
1
April 4, 2016
NOTE TO: Medicare Advantage Organizations, Prescription Drug Plan Sponsors, and
Other Interested Parties
Subject: Announcement of Calendar Year (CY) 2017 Medicare Advantage Capitation
Rates and Medicare Advantage and Part D Payment Policies and Final Call Letter
In accordance with section 1853(b)(1) of the Social Security Act, we are notifying you of the
annual Medicare Advantage (MA) capitation rate for each MA payment area for CY 2017 and
the risk and other factors to be used in adjusting such rates. The capitation rate tables for 2017
are posted on the Centers for Medicare & Medicaid Services (CMS) web site at
http://www.cms.gov/Medicare/Health-Plans/MedicareAdvtgSpecRateStats/index.html under
Ratebooks and Supporting Data. The statutory component of the regional benchmarks,
transitional phase-in periods for the Affordable Care Act rates, qualifying counties, and each
county’s applicable percentage are also posted at this website.
Attachment I shows the final estimates of the National Per Capita MA Growth Percentage for
2017 and the National Medicare Fee-for-Service (FFS) Growth Percentage for 2017. These
growth rates will be used to calculate the 2017 capitation rates. As discussed in Attachment I,
the final estimate of the National Per Capita MA Growth Percentage for combined aged and
disabled beneficiaries is 3.08 percent, and the final estimate of the FFS Growth Percentage is
3.12 percent. Attachment II provides a set of tables that summarizes many of the key Medicare
assumptions used in the calculation of the National Per Capita MA Growth Percentage.
Section 1853(b)(4) of the Act requires CMS to release county-specific per capita FFS
expenditure information on an annual basis, beginning with March 1, 2001. In accordance with
this requirement, FFS data for CY 2014 are being posted on the above website.
Attachment II details the key assumptions and financial information behind the growth
percentages presented in Attachment I.
Attachment III presents responses to Part C payment related comments on the Advance Notice of
Methodological Changes for CY 2017 MA Capitation Rates and Part C and Part D Payment
Policies (Advance Notice).
Attachment IV presents responses to Part D payment related comments on the Advance Notice.
Attachment V shows the final Part D benefit parameters and contains details on how they are
updated.
Attachment VI shows the CMS-HCC and RxHCC Risk Adjustment Factors
2
Attachment VII presents the final Call Letter.
We received many submissions in response to CMS’ request for comments on the Advance
Notice/Call Letter, published on February 19, 2016. Comments were received from professional
organizations, MA and Part D sponsors, advocacy groups, the pharmaceutical industry, members
of congress, pharmacy benefit managers, pharmacies, and concerned citizens.

3
Key Changes from the Advance Notice:
Growth Percentages: Attachment I provides the final estimates of the National MA Growth
Percentage and the FFS Growth Percentage and information on deductibles for MSAs.
Calculation of FFS Rates: We are finalizing the methodology that we proposed for calculating
FFS rates with two modifications. First, the rebasing of DME claims in non-competitively bid
areas (non-CBAs) are based on the blended fee amounts instead of the proposed use of the fully
adjusted fees. The blended payments, which have been used in payment since January 2016, are
based on 50 percent of the unadjusted fee schedule amount and 50 percent of the fully adjusted
fee amounts scheduled to be implemented in July 2016. This change is being made because the
fully adjusted fees for 2016 have not yet been announced. Second, the Secretary has directed the
Office of the Actuary to adjust the fee-for-service experience for beneficiaries enrolled in Puerto
Rico to reflect the propensity of zero dollar claimants nationwide.
Medicare Advantage Employer Group Waiver Plans: We are finalizing the methodology that we
proposed for calculating EGWP county payment rates with two modifications. First, in order to
release final EGWP county payment rates in the Rate Announcement, we will use the average
bid-to-benchmark ratio for individual market plan bids from the prior payment year to calculate
the Part C base payment amounts for EGWPs. For example, the EGWP county payment rates
for 2017 have been calculated using 2016 bid-to-benchmark ratios. Second, to provide
employers and MAOs more time to adapt to this payment change, we are providing a two-year
transition to the new EGWP county payment rate methodology. More details about the final
policy are discussed in Section F of Attachment III below.
CMS-HCC Risk Adjustment Models for CY2017: We will fully implement the 2017 CMS-HCC
Risk Adjustment model proposed in the Advance Notice, but have updated the coefficients using an
updated denominator. Attachment VI contains the revised coefficients.
Normalization Factors: CMS is updating the 2017 normalization factors that were proposed in
the Advance Notice. The 2017 Normalization factors are as follows:
CMS-HCC model used for MA plans is 0.998.
CMS-HCC model used for PACE organizations is 1.051.
CMS-HCC ESRD functioning graft model is 1.051.
CMS-HCC ESRD dialysis model is 0.994.
RxHCC model is 0.976.
Encounter data as a diagnoses source for 2017: CMS will calculate 2017 risk scores by adding
25% of the risk score using encounter data and FFS diagnoses with 75% of the risk score using
RAPS and FFS diagnoses.

4
Proposals Adopted as Issued in the Advance Notice:
As in past years, policies proposed in the Advance Notice that are not modified or retracted in
the Rate Announcement become effective in the upcoming payment year. Clarifications in the
Rate Announcement supersede materials in the Advance Notice.
MA Benchmark, Quality Bonus Payments and Rebate: The Affordable Care Act (ACA)
established a new benchmark methodology beginning in 2012. In the Advance Notice we
announced the continued implementation of the methodology used to derive the benchmark
county rates, how the qualifying bonus counties will be identified, and how transitional phase in
periods were determined. The continued applicability of the star system was also announced.
This Announcement finalizes these proposals.
IME Phase Out: For 2017, CMS will continue phasing out indirect medical education amounts
from MA capitation rates.
ESRD State Rates: We will continue to determine the 2017 ESRD dialysis rates by state as we
specified in the Advance Notice.
Clinical Trials: We are continuing the policy of paying on an FFS basis for qualified clinical
trial items and services provided to MA plan members that are covered under National
Coverage Determination 310.1.
Location of Network Areas for PFFS Plans in Plan Year 2018: The list of network areas for plan
year 2018 is available on the CMS website at http://www.cms.gov/PrivateFeeforServicePlans/,
under PFFS Plan Network Requirements.
Adjustment for MA Coding Pattern Differences: We will implement an MA coding pattern
difference adjustment of 5.66 percent for payment year 2017.
Frailty Adjustment for PACE organizations and FIDE SNPs: We are finalizing the 2017 frailty
factors as proposed.
Medical Loss Ratio Credibility Adjustment: We are finalizing the credibility adjustment factors
as published in the MLR final rule (CMS-4173-F).
RxHCC Risk Adjustment Model: We will implement the updated RxHCC Risk adjustment
model proposed in the Advance Notice. Attachment VI contains the risk adjustment factors for
the RxHCC model.
Part D Risk Sharing: The 2017 threshold risk percentages and parameters for Part D risk sharing
will be finalized as stated in the Advance Notice.
Part D Benefit Parameters: Attachment V provides the 2017 Part D benefit parameters for the
defined standard benefit, low-income subsidy, and retiree drug subsidy.

5
Part D Calendar Year Employer Group Waiver Plans: We are finalizing the Part D CY EGWP
prospective reinsurance policy as proposed.
/ s /
Sean Cavanaugh
Deputy Administrator, Centers for Medicare and Medicaid Services
Director, Center for Medicare
/ s /
Jennifer Wuggazer Lazio, F.S.A., M.A.A.A.
Director
Parts C & D Actuarial Group
Office of the Actuary
Attachments
6
2017 ANNOUNCEMENT
TABLE OF CONTENTS
Subject: Announcement of Calendar Year (CY) 2017 Medicare Advantage Capitation Rates
and Medicare Advantage and Part D Payment Policies and Final Call Letter ......... 1
Key Changes from the Advance Notice: ...................................... 3
Proposals Adopted as Issued in the Advance Notice: ............................. 4
Attachment I. Final Estimates of the National Per Capita Growth Percentage and the
National Medicare Fee-for-Service Growth Percentage for Calendar Year 2017 ...... 8
Attachment II. Key Assumptions and Financial Information ......................... 10
Attachment III. Responses to Public Comments on Part C Payment Policy .............. 19
Section A. Final Estimate of the National Per Capita Growth Percentage and the Fee-
for-Service (FFS) Growth Percentage for Calendar Year 2017 ................ 19
Section B. MA Benchmark, Quality Bonus Payments and Rebate .................. 21
Section C. Calculation of Fee for Service Cost ................................ 23
Section D. ESRD Rates ................................................. 26
Section E. Clinical Trials ............................................... 26
Section F. MA Employer Group Waiver Plans ................................ 27
Section G. CMS-HCC Risk Adjustment Model for CY 2017 ..................... 44
Section H. Medicare Advantage Coding Pattern Adjustment ...................... 53
Section I. Normalization Factors .......................................... 56
Section J. Frailty Adjustment for PACE organizations and FIDE SNPs .............. 59
Section K. Encounter Data as a Diagnosis Source for 2017 ....................... 60
Attachment IV. Responses to Public Comments on Part D Payment Policy .............. 63
Section A. Update of the RxHCC Model .................................... 63
Section B. Encounter Data as a Diagnosis Source for 2017 ....................... 63
Section C. Part D Risk Sharing ........................................... 64
Section D. Medicare Part D Benefit Parameters: Annual Adjustments for Defined
Standard Benefit, Low-Income Subsidy, and Retiree Drug Subsidy in 2017 ....... 64
Section E. Part D Calendar Year Employer Group Waiver Plans ................... 65
Attachment V. Final Updated Part D Benefit Parameters for Defined Standard Benefit,
Low-Income Subsidy, and Retiree Drug Subsidy ............................ 68
Section A. Annual Percentage Increase in Average Expenditures for Part D Drugs per
Eligible Beneficiary (API) ........................................... 70
Section B. Annual Percentage Increase in Consumer Price Index (CPI) .............. 70
Section C. Calculation Methodology ....................................... 71
Section D. Retiree Drug Subsidy Amounts ................................... 74
7
Section E. Estimated Total Covered Part D Spending at Out-of-Pocket Threshold for
Applicable Beneficiaries ............................................ 74
Attachment VI. CMS-HCC and RxHCC Risk Adjustment Factors ..................... 77
Table VI-1. 2017 CMS-HCC Model Relative Factors for Community and Institutional
Beneficiaries .................................................... 78
Table VI-2. 2017 CMS-HCC Model Relative Factors for Aged and Disabled New
Enrollees ....................................................... 85
Table VI-3. 2017 CMS-HCC Model Relative Factors for New Enrollees in Chronic
Condition Special Needs Plans (C-SNPs) ................................ 86
Table VI-4. Disease Hierarchies for the 2017 CMS-HCC Model ................... 87
Table VI-5. RxHCC Model Relative Factors for Continuing Enrollees ............... 88
Table VI-6. RxHCC Model Relative Factors for New Enrollees, Non‑Low Income ..... 93
Table VI-7. RxHCC Model Relative Factors for New Enrollees, Low Income ......... 94
Table VI-8. RxHCC Model Relative Factors for New Enrollees, Institutional .......... 95
Table VI-9. List of Disease Hierarchies for RxHCC Model ....................... 96
Attachment VII: CY 2017 Final Call Letter ..................................... 97
How to Use This Call Letter ............................................... 101
Section I – Parts C and D .................................................. 102
Section II – Part C ....................................................... 156
Section III – Part D ...................................................... 186
Section IV – Medicare-Medicaid Plans........................................ 223
Medicare-Medicaid Plan Annual Requirements and Timeline for CY 2017 .......... 223
Appendix 1 – Contract Year 2017 Guidance for Prescription Drug Plan (PDP) Renewals and
Non-Renewals (Updated) ............................................ 228
Appendix 2 – Contract Year 2017 Guidance for Prescription Drug Plan (PDP) Renewals and
Non-Renewals Table ............................................... 232
Appendix 3 – Improvement Measures (Part C & D) .............................. 237
Appendix 4 - 2017 Draft Call Letter Star Ratings Summary of Comments and Responses .. 240
Appendix 5 – Adjusted Measure Selection Criteria ............................... 250

8
Attachment I. Final Estimates of the National Per Capita Growth Percentage and the
National Medicare Fee-for-Service Growth Percentage for Calendar Year 2017
The Table I-1 below shows the National Per Capita MA Growth Percentage (NPCMAGP) for
2017. We have calculated the final MA Growth Percentage and the FFS Growth Percentage
based on the assumption of a 0.5 percent update for the physician fee schedule for 2017.
An adjustment of 0.1 percent for the combined aged and disabled is included in the NPCMAGP
to account for corrections to prior years’ estimates as required by section 1853(c)(6)(C). The
combined aged and disabled change is used in the development of the ratebook.
Table I-1 - National Per Capita MA Growth Percentage for 2017
Prior Changes
Current Changes
2003 to 2016
2003 to 2016
2016 to 2017
2003 to 2017
NPCMAGP for 2017
With §1853(c)(6)(C)
adjustment
1
Aged+Disabled
50.20%
50.35%
2.98%
54.84%
3.08%
1
Current changes for 2003-2017 divided by the prior changes for 2003 to 2016.
The Affordable Care Act of 2010 requires the Medicare Advantage benchmark amounts be tied
to a percentage of the county FFS amounts. Table I-2 below provides the change in the FFS
USPCC which will be used in the development for the county benchmark. The percentage
change in the FFS USPCC is shown as the current projected FFS USPCC for 2017 divided by
projected FFS USPCC for 2016 as estimated in the 2016 Rate Announcement released on April
6, 2015.
Table I-2 – FFS USPCC Growth Percentage for CY 2017
Aged + Disabled
Dialysis –only ESRD
Current projected 2017 FFS USPCC
$825.20
$7,023.24
Prior projected 2016 FFS USPCC
$800.21
$7,155.20
Percent change
3.12%
−1.84%
Table I-3 below shows the monthly actuarial value of the Medicare deductible and coinsurance
for 2016 and 2017. In addition, for 2017, the actuarial value of deductibles and coinsurance is
being shown for non-ESRD only, since the plan bids will not include ESRD benefits in 2017.
These data were furnished by the Office of the Actuary.

9
Table I-3 - Monthly Actuarial Value of Medicare Deductible and Coinsurance for 2016 and 2017
2016
2017
Change
2017 non-ESRD
Part A Benefits
$39.57
$39.43
−0.4%
$37.52
Part B Benefits
1
$118.86
$125.73
5.8%
$116.05
Total Medicare
$158.43
$165.16
4.2%
$153.57
1
Includes the amounts for outpatient psychiatric charges.
Medical Savings Account (MSA) Plans. The maximum deductible for current law MSA plans
for 2017 is $11,650.

10
Attachment II. Key Assumptions and Financial Information
The USPCCs are the basis for the National Per Capita MA Growth Percentage. Attached is a
table that compares last year’s estimate of United States Per Capita Costs (USPCC) with current
estimates for 2003 to 2018. In addition, this table shows the current projections of the USPCCs
through 2019. We are also providing an attached set of tables that summarize many of the key
Medicare assumptions used in the calculation of the USPCCs. Most of the tables include
information for the years 2003 through 2019.
Most of the tables in this attachment present combined aged and disabled non-ESRD data. The
ESRD information presented is for the combined aged-ESRD, disabled-ESRD and ESRD only.
All of the information provided in this enclosure applies to the Medicare Part A and Part B
programs. Caution should be employed in the use of this information. It is based upon
nationwide averages, and local conditions can differ substantially from conditions nationwide.
None of the data presented here pertain to the Medicare prescription drug benefit.
Comparison of Current & Previous Estimates of the Total USPCC – Non-ESRD
Part A
Part B
Part A & Part B
Calendar
Year
Current
Estimate
Last
Year’s
Estimate
Current
Estimate
Last
Year’s
Estimate
Current
Estimate
Last
Year’s
Estimate
Ratio
2003
$296.18
296.18
$247.66
247.64
$543.84
$543.82
1.000
2004
$314.08
314.08
$271.06
271.03
$585.14
$585.11
1.000
2005
$334.83
334.83
$292.86
292.83
$627.69
$627.66
1.000
2006
$345.30
345.30
$313.70
313.67
$659.00
$658.97
1.000
2007
$355.44
355.47
$330.68
330.65
$686.12
$686.12
1.000
2008
$371.90
371.93
$351.04
351.01
$722.94
$722.94
1.000
2009
$383.93
383.89
$367.93
367.92
$751.86
$751.81
1.000
2010
$382.99
385.42
$376.82
376.84
$759.81
$762.26
0.997
2011
$389.78
389.75
$386.31
386.33
$776.09
$776.08
1.000
2012
$379.28
379.07
$392.90
392.90
$772.18
$771.97
1.000
2013
$381.32
381.24
$399.73
400.31
$781.05
$781.55
0.999
2014
$371.80
371.91
$418.58
419.91
$790.38
$791.82
0.998
2015
$372.10
369.18
$432.53
430.51
$804.63
$799.69
1.006
2016
$375.95
375.14
$441.72
441.69
$817.67
$816.83
1.001
2017
$386.02
386.12
$456.04
460.23
$842.06
$846.35
0.995
2018
$397.89
405.23
$473.50
484.64
$871.39
$889.87
0.979
2019
$410.97
$503.55
$914.52

11
Comparison of Current & Previous Estimates of the FFS USPCC – Non-ESRD
Part A
Part B
Part A & Part B
Calendar
Year
Current
Estimate
Last
Year’s
Estimate
Current
Estimate
Last
Year’s
Estimate
Current
Estimate
Last
Year’s
Estimate
Ratio
2010
$369.90
$373.09
$374.91
$374.89
$744.81
$747.98
0.996
2011
$373.81
$373.73
$384.47
$384.47
$758.28
$758.20
1.000
2012
$359.57
$359.23
$392.07
$392.02
$751.64
$751.25
1.001
2013
$365.58
$365.16
$395.99
$396.51
$761.57
$761.67
1.000
2014
$365.88
$364.88
$408.86
$409.90
$774.74
$774.78
1.000
2015
$368.23
$362.92
$426.30
$422.05
$794.53
$784.97
1.012
2016
$370.33
$368.54
$431.08
$431.67
$801.41
$800.21
1.001
2017
$378.95
$380.46
$446.25
$451.24
$825.20
$831.70
0.992
2018
$390.23
398.27
$462.98
473.81
$853.21
$872.08
0.978
2019
$402.64
$491.86
$894.50
Comparison of Current & Previous Estimates of the ESRD Dialysis-only FFS USPCC
Part A+B
Calendar
Year
Current
Estimate
Last Year’s
Estimate
Ratio
2010
$6,834.14
$6,834.14
1.000
2011
$6,770.39
$6,770.39
1.000
2012
$6,719.08
$6,719.08
1.000
2013
$6,779.61
$6,779.61
1.000
2014
$6,762.22
$6,863.06
0.985
2015
$6,815.23
$6,997.24
0.974
2016
$6,862.30
$7,155.20
0.959
2017
$7,023.24
$7,413.51
0.947
2018
$7,213.94
$7,731.47
0.933
2019
$7,455.35
Basis for ESRD Dialysis-only FFS USPCC Trend
Part A+B
Calendar
Year
All ESRD
Cumulative
FFS Trend
Adjustment
Factor for
Dialysis-
only
Adjusted
Dialysis-only
Cumulative
Trend
2015
1.0151
0.9929
1.0078
2016
1.0294
0.9858
1.0148
2017
1.0610
0.9789
1.0386
2018
1.0975
0.9720
1.0668
2019
1.1422
0.9652
1.1025

12
Summary of Key Projections
Part A
1
Year
Calendar Year
CPI Percent Change
Fiscal Year
PPS Update Factor
FY Part A Total Reimbursement
(Incurred)
2003
2.2%
3.0%
3.5%
2004
2.6%
3.4%
8.4%
2005
3.5%
3.3%
8.8%
2006
3.2%
3.7%
5.9%
2007
2.9%
3.4%
5.7%
2008
4.1%
2.7%
7.6%
2009
−0.7%
2.7%
6.7%
2010
2.1%
1.9%
3.0%
2011
3.6%
−0.6%
4.9%
2012
2.1%
−0.1%
0.5%
2013
1.4%
2.8%
4.6%
2014
1.5%
0.9%
0.5%
2015
−0.4%
1.4%
2.2%
2016
0.9%
0.9%
3.9%
2017
2.8%
1.4%
5.5%
2018
2.6%
2.8%
6.1%
2019
2.6%
2.5%
6.2%
Part B
2
Physician Fee Schedule
Calendar Year
Fees
3
Residual
4
Part B Hospital
Total
2003
1.4%
4.5%
4.4%
6.8%
2004
3.8%
5.9%
11.1%
9.8%
2005
2.1%
3.2%
10.8%
7.0%
2006
0.2%
4.6%
5.1%
6.1%
2007
−1.4%
3.5%
8.3%
4.3%
2008
−0.3%
4.0%
6.3%
4.8%
2009
1.4%
1.6%
5.7%
4.0%
2010
2.3%
1.6%
6.6%
2.4%
2011
0.8%
2.3%
7.1%
2.3%
2012
−1.2%
1.0%
7.3%
1.7%
2013
−0.1%
0.2%
7.4%
0.8%
2014
0.5%
0.7%
12.6%
3.4%
2015
−0.4%
1.0%
6.0%
2.3%
2016
−0.4%
−0.6%
2.8%
1.6%
2017
0.4%
2.2%
8.0%
3.4%
2018
−0.3%
2.9%
7.2%
3.2%
2019
0.6%
6.3%
7.7%
6.0%
1
Percent change over prior year
2
Percent change in charges per Aged Part B enrollee.
3
Reflects the physician update and all legislation affecting physician services—for example, the addition of new preventative services enacted in
1997, 2000, and 2010.
4
Residual factors are factors other than price, including volume of services, intensity of services, and age/sex changes.

