
Pittsburg State University Pittsburg State University
Pittsburg State University Digital Commons Pittsburg State University Digital Commons
Doctor of Nursing Practice Scholarly Project Irene Ransom Bradley School of Nursing
Summer 7-28-2021
DEPRESSION KNOWLEDGE IN NURSING HOME LICENSED DEPRESSION KNOWLEDGE IN NURSING HOME LICENSED
PRACTICAL NURSES, REGISTERED NURSES, AND CERTIFIED PRACTICAL NURSES, REGISTERED NURSES, AND CERTIFIED
NURSING ASSISTANTS NURSING ASSISTANTS
Jason He>in
Pittsburg State University
Follow this and additional works at: https://digitalcommons.pittstate.edu/dnp
Part of the Nursing Commons
Recommended Citation Recommended Citation
He>in, Jason, "DEPRESSION KNOWLEDGE IN NURSING HOME LICENSED PRACTICAL NURSES,
REGISTERED NURSES, AND CERTIFIED NURSING ASSISTANTS" (2021).
Doctor of Nursing Practice
Scholarly Project
. 58.
https://digitalcommons.pittstate.edu/dnp/58
This Scholarly Project is brought to you for free and open access by the Irene Ransom Bradley School of Nursing at
Pittsburg State University Digital Commons. It has been accepted for inclusion in Doctor of Nursing Practice
Scholarly Project by an authorized administrator of Pittsburg State University Digital Commons. For more
information, please contact [email protected].
DEPRESSION KNOWLEDGE IN NURSING HOME LICENSED PRACTICAL
NURSES, REGISTERED NURSES AND CERTIFIED NURSING ASSISTANTS
A Scholarly Project Submitted to the Graduate School in Partial Fulfillment of the
Requirements for the Degree of Doctor of Nursing Practice
Jason Heflin
Pittsburg State University
Pittsburg, Kansas
August 2021
ii
DEPRESSION KNOWLEDGE IN NURSING HOME LICENSED PRACTICAL
NURSES, REGISTERED NURSES AND CERTIFIED NURSING ASSISTANTS
An abstract of the Scholarly Project by
Jason Heflin, BSN
The purpose of this project was to ascertain whether providing education to
licensed nurses and certified nurse aide staff in nursing homes results in an increased
awareness and recognition of depression and depressive symptoms among the nursing
home population. A descriptive research design was used to identify knowledge of
nursing staff in long-term nursing home facilities before and after depression and
depressive symptom education. The study utilized a one-group pre-test/post-test design
with nursing home staff that interact with nursing home residents during a normal
workday. A total of 26 of the 30 participants (86.6%) achieved a pre-test score of 22 or
greater representing satisfactory performance. The mean post-test score was 24.2333 with
a standard deviation of 1.95965. An average of 86.5% was achieved by the participants
on the pre-test.
iii
TABLE OF CONTENTS
CHAPTER I 1
DEPRESSION IN NURSING HOMES 1
SIGNIFICANCE 2
PURPOSE 2
THEORETICAL FRAMEWORKS 3
PROJECT QUESTIONS 5
DEFINITION OF KEY TERMS/VARIABLES 6
CONCEPTUAL IMPLICATIONS 7
LOGIC MODEL 8
CHAPTER CONCLUSION 12
CHAPTER II 14
LITERATURE REVIEW 14
SEARCH PARAMETERS 14
SCOPE OF DEPRESSION AMONG ADULTS 15
INCREASING RATES OF DEPRESSION AMONG THE ELDERLY 16
WOMEN AND DEPRESSION 18
PRIMARY CARE AND DEPRESSION 18
TREATMENT FAILURE AND CASES OF DEPRESSION 19
ELDERS IN NURSING HOMES 19
CONTRIBUTORS TO LATE LIFE DEPRESSION 20
IMPACTS OF DEPRESSION 21
DEPRESSION EDUCATION FOR POLICY CHANGE IN NURSING HOMES 21
LICENSED NURSE AND CAN EDUCATION AND TRAINING 23
DELIVERY OF EDUCATION 24
CHAPTER CONCLUSION 25
CHAPTER III 27
PROJECT DESIGN 27
METHODS 27
PROJECT QUESTIONS 28
PROJECT SITE AND POPULATION 29
DATA COLLECTION 29
MEASUREMENT INSTRUMENTS 29
ETHICAL CONSIDERATIONS/PROTECTION OF HUMAN SUBJECTS 30
DATA ANALYSIS 30
RELIABILITY AND VALIDITY 30
ANALYTICAL METHODS 31
TIMELINE 31
ASSUMPTIONS 31
BUDGET 31
STRENGTHS AND WEAKNESSES 32

iv
CHAPTER IV 33
FINDINGS 33
DEMOGRAPHICS 33
DESCRIPTION OF KEY VARIABLES 35
PRE-TEST AND POST-TEST 35
RESEARCH QUESTION RESULTS 35
SUMMARY 43
CHAPTER V 45
DISCUSSION 45
EVALUATION OF THEORETICAL FRAMEWORK 48
RECOMMENDATION FOR FUTURE RESEARCH 48
LIMITATIONS OF STUDY 49
IMPLICATIONS FOR PRACTICE/HEALTH POLICY/EDUCATION 49
CONCLUSION 49
REFERENCES 51
APPENDIX A 60
APPENDIX B 62
APPENDIX C 69

v
LIST OF TABLES
TABLE PAGE
1. DEMOGRAPHIC DATA 34
2. PRE AND POST-TEST SIDE BY SIDE COMPARISON 36
3. PRE-TEST RESULTS HISTOGRAM 37
4. POST-TEST RESULTS HISTOGRAM 37
5. BOXPLOT 38
6. PAIRED SAMPLES TEST 39
7. PRE-TEST/POST-TEST SCORE COMPARISON 40
8. SPEARMAN’S RHO CORRELATION 41
9. SCATTER PLOT OF SCORES BY LEVEL OF EDUCATION 42
10. PARTICIPANT ABILITY TO IDENTIFY RISK FACTORS OF DEPRESSION 43

vi
LIST OF FIGURES
TABLE PAGE
1. BENNAR’S NOVICE TO EXPERT THEORY 5
2. LOGIC MODEL OF SCHOLARLY PROJECT 12
1
Chapter I
Depression in Nursing Homes
Depression is a disorder that is manifested in the form of sadness, feelings of
guilt, sleep disturbances, and lack of concentration (Depression and Older Adults, 2017).
A multi-factorial condition, The World Health Organization (WHO) notes that depression
is brought about by social, psychological, and biological factors (2018). The disorder is a
common problem in nursing homes. In most cases, the elderly suffers from multiple
conditions such as dementia and depression, and the management of these problems calls
for clinical treatment and management of the conditions. The focus of this project was to
foster the recognition of depressive symptoms in nursing home residents by providing
targeted education to licensed nursing and nurse aide staff.
People with depression are likely to be dependent on others; consequently, the
treatment process is a herculean task for nursing home staff (Kvæl, Bergland, & Telenius,
2017). Depression is associated with multiple conditions including diabetes mellitus,
anorexia, and other chronic diseases. In addition, the loss of physical functions often
occurs with those in nursing homes and may lead to symptoms of depression for many
residents. Nursing home staff can have trouble in the diagnosing, treating, and managing
of patients with diverse depressive disorders. Nursing homes utilize various techniques in
the identification of depressed patients, including the Pre-Admission Screening and
2
Annual Resident Review (PASARR) system, which enhances the detection of different
depressive conditions (Lantz, 2019). Despite screening interventions, depression in
nursing homes continues to be underdiagnosed (Simning & Simons, 2017). Therefore, the
widespread incidence of depression in nursing homes calls for proper intervention in
terms of training for the identification of symptomology.
Significance
Nursing homes are vital institutions since they cater to the needs and management
of the elderly in society. The rise in the number of older adults in the world calls for an
increase in care for their physical, social, and psychological needs. Old age is
accompanied by conditions such as dementia and the loss of vital skills which affect the
quality of life and increase the demand for psychiatric interventions. The incidence of
depression and dementia has risen, and an approximate 47.5 million are affected by
dementia (Simning & Simons, 2017). The CDC (2014) notes that the nursing home
population has an incidence of depression approximately double of other care modalities
in the aging population. Additionally, the WHO statistics predict the incidence of people
with depression to rise to 76.5 million by 2030. This alarming trend in the increase in
depression in the elderly will impact many aspects of healthcare; hence, the need for
intervention. Most countries report a high percentage of older adults with cognitive
impairment that causes depression. For example, in Brazil, 64.6 % of individuals over 65
years and living in nursing homes have cognitive problems, which contribute to
depressive orders (Kvæl et al., 2017). In essence, nursing homes in most regions of the
world have older adults who suffer from depression and other associated disorders.
Purpose
3
Depression in nursing homes is a subject of concern, and the purpose of this study
was to improve on the recognition (diagnosis) of its various symptoms. Also, the study
sought to develop an educational presentation that will increase licensed nurses and
Certified Nursing Aide (CNA) knowledge of depression with the goal of reducing the
cases of under treatment and inappropriate management of depression among nursing
home residents. The study aimed to enhance the symptom recognition techniques and the
appropriate preparation of nursing home staff on the subject of depression.
The upsurge in the incidence of depression in nursing homes calls for an
integrative approach to education and training for licensed nurse and CNA staff, which
leads to the combating of the risk factors of depressive conditions. Depression in nursing
homes calls for the application of positive experiences for the elderly who often suffer
from loneliness and other risk factors of the condition. As transitional stages for the
elderly, nursing homes should be engaging in terms of positive activities to promote the
cognitive and physical health of the elderly. Also, the incorporation of a proper diet and
exercise helps reduce depression risk factors and symptoms in nursing homes. The study
sought to enhance the role of licensed nursing and CNA staff in the reduction of
depression in nursing homes through the application of education and practice.
Theoretical Frameworks
Multiple theories can help explain the manifestation of depression in the aging
populace, and they can help direct methods to combat disorders associated with this
condition. Theoretical perspectives can help justify non-medical interventions to the
multiple depressive disorders of the elderly. Each approach formulates different
techniques such as relaxation, behavioral change, and exercise remedies for depression
4
(Simning & Simons, 2017). The activity theory is reflected in the transitional challenges
the elderly face in nursing homes. The theory asserts that individuals must maintain an
active role in life to maintain satisfaction in life (Bell, n.d.). Any form of activity
contributes to wellbeing as it gives the individual a sense of value. The nursing home
environment is limiting to the elderly; this means that they have limited control over
activities and dietary choices. Nursing homes polices dictate the nature of physical
activity and the amount of time allocated for physical activity. Also, many elderly have
limitations concerning the use of their finances and access to social resources and other
social points of contact (McCarthy-Zelaya, 2016). Nursing homes are perceived holding
facilities for the aging, who, in turn, lose social contacts and many forms of control over
their lives; these factors contribute to mental and psychological disorders (Guimarães et.
al., 2019).
Another theory that could be applied to the identified problem of depression in
nursing homes being undertreated is Dr. Patricia Bennar’s Novice to Expert Theory. The
theory asserts that all nurses range in experience on any given subject on a five-level
spectrum from novice to expert (Petiprin, 2020). A problem that remains unrecognized
continues to be a problem. If nursing home staff lack the knowledge required to
recognize depressive symptoms, it will likely remain untreated. Current CNA
certification requirements vary state by state but primarily focus on activities of daily
living and physical modalities of care (Institute of Medicine, 2008). Identification of
depression may be improved if the healthcare workers that spend the most time with the
nursing home population is better equipped to recognize symptoms and bring attention to
the problem.

