Accessed
December 11, 2019. https://mthcf.org/wp-content/uploads/2018/04/BBER-MT-Medicaid-
Expansion-Report_4.11.18.pdf.
Census Bureau's American Community Survey. 2018. "Health Insurance Coverage of the Total
Population." Kaiser Family Foundation . https://www.kff.org/other/state-indicator/total-
population/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:
%22asc%22%7D.
Center for Health Economics and Policy. 2019. "Analysis of the Fiscal Impact of Medicaid Expansion in
Missouri." Institute for Public Health at Washington University. February.
https://publichealth.wustl.edu/wp-content/uploads/2019/02/Analysis-of-the-Fiscal-Impact-of-
Medicaid-Expansion-in-Missouri-IPH.pdf.
Centers for Medicare & Medicaid. 2019. "CMS 64 FY 2019 Net Expenditures."
Commonwealth of Virginia Senate Finance Committee. 2018. "Overview of the Governor’s Introduced
Budget 2018." Accessed December 11, 2019.
http://sfc.virginia.gov/pdf/health/2018/010818_No1_Jones_DMAS%20Budget%20Briefing.pdf.
Federal Reserve Bank of St. Louis. 2019. Labor Force Participation Rate for Missouri. October.
https://fred.stlouisfed.org/series/LBSNSA29.
Missouri State Auditor's Office. 2019. "Fiscal Note (20-063)." May 23.
https://app.auditor.mo.gov/Repository/Notes/20-063.pdf.
Ohio Departments of Medicaid and Mental Health and Addiction Services. 2017.
Ohio Office of Budget and Management . 2019. "Controlling Board Portal ."
https://www.ecb.ohio.gov/public/default.aspx?MSG=1&ReturnUrl=%2f.
Richardson, James A., Jared J. Llorens, and Roy L. Heidelberg. 2018. "Medicaid Expansion and the
Louisiana Economy." Louisiana Office of the Governor. March. Accessed December 2019.
http://gov.louisiana.gov/assets/MedicaidExpansion/MedicaidExpansionStudy.pdf.

Health Management Associates
Stoddard, Martha. 2019. "Nebraska Medicaid expansion plan would rein in state costs; critics say it cuts
coverage, benefits." Omaha World-Herald. December 22.
https://www.omaha.com/livewellnebraska/health/nebraska-medicaid-expansion-plan-would-
rein-in-state-costs-critics/article_c4127595-c78e-5863-9c6e-f34ab71dbe1d.html.
The Colorado Health Foundation. 2016. "Assessing the Economic and Budgetary Impact of Medicaid
Expansion in Colorado: FY 2015-16 through FY 2034-35." June.
https://www.coloradohealth.org/reports/assessing-economic-and-budgetary-impact-medicaid-
expansion-colorado-fy-2015-16-through-fy.
The Lewin Group. 2017. "Healthy Indiana Plan 2.0: POWER Account Contribution Assessment." March
31. https://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-
Topics/Waivers/1115/downloads/in/Healthy-Indiana-Plan-2/in-healthy-indiana-plan-support-
20-POWER-acct-cont-assesmnt-03312017.pdf.
—. 2016. "Indiana Healthy Indiana Plan 2.0: Interim Evaluation Report." July 6.
https://www.in.gov/fssa/files/Lewin_IN%20HIP%202%200%20Interim%20Evaluation%20Report
_FINAL.pdf.
The Ohio Department of Medicaid. 2018. "2018 Ohio Medicaid Group VIII Assessment: A Follow-Up to
the 2016 Ohio Medicaid Group VIII Assessment." August.
https://medicaid.ohio.gov/Portals/0/Resources/Reports/Annual/Group-VIII-Final-Report.pdf.
The Stephen Group. 2016. "Arkansas Health Reform Legislative Task Force." Arkansas State Legislature.
Accessed December 11, 2019.
http://www.arkleg.state.ar.us/assembly/Meeting%20Attachments/836/I14805/Final%20Approv
ed%20Report%20from%20TSG%2012-15-16.pdf.
United States Census Bureau. 2019. "Health Insurance Coverage in the United States: 2018." November.
https://www.census.gov/content/dam/Census/library/publications/2019/demo/p60-267.pdf.