13
Medicare Enrollment Projections (In Millions)
Non-ESRD Total
Part A
Part B
Calendar Year
Aged
Disabled
Aged
Disabled
2003
34.437
5.961
33.038
5.215
2004
34.849
6.283
33.294
5.486
2005
35.257
6.610
33.621
5.776
2006
35.795
6.889
33.975
6.017
2007
36.447
7.167
34.465
6.245
2008
37.378
7.362
35.140
6.438
2009
38.257
7.574
35.832
6.664
2010
39.091
7.832
36.516
6.938
2011
39.930
8.163
37.229
7.247
2012
41.666
8.403
38.526
7.496
2013
43.066
8.620
39.759
7.725
2014
44.516
8.733
41.041
7.879
2015
45.714
8.712
42.280
7.926
2016
47.514
8.749
43.616
7.951
2017
49.089
8.788
44.992
7.991
2018
50.709
8.866
46.419
8.056
2019
52.395
8.937
47.894
8.121
Non-ESRD Fee for Service
Part A
Part B
Calendar Year
Aged
Disabled
Aged
Disabled
2003
29.593
5.628
28.097
4.875
2004
29.946
5.931
28.300
5.128
2005
30.014
6.178
28.287
5.339
2006
29.365
6.146
27.462
5.267
2007
28.838
6.226
26.782
5.297
2008
28.613
6.241
26.301
5.311
2009
28.563
6.288
26.071
5.374
2010
28.903
6.455
26.261
5.556
2011
29.190
6.650
26.421
5.730
2012
29.940
6.685
26.724
5.772
2013
30.309
6.683
26.928
5.783
2014
30.586
6.576
27.038
5.718
2015
30.751
6.349
27.243
5.559
2016
31.721
6.246
27.748
5.445
2017
32.427
6.165
28.251
5.364
2018
33.255
6.134
28.882
5.321
2019
34.159
6.097
29.571
5.278

14
ESRD
ESRD-Total
ESRD-Fee for Service
Calendar Year
Total Part A
Total Part B
Total Part A
Total Part B
2003
0.340
0.331
0.319
0.309
2004
0.353
0.342
0.332
0.321
2005
0.366
0.355
0.344
0.332
2006
0.382
0.370
0.353
0.340
2007
0.396
0.383
0.361
0.347
2008
0.411
0.397
0.367
0.353
2009
0.426
0.412
0.374
0.360
2010
0.442
0.428
0.388
0.373
2011
0.456
0.441
0.398
0.383
2012
0.471
0.455
0.408
0.393
2013
0.483
0.468
0.414
0.398
2014
0.495
0.480
0.416
0.401
2015
0.504
0.489
0.415
0.400
2016
0.514
0.500
0.419
0.404
2017
0.525
0.511
0.424
0.410
2018
0.536
0.522
0.432
0.417
2019
0.548
0.533
0.438
0.424
Part A Projections for non-ESRD (Aged+Disabled)
Calendar
Year
Inpatient Hospital
Aged + Disabled
SNF
Aged + Disabled
Home Health
Aged + Disabled
Managed Care
Aged + Disabled
Hospice: Total
Reimbursement
(in Millions)
Aged + Disabled
2003
2,594.78
370.63
124.28
457.87
5,733
2004
2,714.57
413.44
133.89
500.73
6,832
2005
2,818.21
450.54
140.87
602.29
8,016
2006
2,764.82
475.07
141.30
757.20
9,368
2007
2,707.49
504.24
143.72
905.77
10,518
2008
2,695.88
536.68
151.00
1,075.01
11,404
2009
2,651.47
551.67
153.86
1,246.31
12,274
2010
2,615.34
571.72
155.17
1,250.04
13,126
2011
2,602.24
624.93
143.61
1,300.70
14,034
2012
2,504.45
543.60
136.02
1,360.79
15,045
2013
2,493.61
542.29
133.48
1,400.15
15,466
2014
2,430.53
536.00
128.47
1,360.42
15,506
2015
2,377.54
545.49
124.77
1,411.88
16,212
2016
2,354.83
559.05
124.16
1,469.13
17,264
2017
2,368.01
579.59
125.79
1,554.41
18,522
2018
2,416.83
594.39
128.29
1,630.61
19,713
2019
2,471.56
617.19
133.78
1,713.00
21,218
Average reimbursement per enrollee on an incurred basis, except where noted. Does not reflect the effects of the Independent Payment Advisory
Board (IPAB)

15
Part B Projections for non-ESRD (Aged+Disabled)
Calendar Year
Physician Fee Schedule
Aged + Disabled
Part B Hospital
Aged + Disabled
Durable Medical Equipment
Aged + Disabled
2003
1226.49
364.77
196.96
2004
1343.99
418.85
195.61
2005
1397.41
477.65
196.83
2006
1396.39
497.47
197.78
2007
1368.35
526.92
195.68
2008
1367.83
555.09
200.92
2009
1375.29
592.77
183.61
2010
1413.77
628.55
183.76
2011
1440.63
668.61
175.58
2012
1396.64
704.50
173.34
2013
1353.67
743.47
152.30
2014
1334.67
820.85
128.34
2015
1338.07
857.87
134.19
2016
1312.82
871.92
126.40
2017
1320.19
925.58
123.34
2018
1356.84
982.07
129.93
2019
1444.54
1047.00
135.51
Calendar Year
Carrier Lab
Aged + Disabled
Other Carrier
Aged + Disabled
Intermediary Lab
Aged + Disabled
2003
73.73
329.81
75.18
2004
78.48
354.00
80.47
2005
82.71
362.81
84.16
2006
85.59
361.08
84.51
2007
90.65
363.52
84.38
2008
94.50
366.62
85.78
2009
101.80
385.20
79.19
2010
101.08
393.78
80.23
2011
102.08
406.81
83.19
2012
109.62
409.90
84.59
2013
109.51
409.29
81.78
2014
115.06
411.27
55.54
2015
118.87
416.70
56.21
2016
121.56
417.19
57.02
2017
117.81
423.92
54.73
2018
121.55
437.75
56.36
2019
125.25
451.37
58.09
Average reimbursement per enrollee on an incurred basis, except where noted. Does not reflect the effects of the Independent Payment Advisory
Board (IPAB)

16
Calendar Year
Other Intermediary
Aged + Disabled
Home Health
Aged + Disabled
Managed Care
Aged + Disabled
2003
113.99
136.75
421.40
2004
119.58
156.45
471.37
2005
139.78
179.44
560.31
2006
142.09
202.88
769.94
2007
151.16
232.33
931.18
2008
158.20
252.43
1104.26
2009
187.44
282.09
1203.83
2010
193.08
283.25
1221.65
2011
198.45
262.37
1277.69
2012
205.00
246.82
1368.93
2013
194.42
240.61
1498.09
2014
200.16
233.22
1709.38
2015
212.72
225.54
1816.00
2016
216.96
225.75
1936.62
2017
224.74
228.79
2038.46
2018
193.46
233.49
2155.04
2019
200.11
243.61
2333.89
Average reimbursement per enrollee on an incurred basis, except where noted. Does not reflect the effects of the Independent Payment Advisory
Board (IPAB)
2017 Projections by Service Category for non-ESRD (Aged+Disabled)*
Service Type
Current
Estimate
Last Year’s
Estimate
Ratio
Part A
Inpatient Hospital
2,368.01
2,364.02
1.002
SNF
579.59
591.47
0.980
Home Health
125.79
130.30
0.965
Managed Care
1,554.41
1,542.97
1.007
Part B
Physician Fee Schedule
1320.19
1,342.86
0.983
Part B Hospital
925.58
978.42
0.946
Durable Medical Equipment
123.34
118.56
1.040
Carrier Lab
117.81
116.00
1.016
Other Carrier
423.92
413.41
1.025
Intermediary Lab
54.73
55.41
0.988
Other Intermediary
224.74
183.63
1.224
Home Health
228.79
240.83
0.950
Managed Care
2038.46
2,060.97
0.989
Average reimbursement per enrollee on an incurred basis, except where noted.

17
Claims Processing Costs as a Fraction of Benefits
Calendar
Year
Part A
Part B
2003
0.001849
0.011194
2004
0.001676
0.010542
2005
0.001515
0.009540
2006
0.001245
0.007126
2007
0.000968
0.006067
2008
0.000944
0.006414
2009
0.000844
0.005455
2010
0.000773
0.005055
2011
0.000749
0.004396
2012
0.001008
0.003288
2013
0.000994
0.002846
2014
0.001003
0.002884
2015
0.000952
0.002730
2016
0.000952
0.002730
2017
0.000952
0.002730
2018
0.000952
0.002730
2019
0.000952
0.002730
Approximate Calculation of the USPCC, the National MA Growth Percentage for
Combined (Aged+Disabled) Beneficiaries, and the FFS USPCC (Aged+Disabled)
The following procedure will approximate the actual calculation of the USPCCs from the
underlying assumptions for the contract year for both Part A and Part B.
Part A:
The Part A USPCC can be approximated by using the assumptions in the tables titled “Part A
Projections Under Present Law for non-ESRD (Aged+Disabled)” and “Claims Processing Costs
as a Fraction of Benefits.” Information in the “Part A Projections” table is presented on a
calendar year per capita basis. First, add the per capita amounts over all types of providers
(excluding hospice). Next, multiply this amount by 1 plus the loading factor for administrative
expenses from the “Claims Processing Costs” table. Then, divide by 12 to put this amount on a
monthly basis.
Part B:
The Part B USPCC can be approximated by using the assumptions in the tables titled “Part B
Projections under Present Law for non-ESRD (Aged+Disabled)” and “Claims Processing Costs
as a Fraction of Benefits.” Information in the “Part B Projections” table is presented on a
calendar year per capita basis. First, add the per capita amounts over all types of providers.
Next, multiply by 1 plus the loading factor for administrative expenses and divide by 12 to put
this amount on a monthly basis.

18
The National Per Capita MA Growth Percentage:
The National Per Capita MA Growth Percentage for 2017 (before adjustment for prior years’
over/under estimates) is calculated by adding the USPCCs for Part A and Part B for 2017 and
then dividing by the sum of the current estimates of the USPCCs for Part A and Part B for 2016.
The FFS USPCC:
The tables used to calculate the total USPCC can also be used to approximate the calculations of
the FFS USPCC. The per capita data presented by type of provider in the projections tables for
both Part A and B are based on total enrollment. To approximate the FFS USPCCs, first add the
corresponding provider types under Part A and Part B separately. For the FFS calculations, do
not include the managed care provider type. Next, rebase the sum of the per capita amounts for
FFS enrollees, i.e., multiply the sum by total enrollees and divide by FFS enrollees. (The
enrollment tables in this attachment now also include FFS enrollment). Then, multiply by 1 plus
the loading factor for administrative expenses and divide by 12. The result will only be
approximate because there is an additional adjustment to the FFS data which accounts for cost
plan data which comes through the FFS data system. This cost plan data is in the total per capita
amounts by type of provider, but is removed for the FFS calculations.

19
Attachment III. Responses to Public Comments on Part C Payment Policy
Section A. Final Estimate of the National Per Capita Growth Percentage and the Fee-for-
Service (FFS) Growth Percentage for Calendar Year 2017
Comment: One commenter thanked CMS for providing timely data, including preliminary
estimates of the growth rates.
Response: CMS appreciates the support and will continue to provide timely data when possible.
Comment: CMS received one comment expressing appreciation for the details provided on the
factors used in the calculation of the growth rates.
Response: CMS appreciates the support.
Comment: Commenters requested more transparency regarding the calculation of the growth
rate. Commenters requested that CMS provide plans with a full explanation of the methodology
and assumptions underlying the growth rate, so that plans can conduct careful analysis and
provide meaningful comment
Response: We believe that we are providing useful information and support pertaining to
USPCC levels and trends. Key economic assumptions underlying the USPCCs are included in
attachment II of this payment notice. Consistent with prior years, we will publish additional
information regarding trends for the prior five years at https://www.cms.gov/Medicare/Health-
Plans/MedicareAdvtgSpecRateStats/FFS-Trends.html and will discuss this material on an
actuarial user group call.
Comment: One commenter requested an explanation on why the National Health Expenditures
forecasts show 3.3% per enrollee spending growth for Medicare in 2017, while the CMS
projected benchmark growth is lower than this.
Response: A key difference between the two baselines is that that total USPCC growth rate is
based on more complete historical experience than the NHE. Other differences between the
projections include the treatment of hospice benefits, covered population (e.g., ESRD),
administrative costs, sequestration, and bonuses for use of electronic health records.
Comment: Two commenters expressed concern that there may be significant adjustments
between the growth rate in the Advance Notice and the growth rate in the Rate Announcement,
as there has been in previous years. These commenters requested that CMS work to prevent
adjustments in order to avoid disruption to the MA program.
Response: Each release of the growth rates reflects our best estimate at that time of historical
program experience and projected trend. We always strive to improve our forecasting accuracy
with incorporation of additional data and the refinement of our analytic modeling.

20
Comment: One commenter asked that CMS not make any major adjustments to the growth rate
in the Rate Announcement because plans will not have a chance to review the changes and
provide comments. This commenter also suggested that CMS review all of its assumptions,
including any changes in assumptions from prior years, in order to avoid disruption in the MA
program.
Response: The growth percentages and total USPCC and FFS USPCCs reflected in Attachment
II of this payment announcement are based on the Office of the Actuary’s (OACT’s) best
estimate of historical project experience and program trend. We continue to believe that the best
practice is to base the growth rates on the most recent data and assumptions.
Comment: CMS received one comment asking for clarification on the meaningfulness of the
MA growth percentage now that all counties are phased in. This commenter requested that CMS
clarify whether the FFS growth percentage is now the driving number and if the MA growth rate
percentage will now only be used for calculating the benchmark cap. This commenter also
suggests that CMS present the FFS growth percentage before the MA growth percentage.
Response: The specified amounts, or FFS rates, are based on the FFS USPCC. Also, the
applicable amount, or pre-Affordable Care Act rate, established under SSA section 1853(k)(1) is
updated by the growth in the total USPCC. We will consider modifying the presentation of the
USPCCs and growth rates in future rate announcements.
Comment: Several commenters expressed concern that the ESRD growth rate is significantly
lower than the FFS and MA growth rates. Commenters requested additional information and
explanation for this difference. Commenters stated that they are worried that this negative
growth rate will have adverse effects on beneficiaries.
Response: The preliminary CY 2017 growth rate for the ESRD population reflects a prior period
adjustment of −4.35 percent. This adjustment is primarily due to lower experience for the
dialysis population for calendar year 2014 combined with a negative differential in the growth
rate in 2015 and 2016 between the total ESRD and dialysis-only populations. The increase from
2016 to 2017 tabulated on the current baseline is 2.04 percent. Combining the prior period
update of −4.35 percent and the current trend of 2.04 percent yields the preliminary 2017 ESRD
growth rate of −2.39 percent.
Also, we agree that the negative ESRD FFS USPCC update for 2017 could have an adverse
effect on beneficiary premiums and/or supplemental benefits. We encourage plan sponsors to
take into account beneficiary impacts in their design of 2017 MA and MA-PD plan benefits,
consistent with CMS’ policies.
Comment: Two commenters noted that ESRD rates have fluctuated from year to year. These
commenters stated that it is unclear why there would be such significant oscillation. These two
commenters stated that the fluctuation in ESRD rates make it difficult for plans to design and

21
maintain stable benefit packages, especially for such a vulnerable population. The commenters
requested that CMS provide additional details behind the significant year to year oscillations in
the ESRD calculations, as well as review the rates for accuracy.
Response: We agree that predictable growth rates for the ESRD population are important to
Medicare Advantage plans that cover the ESRD population. The recent trend in ESRD
population reflects several recent program changes including the bundling of Part B services,
audits conducted by Recovery Audit Contractors, the “two midnight” hospital policy, and the
implementation of DMEPOS competitive bidding.
Section B. MA Benchmark, Quality Bonus Payments and Rebate
Comment: Several commenters expressed concern that the pre-ACA rate cap penalizes high
quality plans and plans that offer services in higher-cost areas. Commenters suggested that CMS
review its options for exercising discretionary authority to remove the quality bonuses from the
benchmark cap calculation. One commenter believes that including the bonus in the cap
calculation contradicts the intent of Congress to provide quality bonuses to high performing
plans and to establish a value-based purchasing component in MA. Commenters believe that the
statute can be interpreted to allow the Secretary the discretion to exclude quality bonuses from
the benchmark cap calculation. One commenter indicated that the language used in section
1853(n)(4) refers to “taking into account” the quality bonuses, suggesting that the Secretary
could consider the quality bonus payments but then exercise discretion to omit them from the cap
calculation. Another commenter suggested that the Applicable Amount was a cap on the
blended benchmarks only during the Applicable Amount’s phase-out period; and since the
Applicable Amount is no longer included in the benchmark calculation, the statute does not
require the cap to remain in place for 2017.
Response: CMS shares the commenters’ concern about any rate-setting mechanism that
diminishes incentives for MA plans to continuously improve the care provided to Medicare
beneficiaries. While we appreciate the concerns of commenters, we do not believe we have the
discretion under section 1853(n)(4) of the Social Security Act to eliminate application of the pre-
ACA rate cap or exclude the bonus payment from the cap calculation. The bonus payment is
based on an increase to the “applicable percentage” which is a component of the benchmark
calculation itself. Further, the plain reading of the statute does not indicate congressional intent
to limit the benchmark cap to the transition period described in section 1853(n)(3) of the Act.
When Congress has wanted to authorize or mandate MA payment rules that apply for specific
periods of time, Congress has done so using specific date parameters; section 1853 of the Act
includes numerous examples of this.
Comment: One commenter requested clarification regarding quality bonus payments for low
enrollment plans. The commenter questioned whether quality bonus payments for low

22
enrollment plans should be based on an enrollment-weighted average of the Star Ratings earned
by the parent organization’s existing MA contracts.
Response: Section 1853(o)(3)(A)(ii) does not address the amount of the quality bonus payment
increase for low enrollment contracts. We interpret section 1853(o)(3) of the Act as establishing
two types of qualifying plans for purposes of applying the quality bonus, with the amount of the
quality bonus determined by the basis for treatment of the plan as a qualifying plan (i.e., whether
the amount is based on the score produced under the Star Rating system or based on the default
increase specified in the case of new MA plans). For the purpose of determining a quality bonus
percentage, the Advance Notice uses the term “new MA plan” to refer to an MA plan offered by
a parent organization that has not had another MA contract in the preceding three-year-period.
As discussed in the Advance Notice, we treat new MA plans and low enrollment plans (i.e.,
plans offered under a contract that lacks sufficient enrollment and data for the calculation of a
Star Rating) as qualifying plans that are eligible to receive a 3.5 percentage point quality bonus
percentage increase to the county rates. We believe that new MA plans and low enrollment
plans should receive the same treatment for the purpose of establishing the amount of quality
bonus payments because each type of plan has insufficient data available for the calculation of a
Star Rating. This is consistent with our treatment of low enrollment contracts for purposes of
determining the rebate available to the plan.
Comment: Two commenters suggested that CMS establish a minimum benchmark level for
counties in Puerto Rico, such as maintaining the MA benchmarks in Puerto Rico at previous
levels.
Response: We appreciate the concerns raised by the commenters. However, we do not believe
the approach suggested by these comments would be permissible under statute.
Comment: One commenter suggested that CMS reevaluate Puerto Rico’s eligibility for the
Qualifying County Bonus Payment. The commenter noted that, in 2016, Puerto Rico was the
only jurisdiction where all of its counties achieved two of the three conditions required to be
considered a qualifying county. The one criterion that Puerto Rico did not meet was that 2004
MA capitation must have been based on the amount specified in section 1853(c)(1)(B) for a
Metropolitan Statistical Area with a population of more than 250,000. While Puerto Rico has the
highest level of MA penetration in the nation (over 75%), the commenter believes that Puerto
Rico is disadvantaged by its population being divided into an unusually high number of counties
(78). The commenter suggested that CMS evaluate Puerto Rico’s eligibility for the Qualifying
County Bonus Payment by considering population counts by the Census Bureau’s Metropolitan
Areas (rather than by county), or by removing one of the three qualifying criteria for Puerto
Rico.
Response: We appreciate the concerns raised by the commenter. However, we do not believe the
approach suggested by these comments would be permissible under statute.