5
For this study, the researcher educated three nursing home’s licensed nursing and
CNA staff in the recognition of depressive symptoms in the nursing home population to
reduce depression undertreatment. Application of Bennar’s Novice to Expert Theory can
help identify shortcomings in staff education and provide training for nursing home staff
to be better prepared. Licensed nursing staff will require training as well to ensure their
depression knowledge is adequate as they will receive notification from CNA staff
regarding symptoms nursing home resident’s display.
Figure 1. Bennar’s Novice to Expert Theory
Note: This figure shows the five levels of the Benner Novice to Expert Theory. From
Discussion on Benner’s Theory of Novice to Expert. (2019).
https://www.needassignmenthelp.com/blog/discussion-benners-theory-novice-expert/.
Project Questions
6
Research Questions
1. What knowledge of depression do licensed nurses and CNAs working in
nursing homes possess prior to reviewing the educational PowerPoint?
2. Can an educational presentation over depression increase the recognition of
depressive symptoms in nursing home residents by nursing home licensed nurses
and CNA staff?
3. Does a higher educational level of licensed nurses and CNAs have a positive
correlation with increased knowledge of depression?
Sub-Research Question
1. Can nursing home licensed nurses and CNAs identify risk factors of
depression?
Definition of Key Terms/Variables
Nursing home – A public or private residential facility providing a high level of
long-term personal or nursing care for persons (such as the aged or the chronically
ill) who are unable to care for themselves properly (Nursing home, 2021).
Resident – a. living in a place for some length of time b. one who resides in a
place (Resident, 2021).
Elderly – a. of, relating to, or characteristic of later life or elderly persons b.
individuals over 65 years old (Elderly, 2021).
Depression – A mood disorder marked especially by sadness, inactivity,
difficulty in thinking and concentration, a significant increase or decrease in
appetite and time spent sleeping, feelings of dejection and hopelessness, and
sometimes suicidal tendencies (Depression, 2021).
7
Licensed Nursing Staff – Referring to Registered Nurses (RN) and Licensed
Practical Nurses (LPN).
CNAs – Referring to Certified Nurses Assistants.
Conceptual Implications
Conceptual definitions are crucial in research since they help in the
development of causal relationships between variables. These constructs will help in the
simulation and understanding of various outcomes in the research. The study focused on
the role of the nursing home nursing staff and their contribution to detection of elderly
depression. This atmosphere is defined from a different perspective, and there are
multiple variables, that affect the physiological and psychological outcomes for the
elderly and which can be associated with increased or decreased levels of depression. For
example, the nursing home environment can be described by social support, which is
four-dimensional. The four functions of societal support for nursing homes include
emotional appraisal, belonging, self-esteem, and physical support. These forms of support
involve nursing staff training on the risk factors of depression. Also, informational
support deals with education competencies that influence the ability of nursing home staff
to recognize and treat depressive disorders.
Moreover, social interactions and affection contribute to positive outcomes in
nursing home experiences. The elderly are faced with the issue of social withdrawal
which can contribute to psychological distress. The occurrence of depression and anxiety
in the old is considered a nonspecific and negative human state. Based on the structural
equation model, which is used in relationship analysis, low levels of social interaction
and the complete lack of informational and emotional support are likely to increase the
8
level and rate of psychological distress among this population. Therefore, nursing home
staff should understand the bidirectional nature of the relationship between social support
and the incidence of depressions and other forms of psychological distress.
A study by Sawyer & Dykema-Engblade (2016) indicated a causal relationship
between the home environment and design and its effect on companionship, social
interaction, and independence among the elderly. The disengagement theory asserts that
nursing homes lead to social withdrawal, inactivity, lack of functionality, and other
actions, which lead to distress (Hollis-Sawyer & Dykema-Engblade, 2016). The
improvement of the nursing home setting is significant for depression patients. A relevant
variable, in this case, is access to outdoor space, which helps improve depressed
individuals’ condition (Trueland, 2017). Outdoor spaces account for the unaccompanied
visits to gardens and outside regions for nursing home patients. The inability to access
outdoor spaces affects mood, and can increase irritability, anxiety, and other depression
symptoms (Trueland, 2017).
Logic Model of the Proposed DNP Project
Illustration of the Relationship between Proposed Project Concepts
A logic model is an evaluation tool used by program managers to describe and
illustrate the effectiveness of the program (Simning & Simons, 2017). The tool creates
logical links between project concepts, resources, output, audience, and the specific
outcomes in the project. In this case, the project is the improvement of the elderly’s
experiences in nursing homes through proper training and education for the staff as well
as the improvement of the facility’s environment to reduce the occurrence of depression.
The utilization of evidence-based practices and methods are significant in the project
9
since modern healthcare relies on research and evidence in the treatment and
management of various conditions.
The logic model relies on several processes, which enhance the performance of
the various resources or input towards the project. The first phase in the project was to
locate the most reliable evidence to support the proposed study. This phase is achieved
through the creation of PICOT which is a clinical question statement focused on
identifying the right audience and the expected outcomes of the project. The acronym
PICOT is representative of population, intervention, comparison, outcome, and time. For
example, the population is the elderly seeking support from nursing home facilities. In
this scenario elderly is descriptive of old adults from the age of 65 and above. The
population suffers from depression due to the various conditions of the nursing home
environment and inadequate training among the staff, which leads to overtreatment and
under-treatment of depression patients. The intervention, in this case, was the use of
screening methods and patient feedback that is crucial in improving patient outcomes and
experiences in the nursing homes. The outcome of the project is the proper treatment and
management of depression among the elderly in nursing homes. Depression in a nursing
home environment is a health issue that requires an evidence-based approach.
Analysis of evidence is crucial in the appraisal of the project and the use of the
proper literature to support the project requirements. Literature and theoretical backing
promote reliability and recommendations from the relevant stakeholders. The
confirmation that depression is misdiagnosed, undertreated, and over treated in nursing
homes calls for a different choice of screening techniques and tools. For example, the use
of the Pre-Admission Screening and Annual Resident Review (PASARR) system

10
increases the reliability and validity of assessing for depression in elderly patients
admitted to nursing homes (Lantz, 2019). Also, the Patient Health Questionnaire-9
(PHQ-9) screening tool is appropriate in assessing the level of distress and other forms of
impairment in aging and depressed patients (Levis, Benedetti, & Thombs, 2019). In
essence, the use of proper tools in the recognition and treatment of depression helps the
nursing home staff manage the condition in elderly subjects.
Depression in nursing homes poses new challenges and demands for staff and
nursing professionals. The project is meant to change the nursing home environment and
the approach to the acknowledgment and handling of depression among the old by
enhancing licensed nurses and CNAs ability to recognize symptoms. The use of reliable
techniques such as the PHQ-9 screening tool helps recognize the positive symptoms of
depressive ailments in the aged (Levis et al., 2019). The proper recognition of symptoms
leads to the identification of the appropriate treatment plan. The determination of the
treatment strategy relies on the severity of the condition. Nursing home staff influence the
psychotherapeutic or the pharmacological approach in the treatment of depressed
patients. These amenities are long-term care facilities, and the care settings should be
well equipped to deal with a heterogeneous population. This idea means that facilities and
treatment plan should adapt to low and high-reliance patients in nursing homes. For
example, the creation of high-dependency facilities helps the elderly and staff deal with
the increasing need for care and support. In essence, nursing home staff should be
equipped with the right personnel and equipment to aid in the recognition of depressive
disorders as well as treatment.

11
Part of the treatment plan involves the educational training of licensed nurses and
CNA staff. The nurses in long-term care facilities receive extensive training on the
administration and interpretation of PHQ-9 for the patients. The rating scales from this
tool are crucial in the adherence to treatment schedules. Nurses are vital to decision
making; thus, their contribution to the treatment of depression is an incentive to nursing
homes and the healthcare system to provide education opportunities for their nursing staff
on depression. Depression is a leading cause of disability and major contributor to disease
burden worldwide. Treatment of depression is key to improving the overall wellbeing of
afflicted patients (WHO, 2018).
The Agency for Healthcare Research and Quality (2018) asserts that patient care
and safety are crucial to nursing homes. Training modules focus on the home conditions
and the patient status, which in turn reduces injuries and other adverse outcomes such as
patient suicides. Theoretical perspectives assert that the occurrence of depression for the
elderly is attributed to social withdrawal and decreased physical activity that hinders the
patient’s autonomy (AHRQ, 2018). Therefore, different training modules for nursing
home staff are centered on professional education and the interaction between the patient
and the environment.
The project’s focus was on the improvement of patient outcomes in nursing
homes. Appreciation and dealing with depression rely on the improvement of preparation
and teaching of the nursing home licensed nurses and CNA staff in these facilities. The
primary focus of the logic model is an explanation of the integration and maintenance of
change in nursing practice. To implement change in nursing, there is a need to
communicate the recommendations to the relevant stakeholders. The involvement of the

12
stakeholders helps in assessing the organization’s standards and the alignment of goals.
Quality reviews are part of the integration process since they monitor and evaluate the
outcomes. For nursing homes, the training of personnel is crucial in the attainment of
positive patient outcomes and a reduction in cases of depression.
Figure 2.
Logic Model of Scholarly Project:
Note: This model shows the possible assumed outcomes if management and staff
are educated using best evidence-based practice. The perceived end result is decreased
mortality and increased quality of life.
Chapter Conclusion
Depression is prevalent in nursing homes. The nurses and staff in nursing homes
fail to recognize and treat depressive conditions since elderly patients have different
physical, cognitive, and mental needs than younger patients. To improve the living
conditions of the elderly in nursing home setting, there is a need to improve the
techniques used in the detection, as well as treatment of depression patients. The failure

13
to recognize and treat depression can lead to devastating effects on the patients.
Depression among the elderly is attributed to multiple disorders such as anxiety,
cognitive impairment (dementia), and other conditions that subsequently reduce the
quality of life. Unattended depressive disorders can increase risk of mortality and other
impairments in the patients. The elderly suffers deficits in self-care, and nursing home
staff should engage in the practices to avoid a downward spiral in depression symptoms.
In essence, depression in nursing homes is a significant health concern that requires
nursing intervention in the treatment and management of the condition.
As a mental and psychological condition, depression in nursing homes is often
underdiagnosed or over-treated. The application of the logic model helps in the
identification of proper techniques and tools to recognize of depression symptoms. The
nursing home staff should be able to screen and interpret the scales in depression
measures. Besides the treatment, these professionals require education regarding
recognition of the symptomology of depression. Nursing education and training is a
significant part of transforming nursing homes since it helps in the management of the
condition as well as ensuring patient safety and general wellbeing. Therefore, education
programs should be encouraged to ensure staff in these facilities are well-informed and
properly equipped with the knowledge to attend to the elderly population appropriately.
In the process, the elderly will have a platform for managing conditions associated with
depression.

14
Chapter II
Literature Review
Depression has been identified as one of the most notorious illnesses afflicting
people of all ages, especially the elderly. In particular, studies in mental health of the
elderly demonstrate that the highest rates of depression exist among the elderly living in
nursing homes and long-term care facilities (Kaushal et al., 2019). Adding to the
challenge of the high prevalence rate of this condition among the elderly is the high rate
at which it goes undetected and eventually untreated, causing high mortality and
morbidity rates, increased suffering among these people, and the development of suicidal
feelings. For that reason, the topic of late-life depression has been extensively researched
in the literature. This literature review was broad to gain insights into the nature of
depression among adults residing in nursing homes. The literature review will discuss the
scope of depression among the elderly in the entire population, the details about the
increasing rates of depression among the elderly, and the treatment failures and gender
differences as contributors to the late-life depression of these people when taken to
nursing homes. The literature review will also investigate the scope of education for
nursing home staff focusing on CNAs particularly as licensed nurses are required to pass
a national exam that assesses knowledge of essential nursing care.
Search Parameters

15
The literature review includes information from several databases and websites.
The primary search engine utilized is Pittsburg State University’s Axe Library Summon.
Searches were limited to full text, peer reviewed, and published in the last 5 years.
Searched terms include: depression, depression knowledge test, nursing home depression,
long term care depression, elderly depression, depression education, depression screening
tools, nursing home staff education, CNA education, CNA training, and CNA
qualifications.
Scope of Depression Among the Adults
The rates of depression and suicide among the adults living in the United States
has been on the upward trend, whereas the age at which major depression occurs is
steadily decreasing (Giri et al., 2016). This trend has been in existence for the past few
years, even though new, better, and safer-tolerated medications have been discovered. In
fact, Gonyea et al. (2018) estimated that a significant proportion of adults in the United
States, approximately one in six people, including the elderly will experience a
depressive disorder or have depressive symptoms before the year 2020 comes to an end.
Existing statistics on lifetime prevalence of depression differed from one study to
another. For example, Weinberger et al. (2018) reported that the lifetime prevalence of
depression stood at between 2.5 and 5 percent among males while it was between 6 and
11.9 percent among females. At the same time, Weinberger et al. (2018) reported the
lifetime prevalence of lifetime depression for an extreme depressive condition was at
about 10 percent among both females and males. Also, Weinberger et al. (2018) noted the
lifetime prevalence rate for a significant depressive condition alone stood at about 18
percent, thereby translating to approximately between 30 and 33 million adults.