23
Section C. Calculation of Fee for Service Cost
Comment: Several commenters expressed concern regarding CMS rebasing in 2017 due to rate
unpredictability and fluctuation. Commenters noted that rebasing has occurred every year since
2012, and noted that it is not required annually by statute. One commenter proposed rebasing
FFS county rates every other year. A few commenters asked that CMS institute a regular
schedule of rebasing once every three years. Two commenters suggested that CMS adopt a
corridor to smooth the rebasing fluctuations whereby county benchmarks would be prevented
from increasing or decreasing by more than a specified amount.
Response: Given that MA county rates are based on FFS costs, we believe it is important to
update the FFS rates using the most current FFS data available. We stated in previous Rate
Announcements that we anticipate rebasing each year as a result. We do not believe that
“smoothing” the impacts of rebasing would be consistent with the statute’s requirement of
calculating the specified amount based on the estimated FFS rate for that county. We also note
that our method for calculating the county level rates includes a five-year average that provides
some measure of stability in the rates.
Comment: One commenter offered support for including shared savings and losses incurred
under the Medicare Shared Savings Program (MSSP) and Pioneer ACO programs. The
commenter requested that CMS consider including additional adjustments for other CMS/CMMI
programs, such as the Comprehensive Primary Care Initiative.
Response: We appreciate the support regarding the inclusion in the fee-for-service experience the
shared savings payment and shared losses made to MSSP and Pioneer ACOs. We recognize that
there are other CMS/CMMI programs with incentive payments for the years 2010-2014. Such
programs include the Comprehensive Primary Care Initiative, Physician Group Practice
Demonstration, and the Independence at Home Demonstration. Incentive payments made under
these programs are small relative to the MSSP and Pioneer ACO programs. Due to operational
challenges, CMS will not reflect the payments made under these programs in the CY 2017
ratebook. We will consider including payments made under additional CMS/CMMI programs in
future years.
Comment: One commenter requested more transparency on the calculation of the FFS rates, by
releasing county-level FFS costs of the most recent 5-year period. A few commenters requested
that information related to rebasing be released with the Advance Notice. One commenter asked
for additional information pertaining to the adjustment for care through the Veterans Health
Administration.
Response: We are publishing with the final Rate Announcement files that contain the wage
indices in each claim year (i.e., 2010-2014), and the wage indices for 2016 by county. We
annually publish, with the final Rate Announcement, files that contain the county-level
adjustments that are applied to the FFS costs, including the adjustment for Veterans Affairs. We

24
will consider publishing additional data with the Advance Notice in future years that can help
stakeholders understand the potential impacts of proposed changes in the Advance Notice.
Comment: One commenter requested that CMS apply a uniform approach in all counties to
calculate benchmarks on beneficiaries with both Part A and Part B coverage, as is currently done
in Puerto Rico. The commenter noted that other counties beyond Puerto Rico, such as in Hawaii,
have high MA penetration rates and low FFS Part B enrollment.
Response: While most Medicare beneficiaries are automatically enrolled in Part B and must opt
out to decline it, beneficiaries in Puerto Rico must take affirmative action to opt-in to Part B
coverage. As a result, CMS believes it is appropriate to adjust the FFS rate calculation in Puerto
Rico used to determine MA rates so that it is based on beneficiaries who are enrolled in both Part
A and Part B. We will consider expanding this Part A and Part B adjustment to all counties in the
future.
Comment: A few commenters expressed concern regarding the change of data source for county
designation of beneficiaries used in the summarization of risk scores. Commenters requested
that CMS provide more information regarding this change (such as information pertaining to the
accuracy of each data source, the mismatch rate between the two sources, and county-level
impacts of switching data sources).
Response: The change in county source for the risk score assignment will align the county codes
used to assign risk scores, claims, and enrollment. Based on the CY 2016 ratebook county
codes, risk score changes for 88 percent of the counties were within 2 percent. Further, only 5
percent of the counties had a change in risk score of greater than 5 percent due to the change in
the source of the beneficiary’s county code.
Comment: In the Advance Notice, CMS sought public comment on the possibility of adjusting
FFS experience in Puerto Rico to reflect the propensity of zero claimants nationwide. Several
commenters requested that CMS make an adjustment to the Puerto Rico MA rates to reflect the
prevalence of zero-dollar-claimants. Commenters reiterated that there is a larger proportion of
FFS Medicare beneficiaries in Puerto Rico with coverage for Medicare Parts A and B that have
no Medicare claim reimbursements compared to other jurisdictions, which they believe is
skewing the rate calculation for Puerto Rico. Commenters suggested that, to make such an
adjustment, CMS should identify beneficiaries with zero Medicare claim experience over 24
consecutive months (i.e., zero claims during a two-year period), and exclude these zero-claim
beneficiaries (and their risk score) when developing per capita costs. Commenters propose that
CMS would then apply an adjustment for the zero-claim beneficiaries.
Response: The Secretary has directed the Office of the Actuary to adjust the fee-for-service
experience for beneficiaries enrolled in Puerto Rico to reflect the propensity of zero dollar
claimants nationwide. For purposes of making this adjustment, consistent with the Secretary’s

25
instructions, the Office of the Actuary evaluated experience exclusively for beneficiaries that are
enrolled in both Parts A and B and are not dually eligible for VA coverage.
The study analyzed experience for calendar years 2011 through 2013 and only considered FFS
beneficiaries enrolled mid-year. On average, 14.3 percent of A&B Puerto Rico FFS
beneficiaries were found to have no Medicare claim reimbursements per year. This compares to
a nationwide, non-territory, proportion of 6.1 percent of FFS beneficiaries without Medicare
spending. These results were applied to the Puerto Rico FFS experience by adjusting the
weighting of the enrollment and risk scores for the zero-claim cohort to reflect the nationwide
proportion of zero-claim beneficiaries. The resulting impact was an average increase in the
standardized FFS costs in Puerto Rico of 4.4 percent for 2011 through 2013. Accordingly, a 4.4
percent adjustment was applied to the pre-standardized Puerto Rico FFS rates supporting the CY
2017 ratebook development.
Comment: A few commenters believe that FFS experience is not sufficient to establish accurate
MA benchmarks in Puerto Rico. Commenters expressed concern that FFS data used by CMS to
set the MA rates for Puerto Rico are not representative of the population to which rates are
applied, citing the lower dual-eligible penetration in FFS than exists in MA. Commenters noted
the low level of FFS enrollment in Puerto Rico, and furthermore noted that the FFS costs in
Puerto Rico appear to have low levels of health care utilization. Commenters suggested that
CMS not rebase rates in Puerto Rico for 2017 while there are concerns regarding the data used to
set MA benchmarks. One commenter requested that CMS use another jurisdiction as a proxy to
set benchmarks in Puerto Rico.
Response: We appreciate the concerns commenters have raised regarding Puerto Rico. As
explained in the Advance Notice, CMS believes that the FFS data in Puerto Rico is sufficient for
establishing accurate MA benchmarks as well as consistent with the statutory requirements. We
will continue to analyze these issues and consider whether any refinements to the methodology
may be warranted in future years.
Comment: One commenter requested that CMS adjust MA rates to account for anticipated
changes in Part A (SSI eligible simulation for Uncompensated Care) and Part B (Practice
Expense GPCI) rates through CMS rulemaking. The commenter noted that, as part of the FY
FFS rulemaking process, two specific issues are still being evaluated that could generate Part A
and Part B rate increases in the FFS program of Puerto Rico starting October 1st 2016 (Part A)
and January 1st 2017 (Part B). The commenter mentioned the timing of the rulemaking process
versus 2017 rate-setting, and was concerned about a potential imbalance in MA 2017 payments
if no adjustment were made to FFS costs.
Response: Consistent with prior years, we have adjusted the historical ratebook FFS data to
reflect payment parameters that are finalized at time of the Rate Announcement. Accordingly,
the CY 2017 ratebook repricing reflects the latest regulations for fiscal year 2016 (for example:

26
inpatient hospital, outpatient hospital, and skilled nursing facilities) and calendar year 2016 (for
example: geographic practice cost index, and DMEPOS payment schedules). Further, the Puerto
Rico inpatient hospital claims have been repriced to reflect the provisions of the Consolidated
Appropriations Act, 2016.
Comment: Two commenters expressed support regarding developing rates in Puerto Rico based
on claims and enrollment for beneficiaries with Part A eligibility and Part B enrollment. A few
commenters expressed support regarding the re-pricing of historical inpatient claims to include
the recent legislation that increased the Medicare inpatient payment rates for hospitals in Puerto
Rico.
Response: We appreciate the support.
Section D. ESRD Rates
Comment: Two commenters expressed concern regarding the volatility of the ESRD rates, citing
the decrease from the 2017 projection in the 2016 Rate Announcement. One of the commenters
suggested several rate-setting options such as not allowing ESRD rates to drop below the
previous year’s rate and/or carving-out organ acquisition costs from the ESRD rate.
Response: We appreciate the concerns the commenters raised. However, we do not believe the
approach suggested by these comments would be permissible under statute.
Section E. Clinical Trials
Comment: One commenter opposed our proposal to continue to pay on a fee-for-service basis
for qualified clinical trial items and services provided to MA enrollees in clinical trials that are
covered under the National Coverage Determinations (NCDs) on clinical trials. The commenter
recommended that we require MA plans to cover the cost of clinical trials. The commenter
incorrectly stated that, under CMS’ current policy, beneficiaries who wish to participate in
clinical trials are forced to relinquish their MA coverage and switch to FFS Medicare, where they
would be required to cover all deductibles, copays, and the 20 percent coinsurance for all charges
associated with clinical trial care. The commenter stated that this policy creates a disincentive
for Medicare enrollees with serious or life-threatening diseases, such as cancer, who may benefit
from innovative treatments and health care services through clinical trials. The commenter
indicated that, if individuals are discouraged from participating in clinical trials for cost reasons,
it will be more difficult for physicians to appropriately assess the therapeutic value of new drugs
and devices in the Medicare population until they are available in the general marketplace.
Response: As we stated in the Advance Notice, MA enrollees are able to participate in any
qualifying clinical trial that is open to beneficiaries in original Medicare. CMS does not require
MA enrollees to disenroll from their MA plan if they wish to participate in a clinical trial.
27
We note that our policy of paying on a fee-for-service basis for qualified clinical trial items and
services provided to MA enrollees only applies to clinical trials that meet the criteria to qualify
for coverage under the National Coverage Determination (NCD) for Routine Costs in Clinical
Trials (310.1) (Medicare NCD Manual, Pub. 100-3, Part 4, Section 310.1). CMS has previously
made the determination that all clinical trials that qualify for coverage under NCD 310.1 trigger
the significant cost threshold such that coverage and payment are controlled by 42 CFR
422.109(c). With respect to individual NCDs requiring coverage with evidence development
(CED), MAOs are responsible for covering items and services in CMS-approved clinical trials
that meet the requirements defined in the NCD, unless CMS determines, for each NCD, that the
significant cost threshold is exceeded for that item or service (see § 422.109).
We do not believe that our current policy creates a disincentive for MA enrollees to participate in
clinical trials, or that MA enrollees would have a greater incentive to participate in clinical trials
if MAOs were responsible for costs of qualified clinical trial items and services that are currently
covered on an FFS basis in clinical trials that qualify for coverage under NCD 310.1. Under our
clinical trials policy, for CY 2011 and subsequent years, MAOs must reimburse enrollees for the
difference between the FFS cost sharing for covered clinical trial services and the plan’s in-
network cost sharing for services of the same type, and the member’s cost sharing liabilities must
count towards the MA plan’s in-network out-of-pocket maximum. This cost-sharing
requirement applies to all qualifying clinical trials; MAOs cannot choose the clinical trials or
clinical trial items and services for which this policy applies. The requirement that MAOs
provide in-network cost-sharing for all qualifying clinical trials services means, in effect, that
MA plan enrollees incur the same cost-sharing for clinical trials services that they would incur if
the services were covered by the MAO, rather than by FFS Medicare. As we stated in the CY
2011 Rate Announcement, we believe this policy increases MA enrollees’ participation in, and
access to, clinical trial services.
For more information on these policies, please refer to the Medicare Managed Care Manual, Pub.
100-16, Chapter 4 (Benefits and Beneficiary Protections), section 10.7 (Clinical Trials).
Section F. MA Employer Group Waiver Plans
We are finalizing the methodology that we proposed for calculating EGWP county payment rates
with two modifications. First, in order to release final EGWP county payment rates in the Rate
Announcement, we will use the average bid-to-benchmark ratio for individual market plan bids,
including RPPOs, from the prior payment year to calculate the Part C base payment amounts for
EGWPs. For example, the EGWP county payment rates for 2017 have been calculated using
2016 bid-to-benchmark ratios. Second, to provide employers and MAOs more time to adapt to
this payment change, we are providing a two-year transition to the new EGWP county payment
rate methodology. Under this approach, for 2017, we have moderated the impact of the new
policy by blending individual market plan and EGWP bids to calculate the bid-to-benchmark

28
ratios (as described below). In 2018, we will fully implement the new policy and, therefore, will
use only individual market plan bids to calculate the bid-to-benchmark ratios.
We are finalizing the following methodology for calculating EGWP county payment rates:
First, a weighted average bid-to-benchmark ratio for the prior payment year is calculated
at the quartile
1
level.
o For 2017, the bid-to-benchmark ratio has been calculated using a blend of
individual market plan bids and EGWP bids from 2016, with individual market
plan bids weighted by 50 percent and EGWP bids weighted by 50 percent. The
calculation is: [(weighted average of the intra-service area rate adjustment (ISAR)
adjusted county bid amounts for individual market plan bids by actual
enrollment)/(weighted average of the county standardized benchmarks for
individual market plan bids by actual enrollment)] x 50% plus [(weighted average
of the intra-service area rate adjustment (ISAR) adjusted county bid amounts for
EGWP bids by actual enrollment)/(weighted average of the county standardized
benchmarks for EGWP plan bids by actual enrollment)] x 50% = percentage by
quartile.
2
o For 2018 and future years, the bid-to-benchmark ratios will be calculated using
individual market plan bids only. The calculation will be: (weighted average of
the intra-service area rate adjustment (ISAR) adjusted county bid amounts by
actual enrollment)/(weighted average of the county standardized benchmarks by
actual enrollment) = percentage by quartile.
2
The percentages are applied to each of the published 5%, 3.5% and 0% bonus county
ratebook rates for the payment year to establish Part C base payment amounts for EGWPs
based on their star rating for each county.
In order to calculate a county rebate payment, each county level EGWP Part C base
payment amount is compared to the corresponding published 5%, 3.5% and 0% bonus
county benchmarks for the payment year to determine the amount of savings. The savings
1
As described in more detail in the Advance Notice, to determine the CY 2017 applicable
percentages, CMS ranks counties from highest to lowest based upon their 2016 average per
capita FFS costs and places the rates into four quartiles. When calculating the bid-to-benchmark
ratios CMS grouped them by the 2016 unblended quartiles, these bid-to-benchmark ratios are
then applied to the 2017 unblended quartiles.
2
Territories will not be included in the weighted average bid-to-benchmark ratio, but will be
assigned the weighted average of the quartile within which their counties fall.

29
amount is multiplied by the corresponding star rebate percentage to determine the Part C
EGWP county level rebate amount.
The EGWP Part C base payment amount is added to the Part C EGWP rebate amount to
establish the county level EGWP total payment amount.
The total payment amount will be risk adjusted in payment using beneficiary-specific risk
scores. Therefore, the formula applied for payment will be: (base county payment rate +
county rebate) * beneficiary level risk score
For RPPO EGWPs, the weighted average bid-to-benchmark ratios will be calculated as described
in the first bullet above, then, as described in the Advance Notice, to establish the Part C base
RPPO EGWP payment amount, we would also apply the same methodology as described above
in the second bullet. In order to calculate the regional rebate amounts, these percentages will be
applied for each county within a region to the published payment year regional benchmarks to
establish the savings amount and rebate amounts by star rating and quartile. So the formula
applied for payment for RPPO EGWPs would be: (base county payment rate + regional rebate) ×
beneficiary level risk score. As stated in the Advance Notice, the final MA regional standardized
A/B benchmarks released in late summer will reflect the average bid component of the regional
benchmark based on non-EGWP bid submissions.
The 2017 county payment rates for non-RPPO EGWPs can be found at:
https://www.cms.gov/Medicare/Health-Plans/MedicareAdvtgSpecRateStats/Ratebooks-and-
Supporting-Data.html. The 2017 EGWP RPPO payment rates will be released concurrently with the
2017 Regional MA benchmark release.
Comment: A few commenters support our proposal due to the government savings and greater
payment equity between MA EGWP and MA non-EGWP plans.
Response: We appreciate the support.
Comment: One Medicare Advantage Organization in support of the proposal explained that the
current approach to filing EGWP bids is cumbersome for both health plans and CMS. Plans often
submit many bids accounting for different structural characteristics but without specified benefit
level differences. Since benefits are not being decided during the bid process, beyond the
technical requirements under the current compensation system, the purpose of this additional bid
development work is not clear.
Response: We appreciate the support.
Comment: Many commenters requested that CMS delay implementation, or to consider a phase-
in approach by setting the bid-to-benchmark ratios at a higher level than calculated then stepping
them down over time at incremental target ratios. One commenter also suggested that CMS use

30
distributions or ratios from the 2016 bid year to publish rates in the 2017 Final Rate
Announcement.
Response: We appreciate the flexibilities these commenters suggested be incorporated into the
methodology. In order to address these requests, under the methodology we are finalizing as
described above, we are releasing 2017 final non-RPPO EGWP county payment rates with this
Rate Announcement and we will provide for a two-year transition to the new payment approach
for EGWPs.
Comment: A large number of commenters maintained that CMS does not have the legal
authority to make this payment change given that the purpose of employer group waivers, under
the statute, is to enhance and promote the offering of these types of retiree plans. These
commenters indicated in large part that Section 1857(i) does not give the Secretary the authority
to offer a new payment methodology for EGWPs. Instead the authority given to the Secretary is
to “facilitate” EGWPs by waiving or modifying requirements that “hinder” EGWPs.
Commenters believe that the statutory waiver authority does not provide CMS with the authority
to modify the core statutory payment terms in a manner that hinders EGWPs, by characterizing
the change as a condition for waiving of other program requirements.
Many comments asserted that the CMS proposal does not seem to be waiving or modifying a
methodology that hinders EGWPs. These commenters believe, instead, that it is the methodology
being proposed by CMS that will hinder EGWPs by creating an obstacle to offering EGWPs, by
increasing premiums and reducing benefits, which these commenters believe is contrary to
Congress’s intent in establishing CMS’s waiver authority. Many commenters further stated that
CMS acted in an arbitrary and capricious manner by not presenting data supporting its argument
that the waiver was authorized by statute.
Finally, several other commenters asserted that the proposed changes are inconsistent with the
regulations, asserting that CMS may not implement substantive changes to the MA bidding and
payment process through sub regulatory guidance that contradicts, but leaves intact, existing
regulations. These commenters believe that CMS must engage in rulemaking so that its
regulations accurately reflect the distinct payment methodology CMS is proposing for EGWPs.
Response: Medicare Advantage Organizations (MAOs) are required to submit to CMS a detailed
description of the benefits provided for each individual market plan they offer. MAOs are also
required to submit to CMS a bid for each of these plan benefit packages which includes detailed
pricing experience, assumptions and projections. MAOs negotiate with individual employers to
provide Medicare Advantage plans that exclusively enroll their retirees. To facilitate the offering
of such employer plans, CMS has waived the requirement for MAOs to submit plan benefit
package information and unique bids for each of the plans that they offer to employers. Under
this approach, MAOs may submit a single composite benefit package and bid for EGWPs and
are allowed to customize that benefit package and bid pricing for each of the various

31
arrangements they negotiate with employers. Associated with the waiver of having a financial
bid for each benefit package, CMS has also waived requirements related to the uniformity of
premiums and provided waivers that permit negotiation and customization of benefit packages
throughout the year rather than being limited by specific benefit packages that have been
submitted with bids; using this flexibility, MAOs offering EGWPs (and employers that directly
offer an EGWP) can - throughout the year – vary benefits from the composite bid that is
currently submitted in order to offer enhanced or customized supplemental benefits.
This approach has reduced the administrative burden for MAO sponsors of EGWPs, but also
means that CMS does not know how many EGWP plans any MAO offers, what specific benefits
are provided in each of those plans, or the associated underlying costs. This lack of transparency
has significantly impaired CMS’ ability to comprehensively review and assess the
reasonableness of the underlying actuarial assumptions and projections included in the bids
submitted for EGWPs and to trace how federal funds, in the form of the capitation payments and
the rebates, are spent for beneficiaries in specific EGWPs. This lack of transparency, combined
with the fact that EGWPs do not compete in the open market, has resulted in EGWP bids that are
systematically higher than bids for individual market MA plans. MedPAC has calculated that in
2012 margins were substantially higher for EGWPs (7.2%) than for other plans (4.4%). See,
e.g., MedPac, March 2015 Report to Congress;
http://www.medpac.gov/documents/reports/chapter-13-the-medicare-advantage-program-status-
report-(march-2015-report).pdf.
Given the lack of competition and transparency associated with EGWP bidding, we do not
believe that the current policy of allowing MAOs to submit composite bids and benefit packages
is sustainable. Instead of maintaining the current policy, we considered whether to revert to the
statutory and regulatory requirement of requiring EGWP sponsors to submit to CMS for review
and approval individual benefit packages and bids for each of their employer plans. However,
we concluded that the administrative burden for MAOs and employers of such an approach, in
addition to the significant challenges for CMS associated with expanding our review process to
accommodate thousands of additional benefit packages and bids, would substantially hinder the
offering of these plans.
3
As part of developing and submitting a financial bid for each plan
benefit package, the MAO would have to commit to specific plan benefit packages at the time of
the bid; the flexibility to modify benefits and customize plan offerings for employers would be
limited compared to the flexibility provided under the composite bid waiver; changes after bid
submission or mid-year would be more difficult. Using the statutory and regulatory bid
3
This consideration of how requirements on CMS may contribute to hindering the offering of
EGWPs is consistent with our past approach to exercising the authority under section 1853(i).
71 FR 22082 (“Specifically, because we do not receive and review these benefits we cannot
appropriately oversee their provision and requiring submission of these benefits needs to be
waived because we believe it would hinder the design of, offering, or enrollment in employer
sponsored coverage.”).

32
requirements would hinder the offering and design of MA plans by employers (either when
offered under a contract with an MAO or offered directly). We, therefore, concluded that our
proposed policy was the best framework for facilitating the offering of EGWPs and ensuring
appropriate payments to such plans.
Section 1853(b) requires that CMS use the Advance Notice and Rate Announcement process for
changes in Part C and D payment methodology; this proposal relates to the Part C payment
methodology for EGWPs. Section 1853(b) requires us to provide advance notice of the proposed
changes and to explain in the final Rate Announcement the assumptions and changes in
methodology for payments to MA plans. We have complied with those requirements in
proposing and finalizing this change in the methodology and assumptions for establishing the
capitation rates (and rebate payments) for EGWPs. Moreover, not all waivers issued under
section 1857(i) are in the MA regulations.
4
Indeed, when CMS implemented the EGWP waiver
for Part D bidding to reduce administrative burden, CMS notified Part D sponsors of that waiver
via an HPMS memo, stating in relevant part, “CMS believes that waiving the requirement to
submit 2008 Part D bids will facilitate the offering of plans for employers and unions seeking to
retain high quality coverage for their Medicare eligible retirees by avoiding the cost and
administrative burden of submitting these bids.“
5
The MA bid requirements are extensive and
require significant documentation from actuaries, more so than is required in Part D bids; further,
other flexibilities are associated with and flow from a waiver of the bidding requirements for
EGWPs. CMS therefore believes that waiving the bidding requirements for Part C plans will
have the similar effect of facilitating more offerings of these plan types in light of the significant
amount of time and effort it would take to compile data and project all of the assumptions CMS
requires throughout the bid submission and approval process for each plan benefit package.
Further, CMS has authority under sections 1857(i) and 1860D-22(b) of the Social Security Act to
waive or modify requirements that hinder the design of, the offering of, or the enrollment in
employment-based Medicare plans offered by employers and unions to their members. In this
regard, CMS is confident that we are in full compliance with the statutory authority in both
waiving the bid requirements and modifying the payment methodology to facilitate the offering
of MA plans by employers or under contracts between employers and MAOs.
Comment: Several individual beneficiaries detailed personal experiences with their MA EGWPs,
expressing concern for the potential losses of coverage and higher expenses that may result from
this proposal.
4
See, e.g., Medicare Managed Care Manual Chapter 9 – Employer/Union Sponsored Group
Health Plans; and https://www.cms.gov/Medicare/Prescription-Drug-
Coverage/PrescriptionDrugCovContra/Downloads/EGWP-Waivers.pdf.
5
February 28, 2007 HPMS Memo, 2008 Employer Group Waiver Policy – Elimination of the
Requirement for Entities Offering EGWPs to Submit Part D Bids.

33
Response: We appreciate these commenter’s concerns and while each plan and beneficiary
experience is distinct, we recognize that it is possible that some employers may choose to
provide less supplemental coverage to retirees as a result of this policy change. However, this
policy change will, for the first time, make transparent the amounts paid by CMS to insurers for
beneficiaries enrolled in EGWPs. Employers, as a result, may be able to use this information to
negotiate arrangements with insurers that retain, or perhaps even enhance, the value of the
EGWP for their retirees.
Comment: A large portion of commenters asserted that the proposal presents significant
operational challenges, especially with respect to timing. Under the proposal, payment rates for
EGWPs would not be known until August, which they state is long after most negotiations
between employers and EGWP sponsors must be concluded and too late for retirees to select
plans. Several commenters indicated that contracts are already negotiated and planned for 2017.
Some commenters indicated that they must determine final rates no later than June in order to
develop and print open enrollment materials that are required to reach beneficiaries which will
hinder or make impractical the ability of group sponsors to meet their obligations for
communicating with their retirees and seriously compromise the ability of retirees to make
informed decisions about their coverage. Moreover, commenters indicated, many EGWP group
sponsors have obligations from different regulatory bodies and oversight boards that require
prospective notice to their retirees before changes can be effective. Commenters expressed that
MAOs may be in the situation of being unable to adjust either the benefits provided or premium
charged to avoid significant financial losses caused by such a swiftly implemented and
significant change. Each of these commenters urged CMS to consider alternative timelines from
the proposed to prevent disruption of EGWP sponsors and beneficiaries with confusion and
concern for members who have counted on and made decisions premised on being able to keep
their health plans, claiming that these timing considerations alone would ultimately deter public
and private employers’ ability from providing EGWP coverage to their workforce.
Response: CMS appreciates the timing concerns raised by commenters and we are finalizing the
proposal with modifications to address these concerns. In the Advance Notice, we proposed to
calculate the bid-to-benchmark ratios for 2017 using non-EGWP bids and benchmarks for 2017.
Under this proposed approach, CMS would have released EGWP rates in the August timeframe
after completion of the 2017 bid review process. To address the timing concerns described
above, however, we have calculated bid-to-benchmarks ratios for 2017 using 2016 bids and
benchmarks and the resulting non-RPPO EGWP rates for each county are included at:
https://www.cms.gov/Medicare/Health-Plans/MedicareAdvtgSpecRateStats/Ratebooks-and-
Supporting-Data.html. The final RPPO EGWP rates will continue to be published in late
summer when the final MA regional standardized A/B benchmarks reflecting the average bid
component and the statutory component, i.e., the Regional Benchmarks, are published which is
in keeping with the existing time line for all non-EGWP RPPOs. While the 2016 data are not as
current as the data we proposed to use, we believe this revised approach appropriately prioritizes

34
the need to provide employers and insurers with information on payment rates in the Rate
Announcement. Moreover, the bid-to-benchmark ratios have not fluctuated significantly over
the past several years.
Comment: Several commenters expressed concern about the impact of the proposed payment
changes on retiree benefits, such as EGWPs no longer being able to pay the Part B premium on
behalf of enrollees and EGWPs potentially not being able to offer the supplemental benefits such
as dental, vision and enhanced (non-Part D) drug benefits. Other commenters believe that the
payment changes outweigh any administrative benefit as complex actuarial models will still need
to be maintained to set group renewals and quotes, limiting any administrative benefit.
Response: While we appreciate the concerns raised by these commenters, we believe that there is
sufficient funding under the methodology being finalized to sustain the offering of these benefits.
Moreover, while some actuarial models may still need to be developed for internal plan
purposes, the burden of meeting the June bid submission deadline will no longer need to be part
of the consideration in the development of these models for these plan types, which we believe
does lift the significant administrative burden. By contrast, the alternate proposal CMS
considered that would have required MAOs to submit to CMS individual benefit packages and
bids for each of their employer plans would have made meeting the June deadline an onerous
prospect for MAOs offering EGWPs as well as created significant challenges for CMS
associated with expanding our review process to accommodate thousands of additional benefit
packages and bids, which would substantially hinder the offering of these plans. Further, as
discussed above, by waiving the requirement to submit a financial bid for each plan benefit
package, CMS is facilitating flexibility in the offering and design of EGWPs. MAOs will not be
tied to specific EGWP plan benefit packages submitted as part of the MA bidding process and
may customize benefit offerings throughout the year. We appreciate the concerns raised,
however, and will continue to explore options for future policy development.
Comment: A few commenters suggested CMS permit EGWPs to separately reimburse members
for their Part B premiums.
Response: The Social Security Administration (SSA) must be able to accurately track beneficiary
payments of the Part B premium. Under current payment rules, if an MAO chooses to buy down
their beneficiaries’ Part B premiums, a fixed, standard amount for each beneficiary in their plan
is determined through the bid process. This standard amount is then deducted for each of their
beneficiaries from the monthly plan payments made from CMS to the MAO, which is then
transmitted from CMS to SSA on a beneficiary level. There is no mechanism to permit the
administration or collection of information directly from MA EGWPs to SSA to capture a
payment of the Part B premium for their beneficiaries. As a result, this is not currently a feasible
solution. We appreciate the concerns raised, however, and will continue to explore options for
future implementation. It should be noted however, that very few (approximately 2%) MA
EGWPs currently use rebate dollars to buy down any portion of the Part B premium for their

35
enrollees, so this is not expected to have a significant impact on beneficiaries enrolled in these
plans. In addition, while an MAO may not buy down the Part B premium for MA EGWPs, they
are not prohibited from offering other benefits or lower enrollee premiums in place of the Part B
premium buydown. The elimination of the option to buy down the Part B premium for MA
EGWPs does not affect the MA payments made to the MAOs.
Comment: A few commenters asserted that it seems to be unfair to lower reimbursement for
these plans following a significant Medicare Part B premium increase in 2016 that
disproportionately affected public employees who do not receive Social Security benefits, and
further stated that the significant portion of their Part B-only individuals would not be eligible
for individual MA plans unless they enrolled and paid the full Medicare Part A monthly
premiums.
Response: We appreciate the concern raised by these commenters. We recognize that it is
possible that some public employers may choose to provide less supplemental coverage to
retirees as a result of this modification of payment methodology and policy. However, this
policy change will, for the first time, make transparent the amounts paid by CMS to insurers for
beneficiaries enrolled in EGWPs, which is currently not transparent to Employers given that
MAOs submit highly aggregated bids which serve only as the starting point for their offerings to
differing employers’ with whom they contract under these offerings. Employers, as a result, may
be able to use this information to negotiate arrangements with insurers that retain, or perhaps
even enhance, the value of the EGWP for their retirees.
Comment: Many commenters stated their concern that the proposal will cause most insurers to
abandon the employer group MA market, reduce coverage and/or increase premiums, which will
lead to less choice for retirees and their former employers and discourage innovative plan design
in these markets. Because this policy would disincentivize these plans, these commenters said,
employers are likely to drop the EGWP coverage, and the burden shifts back to the government,
with an increase of members on traditional Medicare. Several State and municipal organizations
also noted that they may be forced to discontinue their retiree coverage or absorb price increases
that would cause state and local budget difficulties.
Response: We appreciate the concerns but believe that there is sufficient funding under the
methodology being finalized to sustain the offering of MA basic and supplemental benefits. We
also believe that employers may be in a better position to negotiate under this methodology,
because payment amounts would be standardized and known across competing plans. CMS does,
however, recognize that, to the extent that CMS’ payments to EGWPs are reduced and MAO
margins remain the same, employers may pay higher premiums for current levels of
supplemental coverage or may choose to reduce the supplemental coverage provided to
employees under these plans.
Comment: Several commenters stated that CMS should keep the annual bidding process and not

36
proceed with the proposed payment methodology in 2017 as the bidding process takes into
account claim experience, geographic location, and product coverage, but the proposal ignores
the differences between employer and non-employer plans. Moreover, several commenters
expressed concerns that this proposal would result in EGWP payments that are actuarially
unsound. Many MAOs that submitted comments also stated that they build their EGWP bids
based on true EGWP experience, so the bid amount requested has always reflected EGWP
claims and therefore revenue requirements. To remove the EGWP bidding process and revert to
a socialized bid would reduce the ability to maintain group MA business; further, the
administrative savings from not bidding on group MA business versus individual business is not
significant, especially for local players that sell EGWP policies primarily to small businesses.
Response: While we appreciate the perspective offered in these comments, CMS continues to
believe that due to the nature of the unique agreements MA EGWPs enter into, EGWPs do not
compete against other plans through the bidding process, and therefore have little incentive to
submit lower MA bids to CMS under the current bidding rules. On the contrary, as noted in the
Advance Notice, MedPAC has noted that the nature of the MA bid process and the ability to
access federal funds creates incentives for these plans to bid as close to the benchmark as
possible, in order to compete for employer business by lowering the costs imposed on employers.
Under this new policy, MAOs offering EGWPs will now need to compete for employers to
contract with them for these offerings on access, quality, customer service, and wrap-around
benefits. Implementing this proposal will also result in savings to the Government. Further, as
noted above, waiving the bidding requirement entirely and modifying the payment methodology
for these plans helps ensure continued flexibility in plan design and the timing under which
EGWP plan designs are finalized. We anticipate that these flexibilities and the increased amount
of information available to employers will facilitate the offering of these plans in the future.
Comment: A few commenters stated that for MA EGWPs to attract employers, plans are
frequently designed in ways that may lead to higher bids relative to the individual MA market.
For example, MA EGWPs frequently cover larger geographic areas in order to accommodate
large employers with retirees living in different parts of the country. Preferred Provider
Organization (PPO) networks are much more commonly found in MA EGWPs than in the
individual MA market as these benefit designs are both popular and valued in the employer
market. Both broad networks and a larger geographic distribution of beneficiaries can lead to
higher costs in coverage. Moreover, these plans offer coverage to beneficiaries in areas that are
underserved by individual MA plans through extended service area options allowed under MA
EGWPs waivers currently in place. The service area waivers allow for EGWPs to offer coverage
in areas where a plan may not have a full network. However, they add to the cost of the product
because, if enrollees use out-of-network providers with no contractual relationship with the plan,
there is less opportunity to effectively engage in care coordination.
Response: We appreciate the concerns but, as noted above, believe that there is sufficient
funding under the methodology being finalized to sustain the offering of these benefits. We also

37
believe that employers may be in a better position to negotiate under this methodology that
waives the bidding requirements for EGWPs, because payment amounts would be standardized
and known across competing plans. By removing the bidding requirements, MAOs will now
need to compete for contracts with employers on access, quality, customer service, and wrap-
around benefits.
Comment: A few commenters stated that while they recognize that there may be some problems
with the current bid structure, they remain concerned that CMS has not fully analyzed the impact
of this policy proposal or given full consideration of the rationale for higher bids from MA
EGWPs. These commenters requested CMS to provide additional information on any current or
ongoing analysis that has been conducted and encourages CMS to more widely solicit public
comments on this policy proposal and analysis.
Response: We thank these commenters for their considered thoughts on this issue. However, we
and MedPAC have monitored and analyzed this issue over the past several years and continue to
observe consistently higher bids from EGWPs without explanation. In the 2012 Advance
Notice, published on February 18, 2011, CMS raised these concerns publically, and specifically
requested comment on the causes for the data relationships we and MedPAC were observing.
We also stated in the 2012 Rate Announcement that we would be reviewing comments received
for future policy development. We would reiterate, however, that the bidding approach that has
been in effect through 2016 has hindered CMS’s ability to analyze this issue fully in light of the
fact that this bidding structure has not permitted CMS to know how many EGWP plans any
MAO offers, what benefits are provided in each of those plans, or the associated underlying
costs. This lack of transparency has significantly impaired CMS’ ability to comprehensively
review and assess the reasonableness of the underlying actuarial assumptions and projections
included in the bids submitted for EGWPs and to trace how federal funds, in the form of the
capitation payments and the rebates, are spent for beneficiaries in specific EGWPs.
Moreover, since the publication of the Advance Notice, CMS has provided the public with the
estimated financial impact of the proposal via an HPMS memo released on March 7, 2016,
which we are mitigating by implementing the policy with a transition. We appreciate the
concerns raised, however, and will continue to analyze options for future policy development.
Comment: One commenter stated their belief that Medicare Supplement plans (Medigap) will
benefit the most from this change, and well-managed Medicare Advantage plans will lose most
of their EGWP membership.
Response: We appreciate the concerns but believe that there is sufficient funding under the
methodology being finalized to sustain the offering of these MA plans.
Comment: A few commenters indicated that their particular areas of the country will be
significantly more impacted than others given the benchmarks and bid-to-benchmark ratios that
are anticipated to be applied to their payment rates, as well as the concentration of large group

38
employers and labor unions that offer retiree coverage in particular areas.
Response: The current bidding and payment methodology has disparate impacts on varying
geographic areas today. By calculating the bid-to-benchmarks at a quartile level, then applying
them to each county’s rate, and taking into account double bonus counties and star ratings, we
are accounting for a significant level of geographic variation in the payments in the methodology
being finalized. In addition, under the approach being implemented for 2017, we have
moderated the impact of the new policy by blending individual market plan and EGWP bids to
calculate the bid-to-benchmark ratios.
Comment: Several commenters stated their belief that CMS’s logic behind the proposal is flawed
as the MA EGWP population's risk scores are less relevant to their costs than this proposal
presumes, and instead it is more important to understand that in most cases, the benefits offered
under these plans have been carefully negotiated as an integral part of the accrued retirement
package for labor union and other large group employer workers. In some cases negotiated
collective bargaining agreements require single employers to continue providing health care
coverage to retirees. In addition, many are associated with Voluntary Employees’ Beneficiary
Associations (VEBAs) that provide health care benefits to retirees. In most cases these VEBAs
were established and are maintained in accordance with the terms of class action or bankruptcy
settlement agreements that were approved by federal district and/or bankruptcy courts.
Response: While we recognize that in certain circumstances the overall benefit package provided
to retirees under an EGWP is the result of a collective bargaining or class action/bankruptcy
agreement, the supplemental benefits provided under such an arrangement do not explain the
higher bids that we have consistently observed from EGWPs. Buying down cost-sharing under
Original Medicare is a supplemental benefit. Under the Medicare Advantage bidding process, all
plans (both EGWPs and non EGWPs) submit a bid for providing the benefits covered under
original Medicare. Despite bidding on the same package of basic benefits, on average, EGWP
bids for A/B benefits have consistently been significantly higher than those submitted by non-
EGWPs.
Comment: A few commenters also asserted that in the commercial market it is often true that
administrative costs for employer-based products are less than individual products due to
economies of scale. However, this is not the case for EGWP plans, especially in particular states,
since CMS announced two years ago that they consider enhanced Part D EGWP benefits to be
commercial coverage. As a result, certain state regulators consider EGWPs to be state-regulated
products and have added a layer of regulation that has made them significantly more complex to
administer than their individual counterparts.
Response: We appreciate these comments. We believe that they are in keeping with CMS’s
belief that waiving the requirement to submit 2017 Part C bids will facilitate the offering of Part
C plans for employers and unions seeking to establish high quality coverage for their Medicare

39
eligible retirees by avoiding the cost and administrative burden of submitting complex bids to the
federal government, particularly in light of these commenters’ concerns about increased state
oversight for those plans that offer both Medicare Advantage and Part D coverage.
Comment: Several commenters noted that EGWP bids tend to be higher than non-EGWP bids
because EGWPs are predominately PPOs, rather than HMOs. They argue that when making an
apples-to-apples comparison of EGWPs and non-EGWPs by plan type, the disparity in the bid-
to-benchmark ratio shrinks significantly. These commenters argue that CMS’s proposal will
arbitrarily lower benchmarks for PPO products and will drive out PPO EGWPs from the
marketplace. These commenters argue that the need to offer a broad network may be accounting
for the rate difference, rather than the CMS assertion that the payments are subsidizing wrap-
around coverage. According to the commenters, the current EGWP payment structure enables
plans to recognize the impact of these various product characteristics and the impact of different
cost structures between MA EGWP plans and individual market MA plans in their bids. The
proposed change does not allow plans to reflect these differences in cost structures in MA
EGWP specific bids and it shifts the MA EGWP funding to be based on individual plan costs
(largely HMOs) despite the fact that MA EGWPs are largely PPO plans. Several of these
commenters stated that if CMS should decide to proceed with the proposal that the bid to
benchmark calculations be modified to account for the different ratio of HMO to PPO plans in
EGWPs vs Non-EGWPs and to exclude D-SNPs from the calculations as they are not
representative of the type of coverage an employer purchases, and are therefore irrelevant to the
calculation.
Response: CMS recognizes that there are a larger number of MA EGWPs that are offered as
PPO plans instead of HMO plans than in the individual MA market, where the inverse is true. In
finalizing this policy, CMS considered whether such an adjustment would be appropriate to
account for this differential in plan offerings between the two markets. However, in the course
of reviewing the data, we determined that basing the MA EGWP payment rates on the small
number of PPO plans in the individual MA market could introduce significant year-over-year
instability in future EGWP payment rates.
Comment: One commenter indicated that retirees enrolled in MA EGWPs have a higher average
age as compared to individual MA plans. This age difference may be a result of a greater
propensity for EGWP plan retirees to stay in their same EGWP MA plan until death, since group
retiree health insurance is generally supported by employer/union contributions toward the
premium, which provides an incentive for retirees to maintain continuous coverage under the
group plan, and “end of life” medical expenses in EGWP plans are higher than in individual
plans.
Response: We appreciate that this commenter’s concerns, however, the CMS-HCC risk
adjustment model takes the age and health status of beneficiaries into account. Therefore, we
would expect that if this were the case, risk scores for MA EGWPs would be higher on average

40
than those in the individual MA market. However, as we noted in the Advance Notice, CMS and
MedPAC have analyzed the data and concluded that the inverse is true.
Comment: Many commenters noted that the proposal is complicated, the two week comment
period did not provide plans sufficient time to fully understand its application and
implementation, and CMS has not released enough information for stakeholders to fully evaluate
the methodology and its financial impact. Moreover, several commenters suggested that while
the Advance Notice is well-anticipated by companies in the health insurance industry, employers
(including many state governments) and unions may not be aware of the publication or anticipate
that it will have a significant impact on their finances or employee and retiree benefits.
Response: We appreciate that the comment period may be limited, however, section 1853(b)
requires CMS to release and post the Rate Announcement on the first Monday in April and
release the Advance Notice describing the proposals at least 45 days in advance. Similar
proposals have been proposed for the past several years in the President’s Budget, and MedPAC
has made similar recommendations. So while we recognize that this policy was proposed for
Part C implementation for the first time in the 2017 Advance Notice, the concepts behind the
methodology being finalized have been proposed previously by the Administration. Moreover,
in the 2012 Advance Notice, published on February 18, 2011, CMS raised these concerns
publically, and specifically requested comment on the causes for the data relationships we and
MedPAC were observing. We also stated in the 2012 Rate Announcement that we would be
reviewing comments received for future policy development.
Comment: Commenters suggested that CMS needs to study the root cause of the differences in
MA versus EGWP payment to identify the actual adjustments to policy that are required to
increase payment equity.
Response: In the course of developing this policy, CMS considered requiring MA EGWPs to
provide CMS with detailed information on the PBP provided to each employer group and class
of retirees within that plan benefit package in order to delve deeper into the root causes of the
differential bidding patterns. However, CMS concluded that it would impractical to require the
submission and collection of data necessary to expand our review process to accommodate the
large number of PBPs which could exceed 25,000 to 50,000 benefit packages depending on the
number of unique plan variations MAOs offer to employers. It should be noted, that these figures
are only a rough estimate, as under the bidding waivers in place through 2016 for MA EGWPs,
CMS does not have sufficient data from submitted bids to know how many various benefit
packages are currently being offered to employers by MAOs. Moreover, since retiree health
benefits would be expected to vary among individual beneficiaries within a single Medicare plan
on the basis of differing underlying union agreements or employment contracts, such data would
likely need to be collected at the beneficiary level, rather than at the plan level. The burden of
such expanded data collection and submission and review was determined to be unduly
excessive for both plan sponsors and CMS.