16
Existing studies indicate that the state of depression among the elderly differs, but
most adults are neither severely depressed nor demented. Zalavadiya et al. (2017) carried
out a cross-sectional study in Western India to compare the epidemiological factors
related to depression among the elderly residing in nursing homes. They discovered that
the elderly admitted to nursing homes were more depressed than those in the community
health facilities. At the same time, it was established that older age people, especially
those with a history of addiction, impaired sleep, lack of prayers, absence of recreational
activities, as well as those with weaker family ties, had higher chances of being
depressed. More health complaints were found among people who were depressed
compared to those who were not. In a different study carried out by Giri et al. (2016), it
was established that physically healthy adults have the lowest rates of substance abuse,
anxiety, and depression. Nevertheless, Mitchell et al. (2017) differed with these findings
and noted that of the over 30 million elderly in the United States, nearly 5 million of them
suffer from chronic and frequent depressive conditions despite health-related factors.
Increasing Rates of Depression Among the Elderly
As the global population ages rapidly, so does the rate of depression among
elderly people. In a cross-sectional study, Chauhan et al. (2016) attempted to establish the
prevalence rates of depression among elderly individuals living in India. By using the
semi-structured questionnaire to assess the risk factors and socio-demographic
characteristics of depression, the researchers discovered that of the 290 elderly people
who responded to the questionnaire, nearly 9.3 percent of them were depressed. At the
same time, it was established that depression was significantly correlated with the

17
physical dependence for daily lives, economic interdependence, co-morbid conditions,
and increased age.
In a different study, Kaushal et al. (2019) studied the increasing rates of
depression among elderly people staying in nursing homes. According to these
researchers, India has witnessed a rising population of the elderly. The statistics they
quote reveal the country now has over 104 million people with the elderly population
growing from approximately 12 percent in 2015 to an estimated 22 percent by 2050. For
this reason, upon carrying out a systematic review, they discovered the prevalence of
depression among the elderly population stands at 21 percent because of factors such as
financial dependence and illness loneliness which make them more prone to depression in
comparison to the total population. Therefore, in order to examine the frequency of
depression among the elderly people staying in nursing homes, the researchers randomly
chose 3 homes from which 50 elderly people were selected by means of a random
sampling technique. The results of this study indicated that more males exhibited high
rates of depression compared to their female counterparts who showed mild depression.
At the same time, it was reported that those participants who were financially dependent
had higher depressive symptoms than those who were independent with higher rates of
this condition being reported among residents living in old age homes.
It is apparent that the depression rate is greatest among the elderly population
staying in long-term care facilities. Some scholars, such as Erdal et al. (2017) reported
that nearly 59 percent of the elderly staying in nursing homes were depressed and other
researchers such as Perkkiö et al. (2019) reported a prevalence rate of a significant
depressive symptom was at 14.4 percent with the incidence of a minor depression being

18
16.8 percent. In addition to those elderly people already having depression, studies
reported another 15 percent of the geriatric patients living in long-term care facilities
show depression symptoms but did not meet the criteria for being identified as having a
significant sign of depression. Some scholars have referred to such depressive symptoms
as minor depression, which contributes to disability and distress since significant
depression is often overlooked by medical practitioners.
Women and Depression
It is evident in the literature that the highest rates of depression are reported
among women. Ali et al. (2019) found nearly 50 percent of people residing in nursing
homes are women and display depressed symptoms upon being admitted to the nursing
homes or long-term care facilities. During the middle-aged span of life, Cornish et al.
(2017) acknowledge that women experience depression at twice the rate at which their
male counterparts experience it. A study carried out by Kuehner (2017) demonstrated the
proportion of women suffering from depression was greater than the proportion of men
experiencing depression. The same study revealed the rate of dysthymia among women
was greater than that of men. At the same time, studies have found out that women are
five times as likely as men to experience depression after being injured. For instance, the
study by Kuehner (2017) indicated that women are twice as likely as their male
counterparts to be depressed after myocardial infarction. In addition, it is thought that
women are at a higher risk of having recurring and long-lasting depression.
Primary Care and Depression
Through the frequency of depression among adults admitted in the primary care
facilities, and among the studies that were reviewed in this study, it was established the

19
incidence of depression was not greater among the elderly than among younger people.
As out-patient older adults start aging, it is revealed that they would require admission in
long-term care facilities at some point in their lives. It was discovered that among the
elderly admitted in primary care facilities, about 10 percent of them meet the criteria for
having a significant depression symptom, with another 30 percent demonstrating the
presence of significant depressive symptoms that need further diagnosis and treatment
(Pramesona & Taneepanichskul, 2018). Other studies have investigated patients admitted
to primary care facilities and discovered there was a high percentage of depression
among people exposed to primary care facilities (Erdal et al., 2017).
Treatment Failure and Cases of Depression
The subject of chronic depression and treatment-resistant depression has gained
momentum in the past few years and has increased the influence of human suffering as
most people have been identified as being non-responsive to treatment. As a result, this
problem has raised the eyebrows of medical practitioners as those people who become
resistant to medication grow old eventually, thereby contributing to the growing number
of elderly people being identified as being depressed. Long-lasting types of depression
include illnesses, such as recurrent depressive disorder, double depression, dysthymic
disorder, and major depressive disorder. Garay et. al (2017) discovered a significant
proportion of depressed people fail to respond adequately to medicines even when they
are given adequate dosage. Among those who were unable to respond to medication,
approximately 26 percent of them were utterly non-responsive.
Elders in Nursing Homes

20
Research demonstrates the incidence of depression is relatively high among the
elderly admitted to nursing homes or long-term care facilities. Studies have shown that
among the elders living in nursing homes, up to 78 percent of them have incidences of
depression (Levin, et al., 2007). In addition to those elderly people in nursing homes
reporting rates of depression, almost 15 percent of them have significant depressive
symptoms that demand further studies. In another study, Damian, J. et al. (2017) reported
a high percentage of the elderly admitted to the nursing homes showed signs of
depressive symptoms.
Contributors to Late-Life Depression
Depression is now regarded as one of the most treatable illnesses, with nearly half
of the patients treated for the condition reporting decrease in their depressive symptoms.
Discrepancies have been noted between the provision of treatment and the availability of
treatment options within disadvantaged populations, a significant causative factor for the
rate of under treated depression (Levin, et al., 2007). While there is a high prevalence rate
of behavioral and psychiatric problems among elderly people residing in nursing homes,
most of these people do not always get adequate mental healthcare services they deserve.
The Patient Health Questionaire-9 (PHQ-9) is a contributor to mental healthcare
inadequacy in nursing homes (Juman & Figlerski, 2017). The PHQ-9 is an evidence-
based tool, but the data is self-reported by the patient, which can lead to misinformed
assessments when the tool is administered by staff that can be spread thin due to staffing
limitations (Juman & Figlerski, 2017).
The shortage of mental health providers is another factor contributing to under
diagnosed and under treated late-life depression. In the United State for example, there

21
have been different incentives or disincentives that have immensely affected the
availability of mental health services to Americans (Ashcroft et al., 2014). Adequate
training and financial aspects of mental health care can be both incentives and
disincentives for treatment depending on the viewpoint of the stakeholder. Improved
training gives the healthcare worker a better understanding of mental health issues, but
there is time to educate and the cost of education that also must be factored in (Ashcroft
et al., 2014).
Impacts of Depression
If depression goes untreated, it can cause other physical and psychological
disorders and can even lead to death. Researchers such as Nelson and Spyker (2017),
explained undiagnosed and untreated depression hastens disability and worsens physical
symptoms. Additionally, Chauvet-Gelinier and Bonin (2017) stated depression increases
the risk of cardiac mortality in victims with or without cardiac illnesses in the first place.
Other researchers who studied the same topic discovered the risk for cardiac death was
twice as high in significant depressive symptoms just as it is for the minor depressive
symptoms. At the same time, studies have demonstrated that elderly people aged over 65
years have higher chances of committing suicide when compared to other age groups. For
example, the study by Chatterjee et al. (2017), noted that the highest suicide rate among
the elderly occurs mostly among the oldest people in this age group with increased
incidence among people aged 85 years and older. Thus, in addition to hastening
disability, depression also increases the chance of depressed individuals to commit
suicide.
Depression Education for Policy Change in Nursing Homes

22
The findings from the literature indicate that there is a lack of knowledge among
healthcare providers in late-life depression. Continuous educational sessions in this area
are warranted for healthcare workers, especially those in nursing homes. In fact, existing
evidence indicates that a lot has been done in this area on how depressed patients can use
personal support services to reduce the symptoms of depression. Existing studies have
concentrated on nurse-led depression education among the elderly in nursing homes as
well as collaborative teaching to help depressed individuals manage depression. Notably,
Abrams et al. (2016) conducted research on a training program meant to improve
understanding of depression in long-term care facilities and nursing homes. The aim of
this study was to refine the current training initiative for nurses working in nursing homes
and provide evaluative knowledge. In this study, three major training modules offered a
summary of the symptoms of depression. Then researchers used paired t-tests and chi-
square tests to assess change in knowledge. It was established that those who participated
in the study gained increased knowledge in the detection, recognition, treatment
practices, and differential diagnosis for those individuals at risk for developing depressive
challenges.
In addition to a training program, interventions such as religion can be used as a
useful intervention to help depressed elderly people in nursing homes. For example,
Pramesona and Taneepanichskul (2018) carried out a study to assess the influence of the
spiritual intervention on value of life and depressive symptoms among the elderly
residing in nursing homes based in Indonesia. In particular, the researchers prepared a
quasi-experiment utilizing repeated measures. The researchers recruited up to 60 elderly
people admitted to three nursing homes in Indonesia with a scale of 5 to 11. Notably,

23
these participants were recruited and the purposely assigned to a religious group for
intervention. The main result was depression measured using a questionnaire on a scale
of between 5 to 11. Importantly, it was established that there was a significant decrease in
depressive scores after the participants were exposed to an intervention plan for
approximately 12 weeks. The researchers ended up concluding that religious-based
intervention was a helpful tool in plummeting symptoms of depression among elders
residing in nursing homes.
Licensed Nurse and CNA Education and Training
Licensed nursing staff must complete an accredited program and pass a national
board exam to work as a Licensed Practical Nurse (LPN) or a Registered Nurse (RN).
LPN programs can be completed in approximately one year while RN programs can be
completed in two years for associate degree or four years for bachelor’s degree. LPN or
RN educational programs must meet specific criteria to become accredited. An accredited
nursing program adheres to national standards. These standards include requirements for
psychological content which includes information on depression.
CNA training, while still important, is less rigorous and the variances between
states can be very significant. The states board of nursing sets the education requirements
for CNA programs. Federal regulation requires a minimum of 75 classroom and clinical
hours ("State Nurse Aide Training: Program Information and Data", 2002). Certified
Nurse Aide training can vary depending on the organization offering the training due to
the vague parameters set forth by the state. The Kansas Department for Aging and
Disability Services (2021) CNA instructor manual outline training targeting basic ADL
needs with vague psychiatric education concerning “dementia and problem behaviors.”