41
Comment: A few commenters detailed several distinctions between MA EGWPs and MA non-
EGWPs such as improved patient outcomes due to better coordination of care programs, the
ability to better coordinate between vendors providing more comprehensive case management
for their beneficiaries, flexible pricing and plan design, consistency in coverage during the
transition from employment coverage to retirement coverage and improved customer service.
Other commenters indicated that MA EGWPs and MA non-EGWPs are distinct as EGWPs serve
a separate purpose, i.e., providing a vehicle to provide comprehensive medical coverage,
integrating fee-for-service Medicare benefits with employer or union-funded supplemental
employee/retiree benefits. Unlike individual-market MA plans, employer-plan sponsors select a
limited number of EGWP options from which retirees can choose to enroll.
Response: We thank commenters for these observations and acknowledge that there are
distinctions between EGWP and non-EGWP plans. However, we do not believe our proposal
will inhibit the ability of employers and insurers to take advantage of these distinctions. Nor do
we believe that these distinctions explain the higher bids that we have observed from EGWPs.
Comment: Many commenters argued that this proposal is too blunt to administer fairly and that
the bidding process takes into account claim experience, geographic location, and product
coverage fluctuations that cannot be accounted for with an administratively-set payment amount.
A few other commenters noted that that MA EGWP bids serve an important administrative
function as they enable CMS to correctly administer Part D and the retiree drug subsidy. The
MA EGWP bids allow CMS to verify that groups receive at least actuarially equivalent benefits
to what the MA plan offers its individual members. Commenters stated that the process helps
ensure that any rebates from the bid savings are used to reduce premiums or enrich benefits.
These commenters also encourage CMS to further discuss how CMS will oversee group
premiums and benefit offerings if group bids are eliminated and there are no longer the group bid
margin proximity rules. Without group bids, there may be uncertainty as to how MA plans will
be regulated by CMS for their group business.
Response: We thank these commenters for their considered thoughts on this issue. We appreciate
the concerns raised, and will continue to explore options for future policy development. We
would also note that this policy is only waiving the MA EGWP bidding (BPT) requirements and
detailing their alternative payment methodology. MA EGWPs will continue to submit the plan
benefit package (PBP) and formulary in accordance with the rules for 2017.
Comment: A few commenters requested that we clarify whether the bid-to-benchmark ratios will
be calculated on an individual bid basis for a particular county or will be tied to the weighted
average bid-to-benchmark results for individual bids submitted nationally, whether the
benchmarks that will be used will have the qualifying county adjustments included, and whether
SNPs are part of the individual bid-to-benchmark ratio calculation. Others inquired as to why
CMS doesn’t collect employer group membership in the individual bids to better calculate an

42
organization’s employer group ISAR and employer group risk scores to make the calculation of
employer group payments based on individual bids more accurate and actuarially sound.
Response: As described in the Advance Notice and finalized as described herein, the bid-to-
benchmark ratios are a weighted average at the quartile level which will result in four
percentages – one for each quartile. The percentages are then applied to the county ratebook to
each of the published 5%, 3.5%, and 0% county ratebook rates, which include adjustments for
bonus counties. SNPs are included in the calculations to determine the bid-to-benchmark ratios.
In developing the policy, CMS considered collecting a limited dataset from MA EGWPs such as
projected risk scores based on the plan’s service area; however, collecting even this limited data
was determined to be contrary to the goal of reducing administrative burden on offering these
plans, as some level of detail in support of the projections would need to be submitted to and
evaluated by CMS to verify it’s actuarial accuracy.
Comment: One commenter stated that they do not feel it is appropriate to apply the risk score to
the county rebate amount as that is different than how the payment is made for individual plans.
Response: Under current bidding rules, rebate dollars resulting from an A/B bid below the
benchmark are risk adjusted within the bid to determine the per-member-per month rebate
amount CMS will pay to the MAO. CMS believes that both the A/B portion of the payment and
the rebate portion of the payment should continue to be risk adjusted and, given the lack of bid
submissions, we are therefore incorporating that step into the payment process in the
methodology being finalized.
Comment: A few commenters indicated confusion regarding how this new methodology would
interact with prior bid instructions related to margin requirements and consistency between
underwriting assumptions and the bid. They requested clarification as to whether these
requirements and others requirements previously included in the bid instructions would still be in
place under this new methodology.
Response: Given that EGWPs will no longer submit bids to CMS, the bid review requirements
related to margins will no longer be applicable to EGWPs. The instructions for the MA Bid
Pricing Tools will be updated accordingly.
Comment: One commenter requested clarification regarding how the methodology will adjust
individual bid-to-benchmark ratios for the Extended Service Area Waiver approved for EGWP
plans, will the ISARs used to develop the individual bid-to-benchmark ratios be normalized to a
1.0 risk score, and how members in ESRD, Hospice, and MSP status would be treated under the
proposed methodology.
Response: Under the finalized payment methodology, the MA EGWP payment will be based on
the beneficiary’s county code. CMS will calculate a bid-to-benchmark ratio for counties in each
FFS quartile and the applicable bid-to-benchmark ratio for each county will be used to calculate

43
a standard EGWP payment for that county. The ISAR-adjusted bid and benchmarks are both
standardized numbers in the bid pricing tool, so they are already at a 1.0 risk score. We are not
applying a normalization adjustment in the bid-to-benchmark calculation. As a result, the
payment for all EGWPs with the same quality Star Rating in a county will be the same,
regardless of other counties the EGWP might include in its total service area. Plans will
continue to be paid using the ESRD ratebook for their ESRD beneficiaries. MSP status is a
payment adjustment to the risk score so the risk score applied to the county payment rate will
reflect the MSP adjustment factor if applicable. Under current payment rules, beneficiaries in
MA plans that elect Hospice currently only receive a rebate payment from CMS. If the rebate is
$0.00 then these plans do not receive a payment. As discussed in the Advance Notice, specific
rebate amounts will no longer be identifiable under the payment methodology being
implemented, therefore, beginning in 2017, all MA EGWPs will receive $0.00 payment for each
of their members that elect Hospice. We appreciate the concerns raised, however, and will
continue to explore options for future policy development.
Comment: One commenter requested clarification surrounding the plan benefit package
submission requirements for MA EGWPs, and further asked if these plans will need to upload a
formulary that represents the “leanest” option that they would make available to EGWP plans.
Response: This methodology is only waiving the MA EGWP bidding (BPT) requirements and
detailing their alternative payment methodology. Therefore, MA EGWPs will continue to submit
the plan benefit package and formulary in accordance with the rules for 2017.
Comment: A few commenters suggested that the MA EGWP proposal represents a step
backwards from the movement towards value based payment and improved models of care. They
indicated that employers would drop EGWP coverage in favor of Medicare “wraparound”
products, thereby increasing costs to the government, and retirees would lose access to care
coordination programs that would possibly reverse gains in health status and outcomes.
Commenters stated that this proposal could cause regression of the quality improvements made
through the Star ratings program.
Response: We thank commenters for these observations, however, we do not believe our
proposal will inhibit the ability of employers and insurers to take advantage of alternative
payment models. In fact, we believe that employers may be in a better position to negotiate
payment arrangements under this methodology to waive the bidding requirements for EGWPs,
because payment amounts would be standardized and known across competing plans. By
removing the bidding requirements, MAOs will now need to compete for employer contracts
primarily on access, quality, customer service, and wrap-around benefits.
Comment: A few commenters expressed concerns about the impact on beneficiaries in Puerto
Rico should this policy be finalized, stating that the economic situation in Puerto Rico and the
government debt crisis preclude any further investment in these types of retirement plans, which

44
have significant actuarial deficits. For example, teachers in Puerto Rico decided a long time ago
not to participate in the Social Security Program and their retirement fund is in a major crisis.
Having their EGWP MA Plan provides beneficiaries with some relief. However, additional
contributions to these MA EGWP retirement plans is not possible in the current economic times.
Response: We appreciate the concerns expressed by these commenters, but believe that the
impact on Puerto Rico is minimal and that there is sufficient funding under the methodology
being finalized to maintain the offering of sustainable benefits in Puerto Rico.
Comment: A significant majority of commenters requested that CMS reconsider and withdraw
the proposal entirely.
Response: While we understand the concerns raised, we have explained throughout this section
why we are finalizing the proposal with modifications. The waivers of bidding requirements and
the modified payment methodology being finalized will eliminate potential burdens and
hindrances on offering EGWPs associated with the MA requirement that each plan benefit
package be associated with a financial bid while simultaneously resulting in savings to the
Government by providing a more equitable payment methodology for MA EGWPs. Further, we
note that CMS has previously waived bidding requirements for Part D for EGWPs and set
payment amounts for Part D plans based on the competitive bids submitted for non-EGWP Part
D plans; here CMS is finalizing a similar waiver and payment policy for EGWP Part C plans
beginning with 2017.
Section G. CMS-HCC Risk Adjustment Model for CY 2017
Comment: Many commenters strongly support CMS’ proposal to update the CMS-HCC model
by separating the community model segment into six subgroups based on dual eligibility status.
Many commenters support implementation of the new model without delay to improve and
stabilize the payment structure for full-benefit dual eligible beneficiaries. A few commenters
noted that the proposed changes would improve the sustainability of D-SNPs and MMPs and
create a more equitable risk-adjustment system. One commenter thanked CMS for not including
a clinical revision of the hierarchical condition categories (HCCs) as part of the model revision
and supports CMS’ proposal to use the same disease interactions across the 6-segment
community model with the addition of the disease interaction for the disabled segment, as this
promotes consistency across the segments.
Response: CMS appreciates the support.
Comment: Many commenters urged CMS not to implement the proposed model in 2017, or
requested a phase in of the new model. These commenters are concerned that the proposed
model changes will reduce overall revenue to the MA program through a net MA funding
reduction of 0.6% and introduce disruptions to benefit designs. One commenter noted that
coefficients for certain HCCs decrease under the proposed 2017 model compared to the 2014

45
model. Another commenter raised concerns that the changes CMS proposes to the partial-benefit
dual eligible model could have the unintended consequences of reducing enrollment in Medicare
Savings Programs (MSPs). A few commenters suggested implementing the new model in Puerto
Rico alone as a pilot.
Response: CMS is proceeding with the implementation of the new model, which will pay more
accurately for beneficiaries, regardless of their dual status, and reduce incentives for plans to
avoid enrolling full benefit dual beneficiaries. Overall, the net impact on plan payments will
vary based on the composition of plans’ enrolled populations and disease profiles of
beneficiaries within those populations.
Comment: A number of commenters expressed concern that the impact on MA payment of the
revised model was greater than the -0.6% that CMS estimated and will lead to instability in the
MA program. Several commenters requested more information regarding how CMS calculated
the model impact. These commenters stated that the effects of the proposed model, combined
with the Part C normalization factor, will result in additional and possibly unintended material
differences on payment risk scores for CY 2017.
Response: We acknowledge the commenters’ concerns and note that there was a technical error
in the calculation of the model denominator used to create the model relative factors. This error
resulted in model relative factors (and, therefore, the raw risk scores) that are 1.8% too low. This
error directly affected the historical risk scores used in determining the normalization factor,
which, as a result, was also too low.
Although the corrected model factors are 1.8% higher, our calculation of the industry level
model impact is the same. To determine the industry level model impact, we compared the
current model (2014 CMS-HCC model) to the revised CMS-HCC model. In order to isolate the
model revision impact, we developed updated denominators for the two models based on the
same year. The model denominators that were developed for the purpose of model impacts both
had the same error, resulting in the same comparison once the error was fixed on both sides. We
do note that the risk scores produced under the new model posted on HPMS should have been
1.8% higher.
Comment: A few commenters appreciated the transparency and early information regarding the
proposed model in the Request for Comment in October 2015, but requested additional
information, including details of how the changed model will operate, raw risk scores under the
2014 and proposed 2017 models, and analyses on impacts that outline how the negative 0.6%
national impact was calculated. Some commenters also suggested that CMS allow plans the
opportunity to study the proposal and the revised risk scores under the new model beyond the
time period allowed for comment following release of the Advance Notice. A few commenters
recommended additional analyses of the model before implementation while a few commenters
urged CMS to monitor the results of the model changes. One commenter recommended that an

46
independent analysis be conducted by an external research organization to analyze the accuracy
of the implemented risk adjustment model and to provide recommendations on areas for
improvement, followed by a stakeholder process and at least a 60-day comment period.
Response: CMS has made efforts to release more information and at earlier times, than the
statutory deadlines require, by, for example, releasing research findings four months prior to the
publication of the Advance Notice through a Request for Comments, sharing plan-level risk
scores (calculated under both the current and the proposed model) a month before the publication
of the Notice; and CMS’ plan to share operational details earlier than usual. We will continue to
engage with stakeholders as we implement the model.
Comment: CMS received comments in support of maintaining the PACE CMS-HCC Risk
Adjustment Model. One commenter recommended that CMS evaluate the impact of updating the
PACE model by applying distinct risk factors for full, partial, and non-dual eligible enrollees;
and also consider recalibrating the PACE model, which is currently calibrated with 2006/2007
data.
Response: CMS appreciates the support. We did not propose to make changes to the risk
adjustment model that we use for PACE organizations and will continue to use the existing
model for 2017. This model is described in the 2011 Advance Notice and Rate Announcement.
We will consider these comments for future years.
Comment: A few commenters recommended providing transitional relief to plans receiving
negative payment adjustments. For example, one plan recommended that CMS implement a
one-time retroactive adjustment to plans serving high proportions of dual beneficiaries to
compensate for prior underpayments based on duals served.
Response: CMS is continually working to improve our method for risk adjusting payments and
can legally only make changes to future years.
Comment: Many commenters expressed concern that CMS is only focusing on dual eligible
beneficiaries and that the new model will hurt plans with low enrollment of full-dual eligible
beneficiaries. These commenters made suggestions about how CMS could make revisions to the
risk adjustment model to improve the prediction of costs for full duals, while maintaining the
current risk score level for non-duals. They stated that a “one-size fits all” approach does not
work and that CMS should instead create proposals to address the needs of specific populations
and geographic regions rather than broadly applying a policy to the entire Medicare program. A
few commenters recommended that CMS implement the model only for dual-SNPs while
retaining the current model for non-SNPs and institutional plans. One commenter stated that
CMS should make an upward adjustment to the non-dual eligible categories to ensure that the
revised model does not unfairly penalize non-dual plans. Several commenters that commended
CMS for focusing on vulnerable populations believe this focus should not result in overall

47
funding reductions across the MA population. One commenter recommended that CMS revise
the model only to reflect the costs between full and partial dual eligible beneficiaries. The
commenter stated that CMS should refrain from adjusting the currently successful model for
non-dual eligible beneficiaries. One commenter noted that the model change is not revenue
neutral and that it is not clear if CMS has the authority to make model changes that are not
revenue neutral to the MA population. A few commenters recommended that CMS institute a
"hold harmless" that allows plans to receive the largest of their risk score calculated under the
2014 and 2017 models or alternatively institute a budget neutrality adjustment to assure that the
overall payment for the MA population is not decreased.
Response: CMS believes that the 2017 model improves payment accuracy and results in more
payment equity across plans. After extensive research, CMS has demonstrated that the current
model underpredicts for full benefit duals, while overpredicting for both partial benefit duals and
for non-duals. Further, it is evident that diagnoses are inadequate to fully predict the costs; in
other words, beneficiaries with similar clinical profiles have different costs, and these costs
differences are related to beneficiaries’ dual status. Whether dual status is predictive of costs
because it is a proxy for income level or because the status is indicative of price sensitivity, or a
combination of both, is an open question. It is clear that dual status, as a supplemental predictor
to diagnoses, is predictive of cost.
Regardless of how we better predict costs for any population of beneficiaries, CMS would need
to redenominate the model to retain an average 1.0 risk score. When we redenominate the
model, all the relative factors will change in relationship to the 1.0 average risk score. For
example, simply increasing the Medicaid factors in the model, in order to better predict
aggregate costs for full benefit duals, would have the effect of decreasing the risk scores for non-
duals, relative to average. CMS sets this 1.0 risk score for the FFS population since Medicare
Advantage payment rates are statutorily tied to FFS. In setting the 1.0 for the risk scores we use
for payment, we mirror our approach of setting the average FFS risk score to 1.0 in the ratebook
in order to be consistent with the rates. Therefore, we did not propose and are not making any
changes to the model in order to retain the average MA risk score at the same level that it was
under the current model. The change in the aggregate MA risk score is almost entirely due to the
different distribution of duals compared to that in FFS (a small portion of the impact is due to
updating the underlying data in the model by three years). Given that we believe that this
revision improves the predictive ability of the model, we believe that it is appropriate to allow
MA risk scores to change in response to the revised model. Finally, section 1853 does not
require that risk adjustment be revenue neutral for MA plans.
Comment: Some commenters stated that revising the model will increase instability in the MA
program. A few commenters highlighted their concern that the 2017 revision to the CMS-HCC
model follows a series of recent major changes, including the clinical revision of the CMS-HCC
model in 2014, introduction of encounter data as a source of risk scores, and conversion from

48
ICD-9 to ICD-10, to the model and risk adjustment methodology in the previous few years. One
commenter recommended that CMS implement annual bounds to changes in the factors to
prohibit overly significant changes in any one year and possible errors in predictive rates.
Another commenter suggested that CMS refrain from making changes to the risk adjustment
model more often than every two years.
Response: We appreciate commenters’ concerns about stability and the impact of multiple
changes happening in plan payment in the last few years. We note that the model that we
implemented in 2014 was phased in over three years, and that we haven’t changed the HCCs
with the revisions to the model for 2017. Similarly, the implementation of ICD-10 has been
planned for many years. There has been strong interest expressed, and CMS agrees, to
continually look for ways to improve the predictive accuracy of the risk adjustment model. We
believe, that if we identify a way to make an improvement to the model, we should do so.
Comment: Several commenters questioned CMS’ decision to use FFS data to estimate the risk
model changes in MA. One commenter stated that the proposed changes in the 2017 Advance
Notice ignore the lack of any measure of quality or care management in the FFS spending data
used as the basis for the risk adjustment model. Several commenters also recommended that
CMS use MA data instead of FFS data for model calibration.
Response: CMS recognizes that FFS utilization and costs may not represent the experience in
Medicare Advantage plans and our goal is to eventually calibrate the CMS-HCC risk adjustment
model on MA data. We note that the aggregate dollars that a plan sponsor needs, in order to
provide Parts A and B benefits to their enrolled beneficiaries, is determined in the plan bid. The
purpose of the model is not to establish the total amount paid to the plan, but the relative
expected costs of the beneficiaries enrolled in the plan. To the extent that the relative costs of
diseases in the model differ for an MA plan from FFS, then the model may not perfectly predict
that plan’s costs. This will always be the case for any specific plan, since the model predicts
expected relative costs, on average, across a population. Because we have used FFS data to
calibrate our risk adjustment models since we first instituted risk adjusted payments to plans, we
believe that it is a suitable alternative for determining the relative costs until we have sufficient
experience using complete encounter data to develop the risk adjustment model.
Comment: Numerous commenters supported the inclusion of the Psychiatric HCC x Substance
Abuse HCC disease interaction for the disabled segments of the community model.
Response: CMS appreciates the support.
Comment: A few commenters who support the proposed changes to the model expressed
concerns about the omission of chronic conditions, such as CKD stages 1, 2, and 3 and diabetic
neuropathy, as well as mental health conditions, including dementia, and mental health and
substance abuse interaction terms from the model. Some commenters believe that CMS should

49
focus more on chronic conditions. One commenter noted that if CMS is concerned about MAOs
coding dementia at greater levels in an effort to serve enrollees, the agency should review the
data to determine whether or not such coding is appropriate. Another commenter noted that the
revised model inappropriately cuts payments for chronic conditions regardless of dual status.
Response: CMS decides whether to include a condition category in the model after balancing
several considerations, including each category’s ability to predict costs for Medicare Parts A
and B benefits, whether the diagnostic classifications measure disease burden, and whether
diagnosis codes that are subject to discretionary or inappropriate coding should be excluded.
CMS understands the clinical significance of the conditions recommended for inclusion in the
model by commenters, including the importance of appropriately managing patients to slow the
progression of kidney disease and that the treatment of dementia can be costly. Further, we
understand that including these conditions in the model would potentially increase the risk scores
of beneficiaries who have been diagnosed with them. Our concern regarding dementia and
chronic kidney diseases focuses on the diagnosis and coding of these conditions relative to FFS
and, in the case of dementia, the broad clinical definitions that have been developed in order to
identify the disease. While we fully support these efforts to identify and treat dementia, we are
concerned that the broad clinical definition may result in dementia being coded at greater levels
in MA relative to FFS, resulting in overstatement of the risk of such beneficiaries and leading to
inaccurate payment. Such concerns do not revolve around whether the coding is accurate, but
rather whether it is different than in FFS. Although not all conditions are included in the CMS-
HCC model, the model still predicts beneficiaries’ expected costs for all A and B benefits,
including costs associated with chronic and mental health conditions. Given the goal of managed
care organizations, we expect plans will appropriately manage chronic conditions and mental
health conditions for their beneficiaries, irrespective of model refinements.
Comment: A commenter requested clarification on whether or not the initial reason for
Medicare entitlement will carry with a beneficiary for the duration of his/her time in the
program, or whether every beneficiary over the age of 65 – regardless of disability status – will
be classified as aged for purposes of the model segment.
Response: CMS is not changing how we handle the determination of aged versus disabled or the
use of original reason for entitlement in the calculation of risk scores. For risk adjustment, all
beneficiaries aged 65 and over are considered aged; if an aged beneficiary was originally entitled
due to disability, they are treated as aged and originally disabled. We continue to use originally
disabled factors for beneficiaries who are aged and were originally eligible for Medicare due to
disability. These factors, like the other factors in the model, are additive. Non-aged beneficiaries
will be classified as disabled for the purposes of determining interaction terms (if applicable)
and, for beneficiaries in the community, which model segment to use for risk score calculation.
Comment: Some commenters recommended that CMS examine factors, other than dual status,
which may further improve the model to help predict costs more accurately. These factors

50
include social determinants of health, functional status, lower risk deciles, and beneficiaries with
high health costs.
Response: Medicaid data is a readily available and comprehensive data source that provides
information about a status that serves well as a predictor of Medicare costs. While CMS has
found that Medicaid status improves the ability of the model to predict costs, we welcome
suggestions from stakeholders regarding other potential predictors of Medicare expenditures that
are easily accessible and available to be used in both calibrating the risk adjustment model and
calculating risk scores for all Medicare beneficiaries.
Comment: One commenter stated CMS ignores the fact that cost differences between full-
benefit and partial-benefit duals reflect different utilization incentives for the two populations
rather than true differences in clinical health care needs and costs. A few commenters encourage
CMS to study QMBs independently to understand if adding them as an additional category of
enrollees would further improve the accuracy of the model.
A few commenters questioned whether there exists sufficient consistency across states to ensure
parity in the risk score model calculation. One commenter asked CMS to consider whether the
definitions of the dual status categories, which are often decided at the state level, are consistent
with how CMS proposed to stratify beneficiaries in developing the model. Another commenter
stated that if the model is going to be implemented, CMS should either include dual code 01 as
full dual or incorporate an adjustment factor by state (or groups of similarly situated states) to
reflect the variation in the predictive ratios from state to state caused by the varying state
eligibility requirements for QMB Plus and SLMB Plus status. A few commenters suggested the
need for strong oversight and quality assurance work with state based Medicaid data. One
commenter proposed enhancements to the current reporting systems requiring all states to report
a minimum set of data upon which a status determination can be made or alternatively, CMS
should consider a system similar to that already in use in the Extra Help program in Medicare
Part D. Another commenter urged CMS to consider adjusting the proposed individual condition
and demographic coefficients so that all dual coefficients (full/partial & aged/disabled) are equal
to, or higher than their non-dual counterparts.
Response: We recognize that there are state-by-state differences in eligibility criteria that will
result in different classifications for some beneficiaries who might be determined to be a partial
benefit dual in some states and a full benefit dual in other states. However, as noted elsewhere in
this Announcement, CMS believes that using Medicaid data, in general and to differentiate dual
eligible subgroups (i.e., full benefit or partial benefit dual status) improves the accuracy of the
model and better predicts costs for key subgroups of beneficiaries. Further, CMS does not have
other data that would inform CMS about different income levels of Medicaid eligible
beneficiaries, so we are unable to explore whether subsetting the Medicare population in other
ways based on income would improve payment accuracy. Without the ability to test whether

51
other subsetting arrangements would improve the model, we also have insufficient information
for assessing whether differing State Medicaid eligibility criteria are a reasonable basis for state-
specific adjustments. As we reported in the October 2015 HPMS memo and in the 2017
Advance Notice, our analyses showed that the current CMS-HCC model overpredicts for partial
benefit dual beneficiaries by 7.2% (disabled) and 12.3% (aged). Further, MedPAC has reported a
similar finding, which indicates that CMS has been overpaying for partial dual beneficiaries. We
also note that the model underpredicts for full benefit duals by approximately 5% (disabled) and
11% (aged). The differences between how well the current model predicts for full and partial
benefit duals are sizable, and CMS believes that improving the prediction of the model is
imperative.
We note that partial benefit dual risk scores are notably higher than non-dual risk scores. As we
shared in the 2017 Advance Notice, our analyses show that the cost and disease patterns of the
non-dual, full benefit dual, and partial benefit dual, and the aged versus disabled segments were
distinct, both within the dual types (e.g., full benefit dual aged versus full benefit dual disabled)
and between the dual types (e.g., full benefit dual disabled versus partial benefit dual
disabled). Furthermore, the differences in cost patterns among these subgroups varied
significantly both overall and by HCC disease category. In other words, predicting costs
separately for each of these dual subgroups, even when using the same diagnoses, produced
unique sets of coefficients. For example, the partial benefit duals are not just less expensive than
full benefit duals (and more expensive that non-duals), but they have different clinical profiles
and cost patterns. In the case of some conditions, the coefficients for partial benefit duals are
higher than those for full benefit duals, reflecting the different clinical profiles.
Comment: One commenter requested that CMS establish a demonstration for C-SNPs, where
they would be provided waivers to existing payment methods and regulatory policy.
Response: Thank you for your comment.
Comment: Many commenters stated that the new model is complicated and introduces
significant operational and administrative challenges for both CMS and plans. One commenter
stated that plans will have much more difficultly using six models to predict future risk scores
and prepare accurate bids, which may create unnecessary volatility in benefit designs, member
premiums, and cost sharing as forecasting CMS payments becomes far more complex. A few
commenters were specifically concerned about dual eligibility determination and asked CMS to
take into account the challenges involved with obtaining accurate and timely monthly data from
states on dual status. These commenters asked CMS to consider developing a process for
applying retroactive changes, if necessary. One commenter recommends that CMS clearly track
payment adjustments and allow for the possibility that payment adjustments resulting from
Medicaid retroactive status and delays in state reporting could occur after the final risk scores are
run.

52
Response: We appreciate the challenges facing plans in order to implement this new model.
CMS is in the process of developing technical specifications for how we would implement the
proposed model and plan to release information regarding the operational implementation after
the CY 2017 Rate Announcement has been published.
Comment: A few commenters indicated the need for a special adjustment to account for non-dual
beneficiaries in Puerto Rico who would otherwise be considered partial benefit duals in a non-
Territory state. Commenters suggested that the two components of this adjustment would be: 1)
an estimate of the proportion of partial duals within the non-dual group in PR, which can be
based off of the Puerto Rico Community Survey data or the proportion of partial duals estimated
using the 10 states with the highest poverty levels, and 2) applying a factor to the non-dual
population in Puerto Rico to account for the partial dual risk.
Response: CMS is not making this adjustment. If CMS were to make an adjustment to the risk
scores of non-duals in Puerto Rico, to account for what the risk scores of some beneficiaries
would be if Puerto Rico had implemented the QMB and SLMB eligibility categories, we would
need to make an adjustment to both the risk scores used in payment and the risk scores used to
standardize the ratebook. Since adjusting the risk scores in the ratebook would make the rates
lower, CMS has determined that an adjustment for non-dual beneficiaries in Puerto Rico would
not improve payments for Puerto Rico.
Comment: A number of commenters are concerned by the large drop in revenue for the
Institutional segment of the model. Plans are requesting more information to explain why the
recalibration of data (updates to the risk adjustment relative factors and coefficients) are having
such a significant negative effect on plan payments. A few commenters recommended that CMS
postpone or not implement the implementation of the revised model for the LTI segment until
further analyses are conducted.
Response: As noted in the Advance Notice, in addition to the model revision to improve the
predictive power of the model for dual eligibles, the entire CMS-HCC model, including the long
term institution (LTI) segment, was recalibrated with more recent data years. We acknowledge
commenters’ concerns and have investigated the drivers of the decrease in the risk scores for the
Institutional segment of the model. We observed that the actual average cost for beneficiaries in
LTI status decreased by 8.6% when we compared 2010-2011 data against 2013-2014 data.
Because the overall costs of beneficiaries in the community has increased slightly, the relative
costs of LTI beneficiaries, relative to the average Medicare beneficiary, have also
decreased. Specifically, the data year update accounts for the change in LTI risk scores, not the
model revision, and given the changes in the actual LTI costs, the decrease in LTI risk scores
would have occurred even if we only had recalibrated the existing model. Our research indicates
that the decrease in LTI risk scores is mostly driven by decreased expenditures for SNFs, home
health organizations, and DMEs in 2014 compared to 2011. Furthermore, we found that

53
utilization rates for ER visits, hospital stays, and SNF stays for this population were lower in
2014 than in 2011.
Comment: A few commenters encouraged CMS to review new enrollee scores utilizing the six
community segments and develop separate rates for members in these membership groups. One
commenter was concerned about the accuracy of the current “default” risk scores and the effect
that imposing the new risk adjustment model will have on already inaccurate default risk scores.
This commenter recommended that CMS should use current year data, supplemented with prior
year data, to establish risk scores for members that age into Medicare to more accurately reflect
member risk in the first year of Medicare eligibility or alternatively, increase the assumed
morbidity in the age/gender risk score weights to more accurately reflect plan liability for these
members.
Response: New enrollee risk scores are scores that CMS uses when a beneficiary does not have
adequate diagnoses to calculate a full risk score (operationalized as having fewer than 12 months
of Part B in the data collection year). Because prior year data is insufficient to predict risk in the
payment year for these beneficiaries, CMS uses a combination of age-sex, Medicaid, and
originally disabled factors to determine the risk score of a new enrollee. The new enrollee model
is calibrated to individually predict for each age-sex/Medicaid/originally disabled combination,
and the beneficiaries in the model sample are limited to those with less than 12 months of Part B
in the data collection year so that predicted costs are reflective of the new enrollee population.
Medicaid status has always been assessed in the payment year for new enrollees. CMS did
analyze the effect of using separate factors for full benefit duals and partial benefit duals and has
determined that predictive ability of the new enrollee risk scores does not improve with separate
factors for partial and full dual benefit beneficiaries. Therefore, CMS is not making any changes
to the new enrollee segment of the model.
Section H. Medicare Advantage Coding Pattern Adjustment
Comment: Many commenters were pleased that CMS is not going above the statutory minimum.
Response: CMS appreciates the support of the commenters.
Comment: We received several comments regarding the coding intensity adjustment level.
Several commenters felt that the coding intensity adjustment should be lower. A few of these
commenters expressed concerns that the cumulative impact of coding adjustment and other
changes in 2017 may present a risk to the ongoing viability of some MA plans. In contrast, a few
commenters requested that the adjustment be higher than the statutory minimum, expressing
concern that CMS may not be fully adjusting for the differing coding trends.
Additionally, a few commenters indicated that coding patterns in MA are heterogeneous and that
applying an across the board adjustment is inequitable. One commenter suggested that CMS
should apply a coding adjuster to plans that code poorly instead of those that code well. Another

54
commenter proposed a segmented approach such that a low coding factor is applied to lower
coding plans while a larger factor is applied to high coding plans.
Response: CMS determines the MA coding pattern adjustment using the model to be used in the
payment year so that the impact on trends in coding differences of any model change are taken
into account. While CMS understands the commenters’ concerns, we have extensively analyzed
the MA data and determined that the optimal way to apply the adjustment is to do so uniformly
and industry wide using the statutory minimum adjustment level.
Comment: One commenter suggested that the coding adjustment factor be reduced or eliminated
for C-SNPs. The commenter stated that SNPs serve beneficiaries who have specified chronic
conditions and are high risk, and they provide more high-touch care to their members so it is
impossible to compare C-SNP coding intensity to FFS, given the concentration of chronically ill
patients in these [MA] products. The commenter also believes that the flexibility afforded to
CMS under the CMMI demonstration authority gives CMS the ability to test the reduction or
elimination of the coding pattern adjustment for C-SNPs without modifying the adjustment
factor for any other plans (i.e., in a non-budget neutral way).
Response: MA coding adjustment is a methodological adjustment to risk scores to improve
payment accuracy given differential coding patterns in MA and FFS. CMS measures the
differences in coding patterns between MA and FFS by observing the year-over-year growth in
disease scores for beneficiaries who remain in MA or in FFS over time. Therefore, our MA
coding adjustment factor reflects differences in coding patterns over time, not levels of risk
scores.
Comment: A few commenters noted that CMS incorrectly implied that any observed coding
differentials between the FFS and MA populations are driven by inappropriate coding on the part
of MA plans and urged CMS to recognize that higher coding does not necessarily equate to
wrong coding. One commenter urged CMS to consider the interaction between the adjustment
for coding intensity and those that may result from RADV audits and ensure that MA plans and
providers are not over-penalized.
Response: As we have noted in previous Advance Notices and Rate Announcements, we are not
assuming that MA coding is inaccurate in calculating the MA coding pattern adjustment factor.
Rather, we are adjusting for the impact on risk scores of coding patterns that differ from FFS
coding, the basis of the CMS-HCC model and the Part C normalization factor. RADV audits, on
the other hand, have the purpose of validating that diagnosis codes submitted for risk adjustment
are documented in the medical record and, therefore, are correctly reported for the beneficiary in
question.
Comment: A few commenters thought that it was inappropriate to apply the coding pattern
adjustment to encounter data-based risk scores and that coding adjustment should apply only to
the RAPS-based portion of payment.

55
Response: CMS will continue to apply the MA coding difference factor to risk scores as long as
we calibrate our CMS-HCC model solely on FFS data. Per the statute, we will apply this
adjustment until we implement “risk adjustment using Medicare Advantage diagnostic, cost, and
use data,” meaning until we have recalibrated the model using MA encounter data. We also note
that because the encounter data system accepts diagnoses obtained through chart review, MAOs
will be able to submit the same diagnoses that they have been submitting into the RAPS. Given
that the encounter data system does not change the definition of acceptable diagnoses or limit
their submission, CMS anticipates that the risk scores calculated using encounter data will reflect
the same coding trend as those calculated with RAPS-based diagnoses. CMS will monitor the
impact of using encounter data-based diagnoses on risk scores and risk score trends.
Comment: A few commenters requested that CMS take the effect of ICD-10 on coding and
reduce the MA coding adjustment factor.
Response: We understand that the healthcare industry has been working with providers to
prepare for the transition to ICD-10 since the final rule was published on January 16, 2009 (45
CFR 162). In addition, we remind commenters that plans have until at least January 31st after the
payment year to submit accurate risk adjustment data (which includes both submissions to the
RAPS and the Encounter Data Processing System). Given the extended period providers and
plans have had to transition to ICD-10 and the extended period of time plans have to submit and
correct diagnosis codes, we do not believe an adjustment to the MA coding pattern adjustment
factor is warranted.
Comment: One commenter noted that any policy changes that would have a significant impact
on MA plan payment should be implemented only after being published in the Federal Register
and considered under notice and comment conducted under the APA and the PRA.
Response: Per statute, the MA coding adjustment is to be made as part of the risk adjustment
methodology established under section 1853(a)(3) of the Social Security Act. Section
1853(b)(2) provides that CMS “shall provide for notice to [MA] organizations of proposed
changes to be made in the methodology. . .used in previous [year] and shall provide [MA]
organizations an opportunity to comment on such proposed changes.” (Emphasis added.)
Section 1853(b)(1) in turn provides for a final notice in which the “risk and other factors to be
used in adjusting” payment will be published. When section 1853(a)(3) was first implemented in
2000 with the initial risk adjustment methodology developed by CMS, the initial methodology
was implemented through this section 1853(b) notice and comment process. All subsequent
changes to the risk adjustment methodology, have all been implemented through the section
1853(b) notice process. We believe that in specifying in section 1853(b) a detailed process for
providing MA organizations with “notice” and an “opportunity to comment” on “changes” in the
MA payment “methodology,” Congress was specifying that this process was to be used to
implement such changes, and that in its judgment this process gives MA organization a sufficient
opportunity for input on changes affecting their payments. This belief is buttressed by the fact

56
that Congress has on several occasions ratified in statute methodologies that CMS established
through this 1853(b) process (e.g., the initial phase in of risk adjustment and the plan to phase
out budget neutrality). Thus, we believe that the Advance Notice and Announcement process is
the appropriate vehicle for implementing and updating the MA coding adjustment factor.
Section I. Normalization Factors
Comment: Many commenters questioned the accuracy of the normalization factors and
subsequent impact provided by CMS in the 2017 Advance Notice.
Response: As mentioned in Section I, “CMS-HCC Risk Adjustment Model for CY 2017,” CMS
has discovered a technical error in the calculation of the denominator used to create relative
factors for the revised CMS-HCC model. While the proposed normalization calculation
methodology was applied correctly, the historical risk scores used to calculate the normalization
factor were incorrect; specifically, due to the technical error in the model relative values
discussed in Section G above, the risk scores were too low and resulted in a predicted payment
year risk score that was too low. Please see the table below for updated historical FFS risk
scores using the revised CMS-HCC model as well as the original scores from the 2014 CMS-
HCC model for comparison.
Table III-1. Historical Risk Scores under the 2014 and the 2017 CMS-HCC Models
Year
FFS Risk Scores
2014 CMS-HCC Model
FFS Risk Scores
2017 CMS-HCC Model
2011
0.988
0.990
2012
0.997
0.998
2013
0.996
0.996
2014
0.999
1.000
2015
1.002
1.001
Comment: Some commenters asked that CMS change the methodology used to calculate the
normalization factors. Commenters expressed concern that the quadratic functional form was
not the best method for predicting future risk scores either because the influence of the aging
baby boomer population on the trend has failed to materialize as expected or because there is not
enough data to accurately predict future risk scores. Commenters suggested several alternatives
for projecting normalization, including changes in methodology, such as a return to a linear
function or a logistic growth function, or including additional years when applying a quadratic
function.
Response: In response to comments, CMS has decided to increase the number of years included
in the historical data used to calculate the normalization factor from four to five. CMS
understands that baby boomers aging into Medicare is resulting in FFS risk scores increasing at a
slower, less predictable, rate. The addition of an extra data point will better capture the variation

57
in FFS risk scores over time and further CMS’ objective of better predicting the average FFS risk
score for Payment Year 2017. We are not changing our methodology and will continue to use a
quadratic equation to estimate a trend in risk scores and calculate the normalization factor for the
payment year.
As some commenters observed, the normalization factors have been increasing over the past two
years at a greater rate than might otherwise be expected. The increases in the normalization
factors are the result of adding more recent years’ risk scores to the historical data used to
calculate each year’s normalization factor. In 2013, FFS risk scores decreased. Since 2013, FFS
risk scores have been increasing (although at a slower rate than before 2013). In other words,
when we projected the Payment Year 2015 risk score using historical data ending in 2013, the
projection reflected a downward trend that later turned out to be incorrect (i.e., the PY2015
normalization factor was too low). Similarly, the PY2016 normalization factor, although
reflecting an upward movement in the historical data when we added the 2014 risk score, was
also too low, although by less than the PY2015 normalization factor. The normalization factor
for PY 2017 would have increased further if we had not increased the number of years included
in the regression model in response to comment. These trends in risk scores and normalization
factors can be seen in the graph of 2014 CMS-HCC model FFS risk scores below. The PY2017
normalization factor shown is the factor we would have used had we not implemented a revised
CMS-HCC model or increased the number of historical years used when calculating
normalization factor for PY2017.
0.990
0.978
0.997
0.992
1.007
1.014
1.026
0.920
0.940
0.960
0.980
1.000
1.020
1.040
1.060
1.080
1.100
2010 2011 2012 2013 2014 2015 2016 2017
2014 CMS-HCC Model FFS Projections by Payment Year
PY2015 v22 Quadratic Trend
PY2016 v22 Quadratic Trend
PY2017 v22 Quadratic Trend
Normalization Factors
*Black markers indicate actual risk score values
Comment: Many commenters requested that CMS provide a detailed explanation of the FFS
normalization factor calculation for 2017.