24
Trinkoff et al. (2017) notes that training requirements between states influences patient
outcomes in nursing home. There is a positive correlation with nursing homes in states
with higher education requirements and better health outcomes for the elderly (Trinkoff
et al. 2017).
Delivery of Education
Current training methods of nursing home facilities is a factor that needs to be
considered, but it is also important to consider the method of education delivery as the
primary goal of this project is to develop and administer education to improve the
recognition of depressive symptoms with the anticipated effect of improving depression
outcomes. The use of a video presentation, PowerPoint presentation, or oral presentation
are all viable options of providing education but is one method more effective than
another? The method of education delivery can be just as important as the material being
presented. If the method of delivery does not resonate with the intended audience, the
retention of material can be put into question.
The literature has sparse information relating to the training methods used by
facilities to educate their staff on depressive symptoms. Beuscher and Dietrich (2016)
performed a pilot study analyzing the aftereffects of staff recognition of depression
following a focused training course. Their study found that staff knowledge of depression
increased, however, recognition of residents with symptoms of depression did not
increase. Bing-Johnson et al. (2016) found that competence with nursing home care has a
positive correlation with level of training with RNs being most competent and support
staff being least competent. Beuscher and Dietrich (2016) note that staff expressed a

25
desire for more information relating to depression following their training which could
relate to improved recognition of depressive symptoms if provided.
One aspect to consider with education delivery methods is whether the intended audience
is familiar with the medium. Moulton, Türkay, and Kosslyn (2017) as well as Alpert and
Hodkinson (2019) found that students were more accepting of the learning process when
utilizing familiar formats although it did not relate to improved understanding of the
subjects presented. Overall, little difference in knowledge acquisition has been found
when comparing video presentations and PowerPoint presentation formats. Although a
newer education tool, Prezi has been found to be increasingly effective as an education
tool and has had more favorable results than other presentation methods (Moulton,
Türkay, & Kosslyn, 2017; Safar, 2015). Prezi is an educational tool that allows the
presenter to present information in a non-linear format which causes the audience to be
more engrossed in the learning process stimulating thought processes (Safar, 2015).
However, cost must be a factor when considering presentation methods and Prezi is an
expensive option.
Chapter Conclusion
Overall, there is no doubt that depression is one of the most common illnesses
inflicting people of all ages, especially the elderly. In fact, studies in this area have
demonstrated that the highest rates of depression exist among the elderly living in nursing
homes. In addition to the fact that depression is exceedingly prevalent among the elderly
in nursing homes, reviewed studied revealed that it goes undetected and eventually
untreated, causing high mortality and morbidity rates, increased suffering among these
people, and development of suicidal feelings. The literature review offers insights into the

26
intricate nature of depression among adults residing in nursing homes. The review of the
literature provides discussing the scope of depression among the elderly in the entire
population, then moved to study the prevalence rates of depression among the elderly and
then a discussion on the gender differences as contributors to late-life depression of these
people when taken to nursing homes.
It was noted that depression, suicides, and depression among the adult, especially
those living in the United States of America have been on the upward trend. Thus, it was
apparent that as the global population ages rapidly, so does the rate of depression among
elderly people. While depression affects people from all genders and races, it was
determined in the literature review that the highest standards of depression are reported
among women compared to men. It was also noted that a shortage of mental health
providers is a significant factor contributing to late-life depression.
27
Chapter III
Project Design
The purpose of this project was to ascertain whether providing education to
licensed nurses and certified nurse aide staff in nursing homes results in an increased
awareness and recognition of depression and depressive symptoms among the nursing
home population. A descriptive research design was used to identify knowledge of
nursing staff in long-term nursing home facilities before and after depression and
depressive symptom education.
Methods
The study utilized a one-group pre-test/post-test design with nursing home staff
that interact with nursing home residents during a normal workday. Demographic data
was obtained related to gender, age, ethnicity, education, and employment status. The
method of data collection selected is chosen to compare pre-test scores and post-test
scores following an educational presentation regarding depression and depressive
symptoms. Participants were invited to participate in a pre-test depression knowledge test
(See Appendix B) constructed and utilized by Gabriel & Violato (2009) that was adopted
for this study. A presentation was developed with Microsoft PowerPoint by creation of a
voice-over presentation (See Appendix C) and converted to a Youtube video. The pre-test
28
was administered prior to the depression education intervention and the post-test (See
Appendix B) was administered following the depression education.
The pre-test/post-test was administered using Google Forms on the internet. The
educational presentation was accessed through a YouTube video embedded into Google
Forms. Instructions were provided for all participants to access and complete the pre-test,
watch the PowerPoint presentation, and then take the post-test at the appropriate web
address. The end goal is for the results of the project to be utilized to improve nursing
home staff education throughout multiple facilities. The development of a short
educational presentation can be essential to help staff recognize untreated depressive
symptoms in nursing home populations. Effective educational material that is cost
effective could help reduce medical costs by treating symptoms before they manifest into
more serious conditions.
There are many research designs that can be utilized to study phenomena. A
descriptive research design, utilizing a survey method, will produce quantifiable data for
statistical analysis (Aggarwal & Ranganathan, 2019).
Project Questions
Research Questions
1. What knowledge of depression do licensed nurses and CNAs working in
nursing homes possess prior to reviewing the educational PowerPoint?
2. Can an educational presentation over depression increase the recognition of
depressive symptoms in nursing home residents by nursing home licensed nurses
and CNA staff?
29
3. Does a higher educational level of licensed nurses and CNAs have a positive
correlation with increased knowledge of depression?
Sub-Research Question
1. Can nursing home licensed nurses and CNAs identify risk factors of
depression? (See Appendix B survey questions 2,4,5,6,8,9)
Project Site and Population
The study was conducted at three Southeast Kansas nursing home facilities. The
pre-test/post-tests were adopted from a tool available through open access research
performed by Gabriel and Violato in 2009. Convenience sampling was employed for the
staff participating in the project and the number of participants was determined by the
available staff at each facility with 30 subjects participating in the study. Licensed nurses
and CNA participants were included in the study if they were between the ages of 18-60
and have direct interaction with nursing home residents during their normal workday.
Participation in the study was voluntary and participants received no
compensation. It was expected for individuals to complete the pre-test survey, receive
education on depression, and then complete the post-test survey during the same day.
Participants were advised that they may remove themselves from the study at any time
without fear of reprisal.
Data Collection
Measurement Instruments. The pre and post-tests were adopted from the
Depression Knowledge Test (DKT) that was developed by Gabriel and Violato in 2009.
The DKT was created by Gabriel and Violato (2009) to assess the knowledge level of
healthcare workers and patients with depression. The DKT consists of 27 multiple choice
30
questions in total ranging from general presentation of depressive symptoms to
confounding issues in depressed individuals. The DKT was used in its entirety and no
changes were made to the tool.
Ethical Considerations/Protection of Human Subjects
Participants had to volunteer to contribute to the study. The benefits and risks of
the study were provided to each study participant prior to initiation. Identifiable data was
not collected. Study participants were nursing staff of nursing homes that have direct
contact with the residents of the facility. The three basic principles of human subject
protection (respect for persons, beneficence, and justice) were observed. IRB approval
was obtained from the School of Nursing and the Pittsburg State University IRB
committee prior to conducting study and interacting with study participants. Written
approval to complete the study in the three nursing home facilities was also obtained
before implementing the project.
Data Analysis
Reliability and Validity. The educational presentation was developed through a
review of the most recent literature regarding the subject. The DKT was found to produce
a Cronbach alpha of 0.68 for internal consistency reliability and was determined to have
content and convergent validity (Gabriel & Violato, 2009). Cronbach alpha is a measure
of internal consistency or reliability of a set of test items (Goforth, 2015). Goforth (2015),
from the University of Virginia states, “methodologists recommend a minimum alpha
coefficient between 0.65 and 0.8” for a measure to be considered “good” with higher
alpha coefficients conferring higher reliability.
31
Analytical Methods. Demographic data was analyzed using descriptive
statistics: number of subjects, educational level, gender, age, and ethnicity. A paired t-test
for summative average was performed using SPSS software to compare average scores of
survey responses pre- and post-depression education.
Timeline
Data collection began upon approval from the IRB committees and concluded
once 30 pre and post-tests had been obtained. Introductory sessions were held at nursing
homes in the southeast Kansas area to introduce the author of the study and explain the
process of accessing the pre-test, educational presentation, and post-test to volunteer
participants. Data analysis was conducted once participants had completed the pre-test,
educational presentation, and post-test. No identifying factors were included in the
reporting of data. No compensation was provided to participants or participating
facilities.
Assumptions
Multiple assumptions are made for this project. It is assumed that licensed nursing
and CNA staff working at nursing homes in Southeast Kansas have undergone education
and training to be employed in their current position. It is also assumed participants
answered test questions honestly and to the best of their ability.
Budget
Time was an expense for introduction of the study to potential participants at
participating nursing home facilities. Participants incurred no monetary cost by
participating in the study. Participants and nursing home facilities were required to
32
donate time for introductions, explanation, and completion of the educational
presentation and testing of the study.
Strengths and Weaknesses
Strengths of the study are in the use of a pre-test to determine current level of
knowledge of participants compared to the post-tests following educational presentation
to determine knowledge gained. Another strength of the study is the voluntary nature of
participants as they are motivated by their own interests rather than influence of this
researcher. Also, internal validity can be undermined by having no control group. Other
potential weaknesses are the educational level of the study participants as well as their
ethnic/cultural background, all of which can influence a participant’s perception of
depression.
33
Chapter IV
Findings
Introduction
The purpose of this project was to help determine whether providing education to
licensed nursing and CNA staff in nursing homes results in an increased awareness and
recognition of depression and depressive symptoms among the nursing home population.
The project was approached by administering an anonymous pretest/posttest survey
through Google Forms. Participants were informed that they may stop participating at
any time during the survey and no data from incomplete forms was used for the project.
The anonymous survey included demographic questions, multiple choice questions, and a
short educational PowerPoint.
Demographics
The survey was offered to licensed nursing and CNA staff at three Southeast
Kansas nursing homes. Staff at the participating facilities were informed of the study by
the researcher. Information regarding the study and with directions of how to participate
were posted at the time clocks with facility administration permission. Staff who were
present during the site visits were encouraged to inform co-workers of the study to reach
the maximum number of potential participants in the facilities. The combined clinical
staff population for all three facilities was 212. Site visits were concluded on June 15
th
,
34
2021. First data was collected on June 17
th
, 2021, and the final data collected occurred on
June 29
th
, 2021. Data collection concluded when 30 participants completed the survey.
Demographic data collected from participants included their age, education level, gender,
ethnicity, and employment status. Demographic data is presented in Table 1.
Table 1.
Demographic Data
(N=30)
Characteristic
n
%
Gender
Male
1
3.3
Female
29
96.7
Ethnicity
Caucasian
26
86.7
Hispanic
4
13.3
Age
18-24
7
23.3
25-34
9
30
35-44
11
36.7
45-54
2
6.7
55-64
1
3.3
Education
Some High School
2
6.7
High School
Graduate
11
36.7
Vocational
Training
10
33.3
Associates Degree
4
13.3
Bachelor’s Degree
1
3.3
Other
2
Employment
Full Time
27
90
Part Time
2
6.7
PRN
1
3.3
Note. This table illustrates the demographic breakdown of participants within the
characteristics of gender, ethnicity, age, education, and employment status. The left
column denotes the number of participants in the respective category. The right column
denotes the percentage of the sample population for the respective category.
35
Description of Key Variables
The primary goal of the study was to determine the depression knowledge of
licensed nursing staff and CNA’s while also measuring if there was an increase in
depression knowledge following an educational PowerPoint presentation. Current
knowledge was measured with a pre-test. Any increase in knowledge was measured with
a post-test following the educational PowerPoint. The dependent variable is the
depression knowledge of licensed nursing and CNA staff, and the independent variable is
the educational PowerPoint.
Pre-test and Post-test
Participants of the study were provided a pre-test immediately prior to an
educational PowerPoint followed immediately by a post-test. Scores were only collected
once all questions in the pre-test and post-test were answered. Participants who did not
complete the pre-test and post-test were not included in the study results. Test scores
were anonymous with the only identifier being the order in which results were collected.
Both pre-test and post-test contained the same 27 multiple-choice questions. One of the
multiple-choice questions asked the participants to “select all that apply” this resulted in
the highest possible score for both the pre and post-test being 28. The educational
PowerPoint presentation was approximately 12 minutes in length.
Research Question Results
Research question one, What knowledge of depression do licensed nurses and
CNAs working in nursing homes possess prior to reviewing the educational PowerPoint?
sought to determine the current knowledge of depression that licensed nurses and CNA’s
working in a nursing home possessed prior to reviewing the educational PowerPoint. The
36
testing instrument has an established standard of 78.7% for participant satisfactory
performance established by Gabriel and Violato (2009). Pre-test scores ranged from 10-
27 correct answers out of a possible 28 correct answers. A total of 16 of the 30
participants (53%) achieved a pre-test score of 22 or greater representing satisfactory
performance. The mean pre-test score was 22.4 with a standard deviation of 3.45014. An
average of 80% was achieved by the participants on the pre-test.
Research question two, Can an educational presentation over depression increase
the recognition of depressive symptoms in nursing home residents by nursing home
licensed nurses and CNA staff? sought to determine if the educational presentation over
depression would increase the recognition of depressive symptoms in nursing home
residents by nursing home licensed nurses and CNA staff. A one tailed test design was
appropriate for this study to measure the one directional effect of post-test scores
following an educational presentation (Birkett, 2020). Post-test scores ranged from 20-27
correct answers out of 28. A total of 26 of the 30 participants (86.6%) achieved a pre-test
score of 22 or greater representing satisfactory performance. The mean post-test score
was 24.2333 with a standard deviation of 1.95965. An average of 86.5% was achieved by
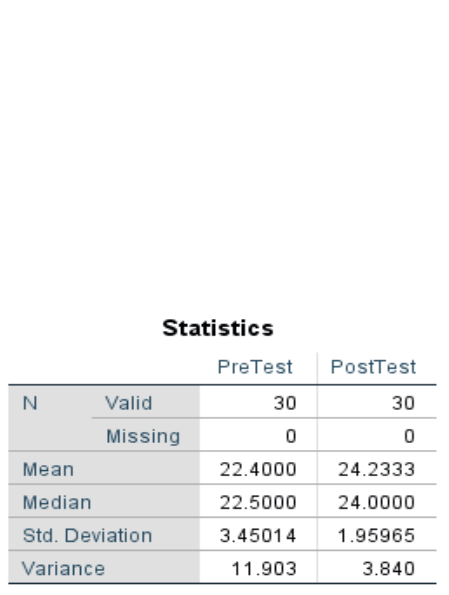
the participants on the pre-test. Tables 2, 3, and 4 illustrate these findings.
Table 2. Pre and Post-Test Side by Side Comparison