58
Response: When CMS updates a risk adjustment model, dollar coefficients from the
model are divided by average per capita FFS expenditure in the denominator year to
create relative factors. Once a model is implemented, the average risk score in FFS is 1.0
in the denominator year. The revised CMS-HCC model has a 2015 denominator. If risk
scores are calculated for any year other than the denominator year, those risk scores will
not be 1.0. In order to keep the average FFS risk score 1.0 in the payment year, CMS
calculates what we call a normalization factor that projects a FFS risk score trend to the
payment year using historical FFS risk score data (see table above). Each payment
model has a normalization factor that is updated in each payment year. A normalization
factor for one year cannot be used with risk scores from another year or another model.
For the last several years, CMS has been using a quadratic function to predict future FFS
normalization values. This function has the form:
The intercept and parameter estimates are derived from an ordinary least squares (OLS)
regression where FFS risk scores are regressed against year and year squared for five years of
data.
Comment: Some commenters stated that the current methodology is not appropriate for the
ESRD model. Several commenters also expressed concern about the significant impact of the
Part D normalization factor. Both factors increase from 2016 to 2017. For Part D, commenters
were concerned that the change in normalization factors would increase beneficiary premiums.
Response: For the Part D and ESRD models, CMS observes a similar pattern of under
normalization in PY2015 as with the CMS-HCC model and, therefore, a larger than expected
increase in normalization factors for PY2016 and PY2017, as more recent data leads to more
accurate predictions in these years. As with the Part C normalization factor, and also in response
to comments that we add an additional data year to more accurately explain variation in observed
risk scores, CMS has decided to add an additional year of data to the calculation of the
normalization factors in PY2017 for the ESRD Dialysis, Part D, and PACE/ESRD Functioning
Graft payment models. Below are the updated normalization factors, along with the historical
data used to calculate them.

59
Table III-2. PY2017 Normalization factors
Year
Revised
CMS-HCC
model
PACE/ESRD
Functioning Graft
CMS-HCC model
ESRD CMS-
HCC Model
RxHCC
model
2010
0.987
2011
0.990
1.031
0.956
0.996
2012
0.998
1.042
0.972
1.002
2013
0.996
1.043
0.974
0.995
2014
1.000
1.048
0.981
1.000
2015
1.001
1.052
0.989
PY 2017
Normalization factor
0.998
1.051
0.994
0.976
*Please note that the Part C normalization factors use 2011-2015 data, while the RxHCC
normalization factor uses 2010 – 2014 data.
Section J. Frailty Adjustment for PACE organizations and FIDE SNPs
Comment: Most commenters supported maintaining the current PACE frailty factors as well as
the use of updated frailty factors to determine frailty scores for FIDE-SNPs.
Response: CMS appreciates the support.
Comment: A few commenters requested that the requirements for eligibility to receive frailty
adjustments be expanded to include other plan types, such as I-SNPs and C-SNPs. Several
commenters suggested that frailty factors should be applied to all frail beneficiaries, not just
those beneficiaries enrolled in PACE plans or qualifying FIDE SNPs.
Response: Under the statute, CMS must use the same payment methodology for all MA plans,
including Special Needs Plans (SNPs), except in specific cases. Section 1853(a)(1)(B)(iv)
permits CMS to make frailty-adjusted payments only to certain dual SNPs – those with fully
integrated, capitated contracts with States for Medicaid benefits, including long term care, and
which have similar average levels of frailty as the PACE program. Thus, CMS cannot make
frailty payments to any SNP that does not meet the statutory criteria without implementing frailty
payments program-wide. If CMS were to apply a frailty adjustment to all MA plans, we would
do so in a manner that does not increase aggregate MA payment. Specifically, the frailty model
is calibrated to result in an average frailty score of 0.0. Thus, some enrollees would have a
negative adjustment. Please reference the 2008 Advance Notice, published February 16, 2007,
for more discussion on this topic. We also note that CMS has previously explored ways of
capturing frailty by all MA plans and found challenges with a number of approaches (see the
“Evaluation of the CMS-HCC Risk Adjustment Model,” 18 published March 2011, at

60
https://www.cms.gov/Medicare/Health-Plans/MedicareAdvtgSpecRateStats/Downloads/
Evaluation_Risk_Adj_Model_2011.pdf for more information).
Comment: One commenter recommended that CMS base its frailty scores for comparison to
PACE on the proportion of FIDE SNP members meeting PACE level of care requirements as
assessed through State-approved assessment mechanisms used for nursing home and community
based waiver level of care determinations.
Response: CMS calculates frailty scores using data obtained in a similar manner to the data used
to calibrate the frailty model. CMS’ frailty model is calibrated and frailty scores are calculated
using data obtained from commonly-fielded surveys (the Consumer Assessment of Healthcare
Providers and Systems (CAHPS) survey of FFS beneficiaries and the Health Outcome Survey of
plan enrollees) to assess the average frailty of a plan or contract. Specifically, CMS uses
limitations on activities of daily living (ADLs) obtained from written surveys that are completed
by the beneficiary (please reference page 6 of the 2008 Advance Notice for a discussion of this
source of the ADL data used to calibrate the frailty model). If CMS were to use ADL data from
provider or plan sources, the frailty scores would be overstated. Further, because ADL data are
collected via survey, we only collect the data for a subset of a plan’s membership and it is,
therefore, not possible to pay frailty calculated at an individual level for all enrollees in a plan.
CMS believes the HOS and HOS-M survey currently provide the best estimate of a plan’s frailty
score because those surveys can be sampled at the PBP level and are standardized, unlike the
state level assessments, which can vary from one state to the next.
See Table III-3 for the 2017 payment factors for all qualifying FIDE SNPs.
Table III-3. FIDE SNP Frailty Factors for CY 2017
ADL
Non-Medicaid
Medicaid
0
−0.083
−0.093
1-2
0.124
0.105
3-4
0.248
0.243
5-6
0.248
0.420
Section K. Encounter Data as a Diagnosis Source for 2017
Comment: While a number of commenters support the continued incorporation of diagnoses
from encounter data into risk score calculations, many expressed concern that moving to a 50/50
blend of the RAPS/FFS and EDS/FFS risk scores is too aggressive at this time. There was a
variety of recommendations for the blend of risk scores that ranged from maintaining the
Payment Year 2016 blend of 90% of RAPS/FFS-based risk scores and 10% of encounter
data/FFS-based risks scores to a more gradual increase in the transition blend. Several
commenters suggested using a blend of 70% of the RAPS/FFS-based risk scores and 30% of the
encounter data/FFS-based risk scores. Some commenters felt that, since the final encounter data

61
filtering logic and the related MAO-004 reports were only recently released, they have not had
sufficient time to understand the impacts and how to operationalize the reports. In addition,
there was concern expressed regarding the ability to accurately reflect the filtering impacts in the
bid for Payment Year 2017, given that the impact of the blend for Payment Year 2016 will not be
known for a while. A few commenters were concerned with complications in submitting
encounters from capitated provider groups and the burden encounter data collection places on
capitated provider groups. Some commenters raised concerns about the completeness, stability,
and reliability of encounter data given problems with system edits. Some commenters thought
the timing of an increased blend would be problematic given the unknown impact of ICD-10 on
diagnosis reporting and risk scores. Finally, many commenters noted that CMS has not
evaluated impacts of encounter data on risk scores nor conducted statistical analysis to ensure
data accuracy and reliability.
Response: CMS appreciates the feedback and understands the challenges regarding the use of
encounter data for risk adjustment. As many of the commenters noted, CMS has been and
continues to work in good faith with submitters on technical and operational issues to address
encounter data acceptance, completeness, and quality. CMS is also working closely with health
plans to respond to their questions and make changes, where needed, to address the issues cited
with the MAO-004 reports.
CMS’s goal is to transition entirely from using diagnoses submitted to RAPS to using diagnoses
from encounter data and we intend to continue transitioning away from a reliance on RAPS data
for calculating risk scores. However, for 2017 payment, CMS will proceed with a blend
percentage for the encounter data/FFS-based risk score of 25%, as opposed to the 50% blend that
was proposed. Specifically, for Payment Year 2017, we will calculate a risk score using
diagnoses submitted to RAPS and FFS diagnoses, and another risk score using diagnoses filtered
from encounter data and FFS diagnoses. We will sum 75% of the RAPS/FFS-based risk score
with 25% of the encounter data/FFS-based risk score. The blended scores will have the same
normalization factor and the same MA coding adjustment.
The policies adopted through this Announcement apply to PY2017 (2016 dates of service),
which will have a submission deadline no earlier than January, 2018. We note that encounter
data submission rates have steadily increased while error rates have steadily decreased. CMS
expects this trend to continue to improve as more experience is gained and for the data to
stabilize by the time this blend would be in effect. CMS has also worked continuously with the
plan community to understand other submission and operational issues through industry and
individual plan level discussions, and will continue to do so. Given this, CMS plans to increase
the weighting of encounter data-based risk scores over the next couple of years by moving to a
risk score incorporating 50% of the encounter data/FFS-based risk score in 2018, a risk score
incorporating 75% of the encounter data/FFS-based risk score for 2019, and a risk score of 100%
encounter data/FFS-based risk score in 2020.

62
Comment: Some commenters supported the proposed 50/50 blend. Two commenters
encouraged a more aggressive approach by going to risk scores based on 100% encounter data,
stating that health plans have had sufficient time to acclimate to the EDS submission
requirements and that, since these data inherently requires a richer level of data submission than
RAPS, transition to this data source should result in greater overall payment accuracy. The
commenter also noted that maintaining two separate data submission processes was burdensome
to both health plans and CMS.
Response: CMS appreciates the support of the commenters.
Comment: A few commenters supported the proposal to continue the same method of
calculating risk scores as used for the 2016 payment year for PACE plans.
Response: CMS appreciates the support of the commenters and is finalizing this as proposed.

63
Attachment IV. Responses to Public Comments on Part D Payment Policy
Section A. Update of the RxHCC Model
Comment: Most commenters expressed support for CMS’s decision to not adjust the hepatitis C
coefficient downward, and encouraged CMS’s commitment to maintaining payment accuracy by
making adjustments as treatment patterns evolve.
Response: CMS appreciates the support.
Comment: Some commenters suggested CMS consider making the hepatitis C coefficient
"concurrent" in the RxHCC model going forward in order to more accurately capture costs.
Response: CMS’s objective in using a prospective model is to identify chronic, predictable
conditions, not acute events. Thus, the Part D risk adjustment model is not designed to predict
costs based on diseases that are primarily diagnosed, treated and cured in the same year. Making
a single factor concurrent would over-emphasize the cost attributed to that condition, and reduce
the costs attributed to the other, prospective factors.
Comment: Some commenters suggested that CMS should continue to review drug costs and
treatment patterns for other diseases and consider similar adjustments to other coefficients, so
long as changes are based on appropriate actuarial and related data analytics.
Response: CMS appreciates this recommendation and will take it into consideration.
Comment: One commenter requested that CMS consider doing an analysis on the accuracy of
the Medicare Part D RxHCC model for dual eligible and to share that analysis with states.
Response: CMS appreciates the request and will take it into consideration. However, the Part D
risk adjustment model is currently segmented by low income status. The risk scores from these
segments take into account the additional cost of low income beneficiaries.
Comment: Some commenters questioned whether CMS intended to leave blank the rows for
NonAged_RXHCC 164 and NonAged_RXHCC 165 in Table 5 in the institutional segment.
Response: Yes, CMS intended to leave blank rows for NonAged_RXHCC 164 and
NonAged_RXHCC 165 in Table 5 in the institutional segment. These interaction terms are
technically included in the calibration of the Part D model but the predicted amounts are either
negative or statistically no different from zero. To avoid confusion, we are removing these
interaction terms from the final table of RxHCC factors.
Section B. Encounter Data as a Diagnosis Source for 2017
See Section K for comments and responses related to this issue.

64
Section C. Part D Risk Sharing
Comment: We received two comments in support of the decision not to make any changes to the
Part D Risk sharing parameters and the analytical approach taken to reach this decision. One
commenter added that staying consistent in this manner will allow for more accurate bids.
Response: CMS appreciates the support.
Section D. Medicare Part D Benefit Parameters: Annual Adjustments for Defined
Standard Benefit, Low-Income Subsidy, and Retiree Drug Subsidy in 2017
Comment: A few commenters asked for CMS to change how the out-of-pocket threshold is
updated each year, asking specifically for a change in how the parameter is indexed to better
align with the growth in drug costs.
Response: Pursuant to section 1860D-2(b)(4)(i)(IV) of the Act, for each of years 2016 through
2019, the out-of-pocket threshold increase is the lesser of the annual percentage increase or the
July CPI plus two percentage points. CMS does not have the authority to modify the parameter
indexing methodology.
Comment: Several commenters expressed concern about the underlying drug cost trends driving
the annual Part D benefit parameter updates. One commenter stated that brand name prescription
drug price increases are continuing to accelerate while the effects of the “generic patent cliff” are
beginning to subside. The commenter added that it is noteworthy that the growth rate for the
Medicare Part D out-of-pocket cap is constrained through 2019 due to the Affordable Care Act.
The commenter stated that, although Part D enrollees are protected now, they will soon face the
full impact of benefit parameter changes that could increase their out-of-pocket liability by
hundreds of dollars per year. The commenter strongly urged CMS to monitor Medicare Part D
spending trends and their subsequent impact on enrollees.
Response: CMS appreciates the concerns of commenters and will continue monitoring Part D
spending trends and their impact on enrollees.
Comment: One commenter noted that it is crucial that Part D sponsors have flexibility to use
clinically-based tools and techniques to promote greater affordability in the program in response
to the threat provided by the influx of high-cost drugs into the Part D market.
Response: While we appreciate the concerns of commenters and will continue to work with the
industry to monitor Part D spending trends and manage their impact on enrollees, CMS must
update the parameters for the defined standard Part D prescription drug benefit and promote
affordability in a manner consistent with the statutorily prescribed methodology.
Comment: One commenter stated that, while Hepatitis C treatment costs present significant
costs for plans and should be captured in the risk adjustment model, they should not be permitted

65
to have a significant and pervasive impact on Part D benefit parameters. The commenter
requested CMS to consider alternative ways to derive benefit parameter increases, since the cost
increases for Hepatitis C patients only impacts the extreme right tail of the claim distribution and
have minimal bearing on the claim distribution pattern for approximately 99 percent of the
Part D population.
Response: CMS again appreciates the concerns of commenters, but is required by statute to
update the parameters for the defined standard Part D benefit by the annual percentage increase
in average expenditures for covered Part D drugs per eligible beneficiary.
Comment: One commenter noted that the maximum copay thresholds for each tier of drug for
individuals that qualify for the low-income subsidy have remained largely unchanged. The
commenter suggests that CMS develop an indexing system where the cost sharing is tied to the
cost of prescription drugs.
Response: While we appreciate the concerns of commenters and will continue monitoring Part D
spending trends and their impact on enrollees, CMS must update the parameters for the low-
income subsidy in a manner consistent with the statutorily prescribed methodology.
Section E. Part D Calendar Year Employer Group Waiver Plans
Comment: The majority of commenters expressed support for the proposal to pay CY EGWPs
prospective reinsurance, with several indicating that through this proposal CMS has provided
calendar year EGWPs with much needed cash flow relief from the effect of the rapid increases in
the cost of specialty drugs experienced by all prescription drug plans over the past few years.
Response: We appreciate the support.
Comment: A few commenters requested that the amount paid be more plan specific instead of
an average. While a few other commenters were uncertain as to whether the prospective payment
amount would be based on a plan specific average or on a national average.
Response: The $26.50 prospective payment is the national average paid to Calendar Year
EGWPs for payment year 2014. CMS considered incorporating a plan or contract specific
methodology in the course of developing the proposal, but ultimately decided against that
approach due to anticipated operational and administrative challenges for both CMS and plans.
Moreover, the intent of the policy is not to pay more or less than actual incurred reinsurance, but
to provide additional cash flow to these plans during the course of the benefit year until the
actual incurred reinsurance costs are ultimately reconciled, which may not take place for as long
as eleven months following the end of a calendar year.
Comment: A few commenters were unsure of the timing of the payments, the administration of
the prospective payments, and the impact of the prospective payments on the regular adjustment
process that occurs in normal plan year reconciliation, and requested clarifying details.

66
Response: Beginning in Calendar Year 2017, CMS will pay $26.50 per member per month in
prospective reinsurance to each Part D Calendar Year EGWP as part of the monthly prospective
payments currently made to these Contracts. Part D EGWPs will still be subject to
reconciliation. Incurred actual reinsurance reconciliation calculations will remain intact as they
exist today, except that the prospective reinsurance payments will be reconciled to actual
incurred reinsurance costs during the normal annual reconciliation process. In the event that the
prospective reinsurance payment amount for a plan for a year exceeds the actual incurred
reinsurance amount calculated during reconciliation for a plan for a year, the difference between
the prospective reinsurance payment and the actual incurred reinsurance amount calculated
during reconciliation will be recouped by CMS. In the event that the prospective reinsurance
payment amount for a plan for a year is less than the actual incurred reinsurance amount
calculated during reconciliation for a plan for a year, the difference between the prospective
reinsurance payment and the actual incurred reinsurance amount will be paid to the plan in
accordance with current reconciliation processes. The reinsurance reconciliation rules as
summarized above for CY Part D EGWPs will be applied the same way that the reinsurance
reconciliation rules currently apply to non-EGWP plans that submit reinsurance estimates in their
bid submissions, upon which they are paid prospectively, but which are ultimately reconciled to
actual incurred reinsurance costs during the normal reconciliation process.
Comment: Two commenters opposed the policy expressing that paying a prospective reinsurance
amount could cause confusion for the impacted plans and lead to an expectation of reduced
premiums while, in fact, their payments will ultimately be reconciled annually. The commenters
suggested that CMS either develop a prospective reinsurance payment for all CY EGWPs that is
not reconciled, or continue the current practice of reconciling reinsurance payments without
paying a prospective payment.
Response: Although CMS appreciates the commenters’ concerns, we believe that our detailed
responses to the comments we received on the policy sufficiently allay their concerns. Our
responses provide more explicit detail surrounding the payment flow details, giving particular
emphasis to the fact that the EGWP policy does not increase or decrease the amount any given
Part D EGWP will ultimately be paid for their actual incurred reinsurance for any given payment
year. The prospective amount paid in reinsurance will be reconciled to actual incurred
reconciliation costs during the normal annual reconciliation process.
Comment: One commenter requested that CMS reconsider using the 2014 proposed values as
metrics for prospective payments given significant drug pricing and payment differences that
will have occurred between 2014 and 2017. The commenter asserted that basing prospective
payments on 2014 will not accurately compare the current status of providing benefits in the
program and will lead to frequent and potentially costly adjustments for the 2017 plan year.
Response: The reconciliation data for 2014 contains the most recent actual total reinsurance
amount available for publication in the 2017 Advance Notice/Rate Announcement. CMS is

67
proposing this methodology as it is based on the most currently available actual Part D CY
EGWP experience. The 2015 reinsurance reconciliation amounts will not be known until
approximately November of 2016, which means CMS and plans will not know the amounts until
near the beginning of the benefit year, which we believe would lead to unnecessary confusion in
the payment process. In addition, given that these plans currently receive $0.00 in prospective
reinsurance, we believe that providing the average amount of $26.50 per member per month is a
reasonable and conservative amount to pay in order to accomplish our goal of providing
additional cash flow throughout the year to facilitate the sustainable offering of these plans,
while limiting the probability of needing to take back a large amount of prospective reinsurance
payments in the annual reconciliation process when the prospective payments are reconciled to
actual incurred reinsurance.
Comment: One commenter requested confirmation that the reinsurance amounts for plans
without additional coverage in the coverage gap will not be different than for plans with
additional coverage in the coverage gap.
Response: The reinsurance amounts will not be different for plans with and without additional
coverage in the coverage gap. The reinsurance reconciliation rules as summarized herein for CY
Part D EGWPs will be applied the same way that the reinsurance reconciliation rules currently
apply to non-EGWP plans that submit reinsurance estimates in their bid submissions, upon
which they are paid prospectively, but which are ultimately reconciled to actual incurred
reinsurance costs during the normal reconciliation process.