37
Note. This table displays the mean, median, standard deviation, and variance of the pre
and post-test.
Table 3. Pre-test Results Histogram
Note. This table displays pre-test scores and the frequency scores occurred within the
sample population.
Table 4. Post-test Results Histogram
Note. This table displays post-test scores and the frequency scores occurred within the
sample population.

38
A paired samples t-test is used to compare the means of two measurements taken
from the same data source (Kent State University Libraries, 2021). Data requirements
must be met for a paired samples test. According to Kent State University Libraries
(2021), the dependent variable must be continuous, subjects in both groups must be the
same, the data is obtained from a random sample of the population, there is a normal
distribution of the difference between the paired values, and there must be no outliers in
the difference between the two groups. Determining the presence of outliers in the data
must be done to determine if data should be excluded. A boxplot is a standardized way of
viewing the distribution of data and can help identify if there are outlier values. An
outlier is a value that differs substantially from the rest of the data. A boxplot for pre-test
and post-test data is displays in Table 5. The pre-test score of 10 is identified as an outlier
in the pre-test data.
Table 5. Boxplot of Pre-test and Post-test.
Note. This table displays the distribution of scores on the pre-test and post-test. The pre-
test score of 10 is identified as an outlier.

39
A paired samples t-test was performed to determine significance of post-test
scores following the educational presentation. The participant’s data with the outlier
score of 10 on the pre-test was omitted for the paired samples test. The critical value for t
distribution with 28 degrees of freedom is 1.701. The paired samples test for the pre-test
and post-test scores produced a t value of 3.449. The p value of the paired samples test is
less than 0.05. The data indicates a statistical significance between pre-test and post-test
scores (t28=3.449, p<0.001). The paired samples t-test is displayed in Table 6. A
comparison of pre and post-test scores is displayed in table 7.
Table 6. Paired Samples t-Test
Note. This table displays the paired samples test results for the pre and post-tests.
40
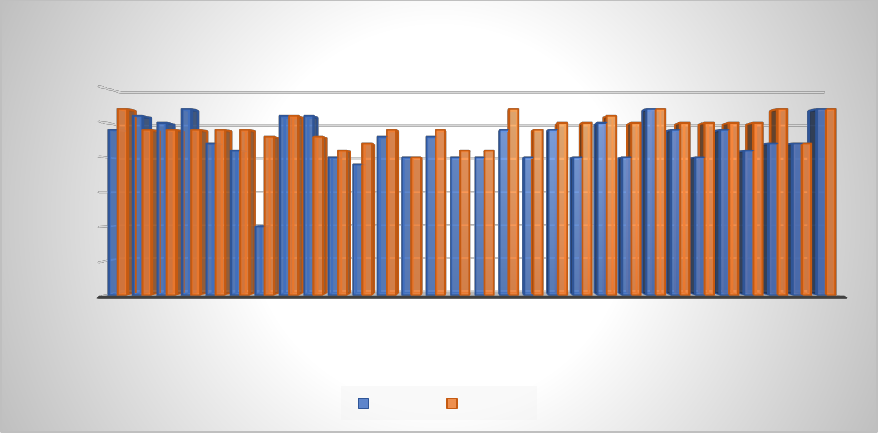
Table 7. Pre-test/Post-test Score Comparison
Note. This table displays pre-test (blue) and post-test (orange) scores per participant.
Higher post-test scores can be observed with this graphic.
Research question three, Does a higher educational level of licensed nurses and
CNAs have a positive correlation with increased knowledge of depression? sought to
determine if a higher level of education equated to a higher score on the pre-test. Within
the sample population there were two that indicated some high school education, 11 high
school graduates, 10 that had received some vocational training, four with an associate
degree, one with a bachelor’s degree, and two indicating other education. The highest
scoring participant and the lowest scoring participant identified as having an associate
degree.
To determine the relationship between participant pre-test scores and their
educational level, it is important to determine the type of data obtained. The pre-test
scores can be identified as ratio data as the difference between two values is meaningful
and there is a defined zero point. The participants level of education can be viewed as
ordinal data. The perceived order of education would be some high school, high school
0
5
10
15
20
25
30
P1 P3 P5 P7 P9 P11 P13 P15 P17 P19 P21 P23 P25 P27 P29
Correct Answers
Participant
Pre-test/Post-test Comparison
Pre-test Post-test

41
graduate, vocational training, associate degree, and bachelor’s degree. Participants that
identified their educational level as “other” were omitted due to the inability to determine
the order of educational level this category presents. A Spearman’s rank-order correlation
was chosen since the data was ordinal in nature.
A Spearman's rank-order correlation was performed to determine the relationship
between participants educational level and pre-test scores. The ratio data of the pre-test
scores was correlated with the ordinal data of the educational level of participants. A one
tailed test was utilized to due to the one directional effect of educational level on pre-test
scores. There was a weak, positive correlation between participants educational level and
pre-test scores, which was not statistically significant (rs(28) = .295, p = .064).
Correlations of pre-test scores and educational level are displayed in table 8. A scatter
plot of pre-test scores by educational level is displayed in table 9.
Table 8. Spearman’s rho correlations.
Correlations
PreTest
Education
Spearman's rho
PreTest
Correlation Coefficient
1.000
.295
Sig. (1-tailed)
.
.064
N
28
28
Education
Correlation Coefficient
.295
1.000
Sig. (1-tailed)
.064
.
N
28
28
Note. The table displays the correlation between pre-test scores and educational level of
participants.

42
Table 9. Scatterplot of Scores by Level of Education.
Note. This table displays pre-test scores separated by educational level with outlier
removed.
Sub research question, Can nursing home licensed nurses and CNAs identify risk
factors of depression? sought to look specifically at whether risk factors for depression
can be identified by correct responses for questions 2, 4, 5, 6, 8, and 9. Eighteen
participants answered each question correctly with all participants answering question 8
correctly on the pre-test. Twenty-two participants answered questions correctly for the
post-test with all participants answering questions 5 and 8 correctly. The combined
average for all six questions on the pre-test was 80.33%. The combined average for all
six questions on the post-test was 90.17%. Both pre-test and post-test participant
performance were greater than the established standard of 78.7% by Gabriel and Violato
(2009). Table 10 illustrates these results.

43
Table 10. Participant Ability to Identify Risk Factors of Depression.
Note. This table displays the number of participants that correctly answered questions 2,
4, 5, 6, 8, and 9 correctly.
Summary
Data for the study was collected using Google Forms. Thirty participants (N=30)
completed the study. Percentages were used to explain the participants demographic
information for age, gender, level of education, ethnicity, and employment. Descriptive
statistics was used to analyze the data along with a paired sample t-test. A paired samples
t-test was performed, excluding the identified outlier, comparing the pre-test scores to the
post-test scores with a finding of statistical significance. The findings indicated a
significant increase in knowledge of depression (p=.001) after an educational PowerPoint
presentation. A scatter plot was created to illustrate pre-test scores sorted by educational
level of the participant with a weak, positive correlation which was not statistically
significant (rs(28) = .295, p = .064). It was determined that participants in the sample
population were able to identify risk factors of depression with participants on the pre-
18
22
28
19
30
28
22
23
30
28
30
28
QUESTION 2 QUESTION 4 QUESTION 5 QUESTION 6 QUESTION 8 QUESTION 9
Correct Answers
Questions Specific for Risk Factors of Depression
Sub-Research Question 1
Pre-test Post-test
44
test and post-test scoring greater than the 78.7% established standard for the testing
instrument.
45
Chapter V
Discussion
Introduction
The literature review indicates a deficiency in the recognition and treatment of
depression among the nursing home population. A scholarly research project was
conducted to measure baseline knowledge of depression amongst licensed nursing and
CNA staff working in nursing homes and to determine if an educational PowerPoint
viewed by participants produced a measurable increase in their knowledge of depression.
The study focused on the following research questions:
1. What knowledge of depression do licensed nurses and CNAs working in
nursing homes possess prior to reviewing the educational PowerPoint?
2. Can an educational presentation over depression increase the recognition of
depressive symptoms in nursing home residents by nursing home licensed nurses
and CNA staff?
3. Does a higher educational level of licensed nurses and CNAs have a positive
correlation with increased knowledge of depression?
Sub-Research Question
1. Can nursing home licensed nurses and CNAs identify risk factors of
depression? (See Appendix B survey questions 2,4,5,6,8,9)
46
Data in relation to research question 1 was obtained through completion of the
pre-test by participants. The testing instrument had an established standard of 78.7% by
Gabriel and Violato (2009) with total of 16 of the 30 participants (53%) achieving a pre-
test score of 22 or greater representing satisfactory performance. The average score for
licensed staff and CNAs on the pre-test was 80% which suggests the nursing home staff,
in the facilities utilized for this study, are adequately educated on depression for long-
term care patients. Pre-test scores could also indicate that the pre-test instrument was not
specific enough to capture inadequacies of the staff. A larger sample from multiple states
would need to be studied to determine if results from this study are generalizable to other
states and facilities. In addition, an analysis of multiple state CNA education curriculum
would need to be conducted to determine if Kansas requirements are comparable to other
states. Education requirements and in-service education within different facilities may
also be a contributable factor.
Research question 2 relates to the comparison of the pre-test and post-test scores
of participants. A total of 26 of the 30 participants (86.6%) achieved a pre-test score of 22
or greater representing satisfactory performance. There were 10 more participants that
achieved satisfactory performance on the post-test when compared to the pre-test.
Following the educational PowerPoint, participants scored a combined average of 86.5%
for a measurable increase of 6.5%. The paired samples t-test indicates a p value of 0.001
which is statistically significant.
Another potential issue with participant results could be the way in which the pre-
test, educational PowerPoint, and post-test was administered. Participants received a link
that provided access to the testing sequence on Google Forms. Participants were not
47
monitored when completing the pre- and post-tests which could have impacted scores if
participants utilized outside materials while taking the tests. Participants could have also
taken the tests with a partner. Either of these occurrences could be confounding variables
effecting the outcomes of the study results (Tulchinsky & Varavikova, 2014).
The relation between participant educational level and their obtained scores was
interesting. Bing-Johnson et al. (2016) found a positive correlation between levels of
education and competence in nursing home care. The data from the study indicates there
is no statistical significance in educational level and the achieved scores of participants.
This discrepancy in the observed data and the literature may be due to the sample size of
the study. A sample size of thirty participants netted two with some high school
education, 11 high school graduates, 10 vocational graduates, four associates graduates,
one bachelor’s graduate, and two that identified as other schooling. In this instance, a
larger sample size is needed for generalizable results.
Data relating to sub-research question 1 indicates participants performed very
well answering questions targeting depression risk factors. A total of 22 of the 30
participants (73.3%) achieved a pre-test score of 22 or greater representing satisfactory
performance. A total of 18 of the 30 participants (60%) answered all the targeted
questions correctly on the pre-test with an increase in the number of participants with
correct answers on the post-test following an educational PowerPoint presentation.
Another consideration that has a potential impact on the data is the COVID-19
pandemic that was affecting the world at the time of the study. During the pandemic
nursing home residents were secluded from outside visitors to reduce transmission of the
virus causing the pandemic. The loss of socialization from friends and family members
48
resulted in an increase in mental health issues for nursing home residents. A result of
these events is an increased awareness of the nursing home resident’s mental health status
by licensed nursing and CNA staff. Participant’s performance in the study could be
directly related to the increased awareness brought about by the COVID-19 pandemic.
Evaluation of Theoretical Framework
Bennar’s Novice to Expert Theory is relevant to this study and served as a guiding
framework for the project. While there was no correlation in the data between educational
level and the attained scores of participants, although there remains a small improvement
from pre-test to post-test. The information provided to participants in the educational
PowerPoint was targeting individuals in the novice to beginner stages of the theory. A
guiding principle of Bennar’s theory is that learning and developing skills is done
through education, experience, and through developing skills of involvement with
patients and family (Petiprin, 2020). Data obtained on years of experience would have
been useful to add context to participant stage of professional development. Accounting
for years of experience along with educational level of participants would help more
accurately identify clinical stage of competence.
Recommendations for Future Research
The testing process and targeting a more diverse population are factors that need
addressed in future research. A testing process that ensures no outside information is
utilized will help measure individual participant baseline knowledge with more accuracy.
A more condensed testing instrument might have been beneficial in two ways. A smaller
instrument could produce more results as participants might not quit before completion of
the PowerPoint and testing. Targeting a more diverse population to draw a sample from,
49
preferably from multiple states, could be beneficial in identifying if there is a measurable
difference between state certification requirements have an influence depression
knowledge.
Limitations of Study
One limitation is that the pre-test and post-test were only available for two weeks.
Three facilities gave consent to allow the testing sequence to be presented to their staff.
There were 212 eligible staff among the three facilities with 30 participants in the study
for a sample size of 14.15%. A larger sample size would be more representative of the
population. With more time, more facilities and more participants could be recruited.
Another potential limiting factor was the willingness of participants to sit through a long
testing sequence. A shorter testing sequence would help ensure participants finished all
parts before opting to remove themselves from the study.
Implications for Practice/Health Policy/Education
Future studies of a similar nature would be needed to verify the findings of this
study. However, if the findings of this study are accurate, other avenues of addressing the
deficiency of depression recognition and treatment in the nursing home population need
to be explored. An evaluation of depression assessment tools would be a logical next step
followed by an evaluation of primary care providers assessment and prescribing
practices.
Conclusion
Untreated and undiagnosed depression in the nursing home elderly is an issue
affecting nursing homes today and will become more prominent as the baby boomer
generation reaches that age group. Depression can decrease quality of life and complicate
50
other chronic diseases. Identifying the disorder is imperative to treating it. The staff
working within nursing homes have the most contact with this population and should
have knowledge of the disorder. The study was conducted to determine the current
depression knowledge of licensed nursing staff and CNA’s while also measuring if there
was an increase in depression knowledge following an educational PowerPoint.
Participants of the study displayed a reasonable knowledge of depression through test
scores with a measurable increase gain following an educational PowerPoint.
51
References
Abrams, R. C., Nathanson, M., Silver, S., Ramirez, M., Toner, J. A., & Teresi, J. A.
(2016). A training program to enhance recognition of depression in nursing
homes, assisted living, and other long-term care settings: Description and
evaluation. Gerontology & Geriatrics Education, 38(3), 325-345.
Alpert, F., & Hodkinson, C. S. (2019). Video use in lecture classes: Current practices,
student perceptions and preferences. Education + Training, 61(1), 31-45.
doi:10.1108/ET-12-2017-0185
Aggarwal, R., & Ranganathan, P. (2019). Study designs: Part 2 - Descriptive studies.
Perspectives in Clinical Research, 10(1), 34–36.
https://doi.org/10.4103/picr.PICR_154_18
Ashcroft, R., Silveira, J., Rush, B., & Mckenzie, K. (2014). Incentives and disincentives
for the treatment of depression and anxiety: A scoping review. Canadian Journal
of Psychiatry, 59(7), 385-392.
Bell, K. (n.d.). activity theory definition | Open Education Sociology Dictionary.
Retrieved 5 April 2021, from https://sociologydictionary.org/activity-theory/
Beuscher, L., & Dietrich, M. (2016). Depression training in an assisted living facility: A
pilot study. Journal of Psychosocial Nursing and Mental Health Services, 54(5),
25-31. doi:10.3928/02793695-20160201-01
Birkett, A. (2020). One-Tailed vs. Two-Tailed Tests (Does It Matter?). Retrieved from
https://cxl.com/blog/one-tailed-vs-two-tailed-tests/
Centers for Disease Control and Prevention. (2014, January 31). QuickStats: Percentage
of users* of long-term care services with a diagnosis of depression,† by provider

52
type - national study of long-term care providers, United States, 2011 and 2012.
Morbidity and Mortality Weekly Report.
https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6304a7.htm?s_cid=mm6304
a7_w
Chauhan, P., Kokiwar, P. R., Shridevi, K., & Katkuri, S. (2016). A study on prevalence
and correlates of depression among elderly population of rural South
India. International Journal Of Community Medicine and Public Health 3, 236-
239.
Chatterjee, S., Bali, V., Carnahan, R. M., Chen, H., Johnson, M. L., & Aparasu, R. R.
(2017). Risk of mortality associated with anticholinergic use in elderly nursing
home residents with depression. Drugs & aging, 34(9), 691-700. 10.1007/s40266-
017-0475-5
Chauvet-Gelinier, J. C., & Bonin, B. (2017). Stress, anxiety and depression in heart
disease patients: A major challenge for cardiac rehabilitation. Annals of Physical
and Rehabilitation Medicine, 60(1), 6-12.
Cornish, E. K., Bergner, E. M., & Griffith, D. M. (2017). “They have said that I was
slightly depressed but there are circumstances that bring that on”: How middle-
aged and older African American men describe perceived stress and
depression. Ethnicity & disease, 27(4), 437.
Damian, J., Pastor-Barriuso, R., Valderrama-Gama, E., & de Pedro-Cuesta, J. (2017).
Association of detected depression and undetected depressive symptoms with
long-term mortality in a cohort of institutionalised older people. Epidemiology
and psychiatric sciences, 26(2), 189-198.

53
Depression. (n.d.). In Merriam-Webster.com. Retrieved March 8, 2021, from
https://www.merriam-webster.com/dictionary/depression.
Discussion on Benner’s Theory of Novice to Expert. (2019).
https://www.needassignmenthelp.com/blog/discussion-benners-theory-novice-
expert/
Elderly. (n.d.). In Merriam-Webster.com. Retrieved March 8, 2021, from
https://www.merriam-webster.com/dictionary/elderly
Erdal, A., Flo, E., Selbaek, G., Aarsland, D., Bergh, S., Slettebo, D. D., & Husebo, B. S.
(2017). Associations between pain and depression in nursing home patients at
different stages of dementia. Journal of Affective Disorders, 218, 8-14.
Gabriel, A., & Violato, C. (2009). The development of a knowledge test of depression
and its treatment for patients suffering from non-psychotic depression: A
psychometric assessment. BMC Psychiatry, 9(1), 56-56.
https://doi.org/10.1186/1471-244X-9-56
Garay, R. P., Zarate Jr, C. A., Charpeaud, T., Citrome, L., Correll, C. U., Hameg, A., &
Llorca, P. M. (2017). Investigational drugs in recent clinical trials for treatment-
resistant depression. Expert review of Neurotherapeutics, 17(6), 593-609.
Giri, M., Chen, T., Yu, W., & Lü, Y. (2016). Prevalence and correlates of cognitive
impairment and depression among elderly people in the world's fastest growing
city, chongqing, people's republic of china. Clinical Interventions in Aging, 11,
1091-1098. https://doi.org/10.2147/CIA.S113668
54
Goforth, C. (2015). Using and interpreting Cronbach’s Alpha | University of Virginia
Library Research Data Services and Sciences.
https://data.library.virginia.edu/using-and-interpreting-cronbachs-alpha/.
Gonyea, J. G., Curley, A., Melekis, K., Levine, N., & Lee, Y. (2018). Loneliness and
depression among older adults in urban subsidized housing. Journal of Aging and
Health, 30(3), 458-474. https://doi.org/10.1177/0898264316682908
Guimarães, L. d. A., Brito, T. A., Pithon, K. R., Jesus, C. S. d., Souto, C. S., Souza, S. J.
N., & Santos, T. S. D. (2019). Depressive symptoms and associated factors in
elderly long-term care residents. Ciência & Saude Coletiva, 24(9), 3275-3282.
https://doi.org/10.1590/1413-81232018249.30942017
Hollis-Sawyer, L., & Dykema-Engblade, A. (2016). Disengagement Theory.
https://www.sciencedirect.com/topics/psychology/disengagement-theory
Institute of Medicine (US) Committee on the Future Health Care Workforce for Older
Americans. Retooling for an Aging America: Building the Health Care
Workforce. Washington (DC): National Academies Press (US); 2008. 4, The
Professional Health Care Workforce. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK215402/
Juman, R., & Figlerski, R. (2017). Vintage Voices: Depression in nursing homes.
https://www.todaysgeriatricmedicine.com/archive/SO17p34.shtml#:~:text=Untrea
ted%20depression%20may%20be%20the,when%20they%20otherwise%20could
%20thrive.
KANSAS 90-HOUR CERTIFIED NURSE AIDE PROGRAM INSTRUCTION
MANUAL. The Kansas Department for Aging and Disability Services. (2021).

55
Retrieved from https://www.kdads.ks.gov/docs/default-source/survey-
certification-and-credentialing-commission/health-occupations-
credentialing/traning-provider-information/nurse-aide/cna-instructor-
manual.pdf?sfvrsn=dd9d07ee_2.
Kaushal, N., Kaur, S., Kaur, N., & Singh, D. (2019). Prevalence of depression among
elderly people in old age homes, Chandigarh. religion, 31, 62. 142-146
Kent State University Libraries, 2021. LibGuides: SPSS Tutorials: Paired Samples t Test.
[online] Libguides.library.kent.edu. Available at:
<https://libguides.library.kent.edu/SPSS/PairedSamplestTest> [Accessed 3
August 2021].
Kuehner, C. (2017). Why is depression more common among women than among
men? The Lancet Psychiatry, 4(2), 146.
Kvæl, L. A., Bergland, A., & Telenius, E. W. (2017). Associations between physical
function and depression in nursing home residents with mild and moderate
dementia: a cross-sectional study. BMJ Open, 7(7), e016875. 10.1136/bmjopen-
2017-016875
Lantz, M. (2019). Recognizing and treating depression in dementia in a nursing home
population. Retrieved from https://www.medscape.org/viewarticle/430711
Levin, C. A., Wei, W., Akincigil, A., Lucas, J. A., Bilder, S., & Crystal, S. (2007,
November). Prevalence and treatment of diagnosed depression among elderly
nursing home residents in Ohio. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2887720/

56
Levis, B., Benedetti, A., & Thombs, B. (2019). Accuracy of patient health questionnaire-
9 (PHQ-9) for screening to detect major depression: Individual participant data
meta-analysis. BMJ, l1781. 10.1136/bmj.l1781
McCarthy-Zelaya, I. (2016). Depression in older adults in nursing homes: a review of
the literature. doi:10.15760/honors.259
Mitchell, A. J., Sheth, B., Gill, J., Yadegarfar, M., Stubbs, B., Yadegarfar, M., &
Meader, N. (2017). Prevalence and predictors of post-stroke mood disorders: a
meta-analysis and meta-regression of depression, anxiety and adjustment
disorder. General Hospital Psychiatry, 47, 48-60.
Moulton, S. T., Türkay, S., & Kosslyn, S. M. (2017). Does a presentation's medium affect
its message? PowerPoint, prezi, and oral presentations. PloS One, 12(7),
e0178774-e0178774. https://doi.org/10.1371/journal.pone.0178774
National Institute on Aging. (n.d). Depression and older adults. U.S. Department of
Health and Human Services. Retrieved March 31, 2021, from
https://www.nia.nih.gov/health/depression-and-older-adults.
Nelson, J. C., & Spyker, D. A. (2017). Morbidity and mortality associated with
medications used in the treatment of depression: an analysis of cases reported to
US poison control centers, 2000–2014. American Journal of Psychiatry, 174(5),
438-450.
Nursing home. (n.d.). In Merriam-Webster.com. Retrieved March 8, 2021, from
https://www.merriam-webster.com/dictionary/nursing home.
Perkkiö, Y., Jokelainen, J., Auvinen, J., Eskola, P., Saltevo, J., Keinänen-Kiukaanniemi,
S., & Timonen, M. (2019). Glucose status and depressive symptoms: a cohort
57
study of elderly people in northwest Finland. Scandinavian Journal of Primary
Health Care, 37(2), 242-248.
Petiprin, A. (2020). Dr. Patricia Benner - Nursing Theory. Retrieved from
https://nursing-theory.org/nursing-theorists/Patricia-Benner.php.
Pramesona, B. A., & Taneepanichskul, S. (2018). The effect of religious intervention on
depressive symptoms and quality of life among indonesian elderly in nursing
homes: A quasi-experimental study. Clinical Interventions in Aging, 13, 473-
483. https://doi.org/10.2147/CIA.S162946
Resident. (n.d.). In Merriam-Webster.com. Retrieved March 8, 2021, from
https://www.merriam-webster.com/dictionary/resident.
Safar, A.H. (2015). Educating with prezi: A new presentation paradigm for teaching,
learning, and leading in the digital age. College Student Journal, 49(4), 491.
Simning, A., & Simons, K. (2017). Treatment of depression in nursing home residents
without significant cognitive impairment: a systematic review. Int
Psychogeriatric, 29(2), 209–226. doi:10.1017/S1041610216001733
State Nurse Aide Training: Program Information and Data. (2002).
https://oig.hhs.gov/oei/reports/oei-05-01-00031.pdf.
Trinkoff, A. M., Storr, C. L., Lerner, N. B., Yang, B. K., & Han, K. (2017;2016;). CNA
training requirements and resident care outcomes in nursing homes. The
Gerontologist, 57(3), 501-508. https://doi.org/10.1093/geront/gnw049.
Trueland, J. (2017). Outdoor spaces improve dementia care: Spending time outdoors can
reduce symptoms of depression in care home residents. but easy access and
58
careful design are a must if residents are to get the most out of their gardens.
Nursing Standard, 32(2), 24-26. https://doi.org/10.7748/ns.32.2.24.s24
Tulchinsky, T. H., & Varavikova, E. A. (2014). Chapter 3 - measuring, monitoring, and
evaluating the health of a population. In T. H. Tulchinsky, & E. A. Varavikova
(Eds.), The new public health (third edition) (pp. 91-147). San Diego: Academic
Press. doi:https://doi.org/10.1016/B978-0-12-415766-8.00003-3 Retrieved
from https://www.sciencedirect.com/science/article/pii/B9780124157668000033
Weinberger, A. H., Gbedemah, M., Martinez, A. M., Nash, D., Galea, S., & Goodwin,
R. D. (2018). Trends in depression prevalence in the USA from 2005 to 2015:
Widening disparities in vulnerable groups. Psychological Medicine, 48(8), 1308-
1315. https://doi.org/10.1017/S0033291717002781
World Health Organization. (2018, 22 March.) Depression. (2018, March 22). Retrieved
from https://www.who.int/news-room/fact-sheets/detail/depression.
Zalavadiya, D. D., Banerjee, A., Sheth, A. M., Rangoonwala, M., Mitra, A., & Kadri, A.
M. (2017). A comparative study of depression and associated risk factors among
elderly inmates of old age homes and community of rajkot: A gujarati version of
the geriatric depression scale-short form (GDS-G). Indian Journal of Community
Medicine, 42(4), 204-208. https://doi.org/10.4103/ijcm.IJCM_181_16
APPENDIX
60
Appendix A
Pre-test and Posttest Instruments
Depression Knowledge Test
1. What is your gender?
Female
Male
2. Which race/ethnicity best describes you? (Please choose only one.)
American Indian or Alaskan Native
Asian / Pacific Islander
Black or African American
Hispanic
White / Caucasian
Multiple ethnicity / Other (please specify)
3. What is your age?
Under 18
18-24
25-34
35-44
45-54
55-64
65+
4. What is the highest level of education you have completed?
Have not completed High School
61
High School Graduate
LPN
Associates Degree in Nursing
Bachelor’s Degree in nursing
5. Which of the following categories best describes your employment status?
Employed, working full-time
Employed, working part-time
Employed, working PRN
62
Appendix B
Pre-test and Post-test Survey
1. Which of the following statements about clinical depression is FALSE?
It is a medical disorder.
It is a weakness of character.
It is a common psychiatric disorder.
It affects both males and females.
2. What is the risk of death by suicide among depressed patients?
The risk is very minimal.
The risk is between 15% and 50%.
The risk is below 15%.
The risk is above 50%.
3. What are the lifetime chances of becoming clinically depressed?
One in 1000
One in 50
One in 3
One in 1
4. Which of the following is TRUE about the age of onset of depression?
Depression does not always begin in adolescence.
Depression can start in childhood or adolescence.
Depression can appear for the first time in middle-aged people.
Depression does not usually affect young children.
63
5. Which of the following, about sex differences in depression is TRUE?
Clinical depression only occurs in women.
Clinical depression is more common in women than men.
Clinical depression is more common in men than women.
Only men get depressed.
6. Which of the following is FALSE about the relapse of clinical depression?
The number of previous episodes of clinical depression increases the chances of
subsequent episodes.
After the first episode of clinical depression, there is an increased risk of a second
episode.
Maintenance treatment can reduce the chances of relapse.
After recovery, there is zero risk for recurrence.
7. Which of the following behavior is associated with poor outcome?
Taking antidepressant treatments regularly
Being involved in talk therapy (psychotherapy)
Staying sober
Stopping antidepressant medications if feeling well
8. What factors may trigger the onset of clinical depression?
Biological factors, such as genetics
Psychological factors such as having marital problems
Social factors such as losing a job
All of the above
64
9. Depression may be triggered by all the following EXCEPT:
Prolonged severe grief
Taking antidepressants
Certain medical conditions
The birth of a new baby
10. The following are indications of clinical depression EXCEPT:
Changes in sleep patterns
Poor concentration
Frequent crying for no obvious reasons
Occasional sadness
11. Which is NOT true about the differences between depression and a passing blue
mood?
People with depression can "pull themselves together."
Depression can be disabling in day-to-day functioning.
Patients who are clinically depressed look sad.
Without treatment, symptoms of clinical depression can last for weeks, months, or years.
12. All the following are recognized symptoms of clinical depression EXCEPT:
Marked loss of interests.
Excessive sleep
Loss of energy
Good concentration
65
13. Which of the following is NOT a symptom of clinical depression?
Restlessness
Changes in appetite
Good decision making
Lack of energy
14. All the following are typical of patients suffering from clinical depression EXCEPT:
Negative thinking that can lead to self-defeating or suicidal behavior.
Mental fatigue and the inability to solve complicated problems.
Marked forgetfulness.
Normal memory.
15. Which is NOT a common symptom of clinical depression?
Poor motivation
Normal energy
Feelings of guilt or self-blame
Fatigue
16. Which of the following statements about the speed of response to the treatment with
antidepressants is FALSE?
Symptoms improve immediately after treatment is begun.
Many antidepressants may take several weeks to start to work.
It is important to continue taking medication even if symptoms improve.
Not all symptoms respond to antidepressants at the same rate.
66
17. If medication does not improve depressive symptoms, one should:
Stop taking all medication.
Talk to a health care professional.
Double the pill dosage.
Ask friends about what to do.
18. Which is NOT a recognized treatment for clinical depression?
Medication
Talk therapy
Light therapy (photo-therapy)
Kiekie therapy
19. Which is NOT a common side effect antidepressant drugs?
Upset stomach
Sleep disturbances
Sexual side-effects (e.g. problems with sexual desire or orgasm)
Feelings of depression
20. Which is FALSE about the effectiveness of antidepressant medications?
About 30-40% of patients do not respond to the initial treatment.
Moderate symptom improvement may take few weeks to be achieved in those who will
respond.
Using more than one antidepressant may be necessary for some patients.
Recovery of symptom can be achieved in all depressed patients
67
21. Which is NOT a common occurrence during treatment with antidepressants?
Gaining weight
Severe continuous headaches
Feeling sleepy
Sweating
22. Which is FALSE about the response to treatment with antidepressants?
Up to 80% of people with depression do get better with the right medication.
Most people with depression need to be treated for at least six to nine months to prevent
relapse.
For some people, it is necessary to stay on medication for long-term maintenance
therapy.
If the acute depressive symptoms are relieved, the patient should stop antidepressants.
23. Psychotherapy can help many people with depression. Which of the following
statements about psychotherapy is FALSE?
Both individual and group talk therapy provides an opportunity to express and discuss
thoughts and feelings with the therapist.
Therapy may help to resolve life issues that may contribute to depression.
All depressed individuals benefit from psychotherapy.
In psychotherapy, negative, and self-defeating thoughts can be replaced by more
positive, realistic thoughts.
24. If one feels better during the course of treatment, one should
Stop taking antidepressant medication.
Discuss the course of antidepressants treatment with doctor.
Reduce the antidepressant dose by half.
Start a course of herbal treatment.
68
25. What should one do if one's first antidepressant medication fails?
Consult one's doctors.
Take sleeping pills.
Drink more alcohol.
Use magnetic therapy.
26. Which is FALSE about Electric Convulsive Therapy (ECT) for treating clinical
depression?
It is proved to be effective.
It is a safe method.
It is no longer used for treating depression.
It is given under general anesthesia.
27. Which is FALSE about selecting the right antidepressant for someone with
depression?
There are no available laboratory tests to guide doctors' choices for treating clinical
depression.
Different people have different responses to antidepressants.
Doctors can tailor antidepressants to suit the symptoms of individual patients.
Doctors can always tell beforehand how a person is going to respond to the medication
they prescribe.

69
Appendix C
Depression Presentation
Depression in the Elderly
(National Institute on Aging, n.d.)
Jason Heflin
Pittsburg State University

70
Slide 2
Mental Illnesses in the Elderly
• Older population is increasing rapidly, intensifying the likelihood of
old age challenges.
• Older people are more exposed to mental illnesses.
• At least 15% of the elderly (60 and above) have a mental disorder
(World Health Organization, 2017).
• Mental and neurological maladies account for 6.6% of the elderly’s
disabilities.
• Affecting at least 5% and 7% of the elderly, dementia and
depression are the most prevalent mental disorders in the age group.
The older population is increasing rapidly, intensifying the likelihood of old age
challenges for many. The World Health Organization (WHO) provides worrying statistics
about the nature of mental health in the elderly population. Older people are more
exposed to mental illnesses. WHO (2017) reports that at least 15% of the older people
(60 and above) have a mental disorder. With disabilities being common among this
elderly population, 6.6% of total disability results from mental and neurological
ailments. Of these cognitive and neurological disorders, dementia and depression affect
the most older adults, with 5% and 7%, respectively, suffering from the two conditions.

71
Slide 3
Common Misconceptions for
Depression in the Elderly
• Late life and young age depression have different symptoms.
• Depression is more common in old than young age.
• Depression is more chronic in late than young age.
• It is more difficult to treat old age depression than young age
depression.
• Old-age depression is often a result of psychological issues.
Haigh et al. (2018) provide five common myths and misconceptions about depression in
the elderly and uses evidence to counter and provide factual truths. The first myth and
misconception relate to symptoms of depression in old and young ages. While people
think that the two are symptomatically different, Haigh et al. (2018) explain that
depression symptoms are the same across adulthood and that observed symptomatic
differences could be due to unaccounted for methodological issues such as onset age
and the chronic nature of depression. Other myths that the study discredits are
depression is more common, chronic, and difficult to treat in old than young age, and
old-age depression is often a result of psychological issues.

72
Slide 4
Depression among the Elderly Nursing
Home Population
• Studies have not focused on depression among the elderly in
nursing homes.
• Depression rate in the nursing home population has not been
comprehensively considered.
• Older adults living in assisted living are more prone to
depression (Almonani & Bani-Issa, 2017).
• At 42.5% depression is more prevalent in nursing homes than
other settings (Pramesona & Taneepanichskul, 2018).
• Though depression is high in nursing homes, “it is
underdiagnosed” (Rasmieh et al., 2019, p.1).
Most studies conducted have focused on other settings ignoring the elderly in the nursing
homes. As a result, the depressed adults in nursing homes and the depression rate among
the population are unconsidered. According to Almomani and Bani-Issa (2017), older
adults living in assisted living are more prone to depression. Focusing on studying the
prevalence and risk factors of depression in nursing homes, Pramesona and
Taneepanichskul (2018 ) found that 42.5% of the older adults in nursing homes are
depressed. At that rate, they explain that depression is more prevalent among the elderly
in nursing homes than in other settings, as previous research has shown a significantly
lower percentage. Therefore, though depression is high in nursing homes, “it is
underdiagnosed” (Rasmieh et al., 2019, p.1).

73
Slide 5
Reasons Why Depression is Overlooked
among the Elderly in Nursing Homes
• There are differences in the occurrence of signs and symptoms of
depression in the elderly.
• Depression is confused with the effects of the elderly’s illnesses.
• Depression is confused with the side effects of medication.
• People assume that depression is a normal occurrence as one ages.
Depression is highly underdiagnosed among older adults in nursing homes mainly
because its symptoms are ignored or overlooked. Several factors contribute to
depressive symptoms being overlooked in this population. One major reason is the
differences in the signs and symptoms of depression across different older people. In
essence, there are various causes and risk factors of depression in the elderly, resulting
in symptoms being displayed differently. Another reason is the confusion of the
depressive symptoms with the effects of the elderly’s illnesses and their medication.
Also, the assumption that depression is normal as one ages leads to the under-diagnosis
and under-treatment of depression in assisted living facilities.
74
Slide 6
Signs and Symptoms of Depression in the
Elderly Nursing Home Population
• Functional impairments.
• High suicide levels.
• Decline in health before death (Zhao, et al., 2018).
• Loss of interest.
• Depressed mood.
• Fatigue.
• Weight loss.
• Poor self-care.
• Social isolation (Rasmieh, 2019).
According to Zhao et al. (2018), the common depressive symptoms among older people
in nursing homes are functional impairments, high suicide levels, and health decline
before their death. Depressive disorders in the more senior nursing home population
affect their willingness to live. Therefore, other symptoms observed include loss of
interest or dejected mood, fatigue, weight loss due to reduced appetite, poor-self
hygiene to inadequate self-care, and social isolation (Rasmieh, 2019). These symptoms
may be characteristic of one or several depressive disorders common in the elderly. For
instance, dementia and depression have been said to occur concurrently.

75
Slide 7
Differences between Depression in the
Elderly and Young People
• Depression occurs alongside other illnesses and disabilities in the
elderly.
• Depression lasts longer among the elderly.
• Depression increases the risks of cardiovascular illnesses and death
among the elderly.
• Depression reduces rehabilitation abilities among the elderly.
There are significant differences between depression in the elderly and young people.
One of the leading dissimilarities is the occurrence of depression alongside other
illnesses and disabilities in the elderly population, making it easy to miss the signs and
symptoms of geriatric depression. Also, while depression in young people can last for a
short time, mainly if appropriate treatment is provided, it tends to last longer among the
elderly. Moreover, depression in the elderly increases the risks of chronic and
cardiovascular illnesses and death. Liguori et al. (2018) found a striking relationship
between heart attack and depression in the elderly population. Another difference
between depression in the elderly and young people is that it decreases rehabilitation
abilities for the elderly.

76
Slide 8
Causes of Depression in the Elderly
Nursing Home Population
• Intense pain.
• Poor physical health.
• Prior institutionalization (Almomani & Bani-Issa, 2017).
• Increased anxiety.
• Mobility problems.
• Self-care issues (Rasmieh et al. 2019).
(Kumar, 2017)
The elderly population in nursing homes are exposed to significant challenges than their
counterparts at home, especially immediately following their placement. Therefore,
Almomani and Bani-Issa (2017) found that many older adults in nursing homes suffered
depression in the first year following their settlement. The common causes of
depression in this elderly nursing home population they list are: “pain, poor physical
health, and prior institutionalization” before placement (p.1646). Besides, Rasmieh et al.
(2019) found that anxiety, mobility problems, and self-care issues were also a common
complaint and cause of depression for those in nursing homes. All these issues increase
the stress level for older people in nursing homes, ultimately leading to depression.

77
Slide 9
Risk Factors for Depression in the Elderly
Nursing Home Population
• Gender. Being female increase the likelihood of depression among
the elderly.
• Loneliness or absence of social support from family members and
the nursing home.
• Chronic illnesses heighten the risk of being depressed for an old
person in a nursing homes.
• Perceived inadequate care in the nursing home also contributes to
depression among the elderly.
Pramesona & Taneepanichskul (2018) found the risk factors for depression among the
elderly in nursing homes are: gender, loneliness, chronic illnesses, and perceived lack of
care. While depression occurs across both genders, the study found that females were
more prone to depressive tendencies. Loneliness resulting from social isolation is also a
significant cause of depression in the elderly at nursing homes. Loneliness was
associated with the length of stay in the nursing home and the psychological support
from family members. Having three or more chronic illnesses is also a significant risk
factor for depression in the nursing home population, as is apparent care inadequacy.
Care inadequacy occurred in the univariate and multivariate analysis of the depression
risk factors.

78
Slide 10
Consequences of Depression in Older
Adults in Nursing Homes
• High mortality.
• Increased medical problems.
• Sleep disruptions.
• Physical pain.
• Diminished physical exercise.
• Poor eating which may result in
malnutrition or obesity.
• Self neglect.
(Human Rights Watch, 2018)
When left untreated, depression can have severe consequences for the elderly nursing
home populations. Almomani and Bani-Issa (2017) explain that untreated depression
can cause sleep disruptions, reduce physical activities, encourage poor eating habits and
self-neglect. These factors have short-term and long-term consequences, such as
malnutrition or obesity. The depressed older person may also suffer from increased
medical problems, especially chronic illnesses. Overall, untreated depression increases
the chance of death for older people.

79
Slide 11
Health Promotion to Improve Depression
among Older People in Nursing Homes
▪ Improving depression among the elderly revolves around health
promotion strategies that meet
their needs (WHO, 2017).
• To improve depression, nursing homes should care for the needs of the
aging by:
✓ Giving them freedom to explore their interests to live fulfilling life.
✓ Assuring security so that they do not worry about their survival.
✓ Availing social support to avoid loneliness.
WHO (2017) notes that improving depression among older people revolves around
health promotion strategies that meet their needs. As a result, nursing homes can
promote health among older people by reducing depression causes and risk factors.
Doing so necessitates giving the more senior person autonomy over their lives. Nursing
homes have to allow older people to do things that they make them appreciate their
lives. Also, nursing homes should provide and assure security. Security revolves around
many things, including shelter and food. Besides, social support is critical in the mental
health of not just the elderly but everyone. Providing avenues that prevent isolation can
help reduce depressive disorders among this population.

80
Slide 12
Depression Interventions among the
Elderly Population
• Constant screening for mental illnesses.
• Early diagnosis of depressive disorders.
• Enhancing mental, physical, and functional health.
• Recognizing and treating illnesses associated with depressive
disorders.
• Distinguishing and handling difficult behavior.
Nursing homes can accomplish different goals to provide interventions for depression in
their aging populations. Since depression often occurs without being detected, nursing
homes should continuously screen their residents for mental illnesses, diagnose
depression early and begin treatment. They can also enhance mental, physical, and
functional health, recognize and treat illnesses associated with depressive disorders, and
distinguish and manage problematic behavior.

81
Slide 13
Treatment Modalities for Depression in
Older People in Nursing Homes
• The following are some of the treatment modalities that can be used
instead of or alongside medication:
✓ Cognitive-behavioral therapy.
✓ Problem-solving therapy.
✓ Physical exercise.
✓ Behavioral activation.
(National Institute on Aging, n.d.)
Holvast et al. (2017) “non-pharmacological treatments” are better and more useful among
older people as antidepressants add to polypharmacy and potential drug interactions.
They found that cognitive behavioral therapy and problem-solving therapy helped in
short-term follow-up of depressive disorders. Psychotherapy treatments help patients in
identifying, avoiding, and overcoming destructive behaviors. When used in treatment of
depression, psychotherapy helps in countering symptoms of depressive disorders, with
the overall possibility of increasing the wellbeing of the patient and resulting in a much
more fulfilling life. Behavioral activation and physical exercise allows the patient to take
active role in treating and preventing reoccurrence of depressive symptoms by managing
the causes and risk factors.
82
Slide 14
References
• Almomani, F. M., & Bani-Issa, W. (2017). The incidence of
depression among residents of assisted living: Prevalence and
related risk factors. Clinical Interventions in Aging, 12, 1645.
• Haigh, E. A., Bogucki, O. E., Sigmon, S. T., & Blazer, D. G. (2018).
Depression among older adults: A 20-year update on five common
myths and misconceptions. The American Journal of Geriatric
Psychiatry, 26(1), 107-122.
• Holvast, F., Massoudi, B., Oude Voshaar, R. C., & Verhaak, P. F.
(2017). Non-pharmacological treatment for depressed older patients
in primary care: A systematic review and meta-analysis. PloS
One, 12(9), e0184666.
83
Slide 15
References
• Human Rights Watch. (2018, February 5). “They Want Docile.”
How Nursing Homes in the United States Overmedicate People with
Dementia. https://www.hrw.org/report/2018/02/05/they-want-
docile/how-nursing-homes-united-states-overmedicate-people-
dementia.
• Kumar, P. (2017). Facts About Depression In Elderly. boldsky.
https://www.boldsky.com/health/wellness/2017/depression-in-
elderly-people/articlecontent-pf144970-110360.html.
• Liguori, I., Russo, G., Curcio, F., Sasso, G., Della-Morte, D.,
Gargiulo, G., ... & Testa, G. (2018). Depression and chronic heart
failure in the elderly: An intriguing relationship. Journal of
Geriatric Cardiology: JGC, 15(6), 451.
84
Slide 16
References
• National Institute on Aging. (n.d.). Depression and Older Adults.
https://www.nia.nih.gov/health/depression-and-older-adults.
• Pramesona, B. A., & Taneepanichskul, S. (2018). Prevalence and
risk factors of depression among Indonesian elderly: a nursing
home-based cross-sectional study. Neurology, Psychiatry and Brain
Research, 30, 22-27.
• Rasmieh, A. A., Subih, M., Aldaraawi, H., Randall, S., Othman, W.
M. M., & Salamonson, Y. (2019). Prevalence of depression and its
influence on the quality of life of Jordanians living in residential
care facilities. Journal of Nursing Research, 27(6), e54.

85
Slide 17
References
• World Health Organization (WHO). (2017). Mental health of older
adults. https://www.who.int/news-room/fact-sheets/detail/mental-
health-of-older-adults.
• Zhao, X., Zhang, D., Wu, M., Yang, Y., Xie, H., Li, Y., ... & Su, Y.
(2018). Loneliness and depression symptoms among the elderly in
nursing homes: A moderated mediation model of resilience and
social support. Psychiatry research, 268, 143-151.