68
Attachment V. Final Updated Part D Benefit Parameters for Defined Standard Benefit,
Low-Income Subsidy, and Retiree Drug Subsidy
Table V-1. Updated Part D Benefit Parameters for Defined Standard
Benefit, Low-Income Subsidy, and Retiree Drug Subsidy
Annual Percentage Increases
Annual
percentage
trend for
2016
Prior
year
revisions
Annual
percentage
increase
for 2017
API: Applied to all parameters but (1) and (2)
6.99%
4.45%
11.75%
July CPI (all items, U.S. city average): Applied to (1)
1.13%
−1.26%
−0.15%
September CPI (all items, U.S. city average): Applied to (2)
1.67%
−1.46%
0.18%
Part D Benefit Parameters
2016
2017
Standard Benefit
Deductible
$360
$400
Initial Coverage Limit
$3,310
$3,700
Out-of-Pocket Threshold
$4,850
$4,950
Total Covered Part D Spending at Out-of-Pocket Threshold for Non-
Applicable Beneficiaries (3)
$7,062.50
$7,425.00
Estimated Total Covered Part D Spending for Applicable Beneficiaries (4)
$7,515.22
$8,071.16
Minimum Cost-Sharing in Catastrophic Coverage Portion of the Benefit
Generic/Preferred Multi-Source Drug
$2.95
$3.30
Other
$7.40
$8.25
Full Subsidy-Full Benefit Dual Eligible (FBDE) Individuals (6)
Deductible
$0.00
$0.00
Copayments for Institutionalized Beneficiaries (category code 3)
$0.00
$0.00
Copayments for Beneficiaries Receiving Home and Community-Based
Services (5) (category code 3)
$0.00
$0.00
Maximum Copayments for Non-Institutionalized Beneficiaries
Up to or at 100% FPL (category code 2)
Up to Out-of-Pocket Threshold (1)
Generic/Preferred Multi-Source Drug (6)
$1.20
$1.20
Other (6)
$3.60
$3.70
Above Out-of-Pocket Threshold
$0.00
$0.00
Over 100% FPL (category code 1)
Up to Out-of-Pocket Threshold
Generic/Preferred Multi-Source Drug
$2.95
$3.30
Other
$7.40
$8.25
Above Out-of-Pocket Threshold
$0.00
$0.00
Full Subsidy-Non-FBDE Individuals

69
2016
2017
Applied or eligible for QMB/SLMB/QI or SSI and income at or below
135% FPL and resources ≤ $8,780 (individuals) or ≤ $13,930 (couples)
(7) (category code 1)
Deductible
$0.00
$0.00
Maximum Copayments up to Out-of-Pocket Threshold
Generic/Preferred Multi-Source Drug
$2.95
$3.30
Other
$7.40
$8.25
Maximum Copayments above Out-of-Pocket Threshold
$0.00
$0.00
Partial Subsidy
Applied and income below 150% FPL and resources below $13,640
(individual) or $27,250 (couples) (7) (category code 4)
Deductible (6)
$74.00
$82.00
Coinsurance up to Out-of-Pocket Threshold
15%
15%
Maximum Copayments above Out-of-Pocket Threshold
Generic/Preferred Multi-Source Drug
$2.95
$3.30
Other
$7.40
$8.25
Retiree Drug Subsidy Amounts
Cost Threshold
$360
$400
Cost Limit
$7,400
$8,250
(1) Pursuant to section 1860D-2(b)(4)(B)(i)(IV) of the Act, for each of years 2016 through 2019, the Out-
of-Pocket Threshold increase is the lesser of the annual percentage increase or the July CPI plus two
percentage points.
(2) September CPI adjustment applies to copayments for non-institutionalized beneficiaries up to or at
100% FPL.
(3) For beneficiaries who are not considered an “applicable beneficiary” as defined at section 1860D-
14A(g)(1) and are not eligible for the coverage gap program, this is the amount of total drug spending
required to reach the out-of-pocket threshold in the defined standard benefit. Enhanced alternative plans
must use this value when mapping enhanced alternative plans to the defined standard benefit for the
purpose of calculating covered plan paid amounts (CPP) reported on prescription drug event (PDE)
records.
(4) For beneficiaries who are considered an "applicable beneficiary" as defined at section 1860D-
14A(g)(1) and are eligible for the coverage gap discount program, this is the estimated average amount of
total drug spending required to reach the out-of-pocket threshold in the defined standard benefit.
Enhanced alternative plans must use this value when mapping enhanced alternative plans to the defined
standard benefit for the purpose of calculating covered plan paid amounts (CPP) reported on PDE
records.
(5) Per section 1860D-14(a)(1)(D)(i) of the Act, full-benefit dual eligibles who would be institutionalized
individuals (or couple) if the individual (couple) was not receiving home and community-based services
qualify for zero cost-sharing.

70
(6) The increases to the LIS deductible, generic/preferred multi-source drugs and other drugs copayments
are applied to the unrounded 2016 values of $73.79, $1.21, and $3.64, respectively.
(7) These resource limit figures will be updated for contract year 2017.
Section A. Annual Percentage Increase in Average Expenditures for Part D Drugs per
Eligible Beneficiary (API)
Section 1860D-2(b)(6) of the Act defines the API as “the annual percentage increase in average
per capita aggregate expenditures for covered Part D drugs in the United States for Part D
eligible individuals, as determined by the Secretary for the 12-month period ending in July of the
previous year using such methods as the Secretary shall specify.” The following parameters are
updated using the “annual percentage increase”:
Deductible: From $360 in 2016 and rounded to the nearest multiple of $5.
Initial Coverage Limit: From $3,310 in 2016 and rounded to the nearest multiple of $10.
Minimum Cost-Sharing in the Catastrophic Coverage Portion of the Benefit: From $2.95
per generic or preferred drug that is a multi-source drug, and $7.40 for all other drugs in 2016,
and rounded to the nearest multiple of $0.05.
Maximum Copayments up to the Out-of-Pocket Threshold for Certain Low Income Full
Subsidy Eligible Enrollees: From $2.95 per generic or preferred drug that is a multi-source
drug, and $7.40 for all other drugs in 2016, and rounded to the nearest multiple of $0.05.
Deductible for Low Income (Partial) Subsidy Eligible Enrollees: From $74
6
in 2016 and
rounded to the nearest $1.
Maximum Copayments above the Out-of-Pocket Threshold for Low Income (Partial)
Subsidy Eligible Enrollees: From $2.95 per generic or preferred drug that is a multi-source
drug, and $7.40 for all other drugs in 2016, and rounded to the nearest multiple of $0.05.
Section B. Annual Percentage Increase in Consumer Price Index (CPI)
Section 1860D-14(a)(4) of the Act specifies that the annual percentage increase in the CPI, All
Urban Consumers (all items, U.S. city average) as of September of the previous year is used to
update the maximum copayments up to the out-of-pocket threshold for full benefit dual eligible
enrollees with incomes not exceeding 100 percent of the Federal poverty line. These
copayments are increased from $1.20 per generic or preferred drug that is a multi-source drug,
6
Consistent with the statutory requirements of section 1860D-14(a)(4)(B) of the Act, the update
for the deductible for low income (partial) subsidy eligible enrollees is applied to the unrounded
2016 value of $73.79.

71
and $3.60 for all other drugs in 2016
7
, and rounded to the nearest multiple of $0.05 and $0.10,
respectively.
Additionally, section 1860D-2(b)(4) of the Act requires that the “annual percentage increase”
applied to the out-of-pocket threshold in 2017 is CPI+2%, which is the lesser of API and
CPI+2%. The change in CPI in this case is measured over the 12-month period ending in July of
the previous year, as required by statute. The threshold is increased from $4,850 in 2016 and
rounded to the nearest multiple of $50.
Section C. Calculation Methodology
Annual Percentage Increase in Average Expenditures for Part D Drugs per Eligible
Beneficiary (API)
For contract years 2007 and 2008, the APIs, as defined in section 1860D-2(b)(6) of the Act, were
based on the National Health Expenditure (NHE) prescription drug per capita estimates because
sufficient Part D program data was not available. Beginning with contract year 2009, the APIs
are based on Part D program data. For the 2017 contract year benefit parameters, Part D
program data is used to calculate the annual percentage trend as follows:
In the formula, the average per capita cost for August 2014 – July 2015 ($3,379.72) is calculated
from actual Part D prescription drug event (PDE) data and the average per capita cost for August
2015 – July 2016 ($3,615.90) is calculated based on actual Part D PDE data incurred from
August 2015 – December 2015 and projected through July 2016.
The 2017 benefit parameters reflect the 2016 annual percentage trend as well as an update for
revision to prior year estimates for API. Based on updated NHE prescription drug per capita
costs and PDE data, the annual percentage increases are now estimated as summarized by Table
V-2.
7
Consistent with the statutory requirements of section 1860D-14(a)(4)(A) of the Act, the
copayments are increased from the unrounded 2016 values of $1.21per generic or preferred drug
that is a multi-source drug, and $3.64 for all other drugs.

72
Table V-2. Revised Prior Years’ Annual Percentage Increases
Year
Prior Estimates
of Annual
Percentage
Increases
Revised
Annual
Percentage
Increases
2007
7.30%
7.30%
2008
5.92%
5.92%
2009
4.17%
4.69%
2010
3.07%
3.14%
2011
2.48%
2.36%
2012
2.45%
2.16%
2013
1.95%
2.53%
2014
−2.72%
−3.13%
2015
9.18%
10.03%
2016
6.37%
9.91%
Accordingly, the 2017 benefit parameters reflect a multiplicative update of 4.45 percent for prior
year revisions. In summary, the 2016 parameters outlined in Section A are updated by 11.75
percent for 2017, as summarized by Table V-3.
Table V-3. Annual Percentage Increase
Annual percentage trend for July 2016
6.99%
Prior year revisions
4.45%
Annual percentage increase for 2017
11.75%
Note: Percentages are multiplicative, not additive.
Values are carried to additional decimal places and may
not agree to the rounded values presented above.
Annual Percentage Increase in Consumer Price Index, September (September CPI)
To ensure that plan sponsors and CMS have sufficient time to incorporate the cost-sharing
requirements into the development of the benefit, any marketing materials, and necessary
systems, the methodology to calculate the annual percentage increase in the CPI for the 12 month
period ending in September 2016 includes an estimate of the September 2016 CPI based on
projections from the President’s FY2017 Budget.
The September 2015 value is from the Bureau of Labor Statistics. The annual percentage trend
in the September CPI for contract year 2017 is calculated as follows:

73
Projected September 2016 CPI
Actual September 2015 CPI
(Source: President’s FY2017 Budget and Bureau of Labor Statistics, Department of
Labor)
The 2017 benefit parameters reflect the 2016 annual percentage trend in the September CPI of
1.67 percent, as well as a revision to the prior estimate for the 2015 CPI increase over the 12
month period ending in September 2015. Based on the actual reported CPI for September 2015,
the September 2015 CPI increase is now estimated to be −0.04 percent. Accordingly, the 2017
update reflects a −1.46 percent multiplicative correction for the revision to last year’s estimate.
In summary, the maximum copayments below the out-of-pocket threshold for full benefit dual
eligible enrollees with incomes not exceeding 100 percent of the Federal poverty line are updated
by 0.18 percent for 2017, as summarized by Table V-4.
Table V-4. Cumulative Annual Percentage Increase in September CPI
Annual percentage trend for September 2016
1.67%
Prior year revisions
−1.46%
Annual percentage increase for 2017
0.18%
Note: Percentages are multiplicative, not additive.
Values are carried to additional decimal places and may
not agree to the rounded values presented above.
Annual Percentage Increase in Consumer Price Index, July (July CPI)
As is the case when calculating the annual CPI trend as of September 2016, the methodology to
calculate the annual percentage increase in the CPI for the 12 month period ending in July 2016
includes an estimate of the July 2016 CPI based on projections from the President’s FY2017
Budget.
The July 2015 value is from the Bureau of Labor Statistics. The annual percentage trend in CPI
for contract year 2017 is calculated as follows:
Projected July 2016 CPI
Actual July 2015 CPI
(Source: President’s FY2017 Budget and Bureau of Labor Statistics, Department of
Labor)
The 2017 benefit parameters reflect the 2016 annual percentage trend in the July CPI of 1.13
percent as well as a revision to the prior estimate for the 2015 CPI increase. Based on the actual
reported CPI for July 2015, the CPI increase over the 12 month period ending in July 2015 is
estimated to be 0.17 percent. The prior year revision here reflects the difference between this

74
actual 0.17 percent increase in CPI observed in July 2015 and the 2015 CPI increase estimate
from the CY 2016 Rate Announcement, which erroneously used September instead of July CPI
values. Accordingly, the 2017 update reflects a -1.26 percent multiplicative correction for the
revision to last year’s estimate.
In summary, the cumulative annual percentage increase in July CPI for 2017 is -0.15 percent, as
summarized by Table V-5. This value plus two percentage points is less than the 11.75 percent
cumulative API for 2017 described above. Thus, the out-of-pocket threshold will be increased
by 1.85 percent for 2017.
Table V-5. Cumulative Annual Percentage Increase in July CPI
Annual percentage trend for July 2016
1.13%
Prior year revisions
−1.26%
Annual percentage increase for 2017
−0.15%
Note: Percentages are multiplicative, not additive.
Values are carried to additional decimal places and may
not agree to the rounded values presented above.
Section D. Retiree Drug Subsidy Amounts
Per 42 CFR 423.886(b)(3), the cost threshold and cost limit for qualified retiree prescription drug
plans are also updated using the API, as defined previously in this document. The updated cost
threshold is rounded the nearest multiple of $5 and the updated cost limit is rounded to the
nearest multiple of $50. The cost threshold and cost limit are defined as $320 and $6,600,
respectively, for plans that end in 2015, and, as $360 and $7,400, respectively, for plans that end
in 2016. For 2017, the cost threshold is $400 and the cost limit is $8,250.
Section E. Estimated Total Covered Part D Spending at Out-of-Pocket Threshold for
Applicable Beneficiaries
For 2017, the total covered Part D spending at out-of-pocket threshold for applicable
beneficiaries is $8,071.16. The figure is calculated given the following basic assumptions:
100 percent beneficiary cost sharing in the deductible phase.
25 percent beneficiary cost sharing in the initial coverage phase and in the coverage gap.
51 percent beneficiary cost sharing for non-applicable (generic) drugs purchased in the
coverage gap phase of the benefit.
90 percent cost sharing for the ingredient cost and sales tax for applicable (brand) drugs
purchased in the coverage gap phase of the benefit – 40 percent beneficiary coinsurance
and 50 percent coverage gap discount program discount.
40 percent cost sharing for the dispensing and vaccine administration fees for applicable
(brand) drugs purchased in the coverage gap phase of the benefit.

75
In this estimate, it is also assumed that the dispensing and vaccine administration fees account
for 0.11 percent of the gross covered brand drug costs used by non-LIS beneficiaries in the
coverage gap. Therefore, a 60 percent reduction in cost sharing for dispensing and vaccine
administration fees results in an overall reduction of 0.05 percent to 89.95 percent in cost sharing
for applicable (brand) drugs in the coverage gap.
The estimated total covered Part D spending at out-of-pocket threshold for applicable
beneficiaries is calculated as follows:
ICL+
100% beneficiary cost sharing in the gap
weighted gap coinsurance factor
ICL is the Initial Coverage Limit equal to $3,700
One hundred percent beneficiary cost sharing in the gap is the estimated total drug
spending in the gap assuming 100 percent coinsurance.
One hundred percent cost sharing in the gap is calculated as follows:
OOP threshold − OOP costs up to the ICL or $4,950 − $1,225.00 = $3,725.00
Weighted gap coinsurance factor is calculated as follows:
(Brand GDCB % for non-LIS × 89.95% gap cost sharing for applicable drugs) + (Generic
GDCB % for non-LIS × 51% gap cost sharing for non-applicable drugs)
or
(87.9% × 89.95%) + (12.1% × 51%) = 85.218%
Brand GDCB % for non-LIS is the percentage of gross covered drug costs below the out-
of-pocket threshold for applicable beneficiaries (i.e., non-LIS) attributable to applicable
(brand) drugs, as reported on the 2015 PDEs.
Gap cost sharing for applicable drugs is the coinsurance incurred by applicable
beneficiaries (i.e., non-LIS) for applicable (brand) drugs in the coverage gap, where:
Coinsurance for applicable drugs = [(percentage of gross covered brand drug costs
attributable to ingredient cost and sales tax) × (cost sharing percentage)] +
[(percentage of gross covered brand drug costs attributable to dispensing and vaccine
administration fees) × (cost sharing coinsurance percentage)]
or
89.95% = [(99.89% × 90%) + (0.11% × 40%)]
76
Generic GDCB % for non-LIS is the percentage of gross covered drug costs below the
out-of-pocket threshold for applicable beneficiaries (i.e., non-LIS) attributable to non-
applicable (generic) drugs as reported on the 2015 PDEs.
Gap cost sharing for non-applicable drugs is the coinsurance incurred by applicable
beneficiaries (i.e., non-LIS) for non-applicable (generic) drugs in the coverage gap.
77
Attachment VI. CMS-HCC and RxHCC Risk Adjustment Factors
Table VI-1. 2017 CMS-HCC Model Relative Factors for Community and Institutional
Beneficiaries ...................................................... 78
Table VI-2. 2017 CMS-HCC Model Relative Factors for Aged and Disabled New Enrollees . 85
Table VI-3. 2017 CMS-HCC Model Relative Factors for New Enrollees in Chronic
Condition Special Needs Plans (C-SNPs) ................................. 86
Table VI-4. Disease Hierarchies for the 2017 CMS-HCC Model ...................... 87
Table VI-5. RxHCC Model Relative Factors for Continuing Enrollees .................. 88
Table VI-6. RxHCC Model Relative Factors for New Enrollees, Non‑Low Income ........ 93
Table VI-7. RxHCC Model Relative Factors for New Enrollees, Low Income ............ 94
Table VI-8. RxHCC Model Relative Factors for New Enrollees, Institutional ............. 95
Table VI-9. List of Disease Hierarchies for RxHCC Model ......................... 96

78
Table VI-1. 2017 CMS-HCC Model Relative Factors for Community and Institutional Beneficiaries
Variable
Description Label
Community,
NonDual,
Aged
Community,
NonDual,
Disabled
Community,
FBDual,
Aged
Community,
FBDual,
Disabled
Community,
PBDual,
Aged
Community,
PBDual,
Disabled
Institutional
Female
0-34 Years
-
0.244
-
0.318
-
0.344
1.031
35-44 Years
-
0.303
-
0.306
-
0.383
0.999
45-54 Years
-
0.322
-
0.338
-
0.374
1.007
55-59 Years
-
0.350
-
0.388
-
0.371
0.986
60-64 Years
-
0.411
-
0.449
-
0.395
1.028
65-69 Years
0.312
-
0.425
-
0.341
-
1.200
70-74 Years
0.374
-
0.511
-
0.406
-
1.092
75-79 Years
0.448
-
0.611
-
0.484
-
0.995
80-84 Years
0.537
-
0.739
-
0.552
-
0.860
85-89 Years
0.664
-
0.917
-
0.678
-
0.749
90-94 Years
0.797
-
1.037
-
0.817
-
0.626
95 Years or Over
0.816
-
1.094
-
0.913
-
0.456
Male
0-34 Years
-
0.155
-
0.225
-
0.330
1.049
35-44 Years
-
0.190
-
0.204
-
0.267
1.074
45-54 Years
-
0.221
-
0.281
-
0.300
1.008
55-59 Years
-
0.271
-
0.372
-
0.307
1.055
60-64 Years
-
0.303
-
0.486
-
0.343
1.039
65-69 Years
0.300
-
0.492
-
0.334
-
1.269
70-74 Years
0.379
-
0.582
-
0.409
-
1.323
75-79 Years
0.466
-
0.692
-
0.491
-
1.331
80-84 Years
0.561
-
0.816
-
0.546
-
1.189
85-89 Years
0.694
-
1.009
-
0.679
-
1.129
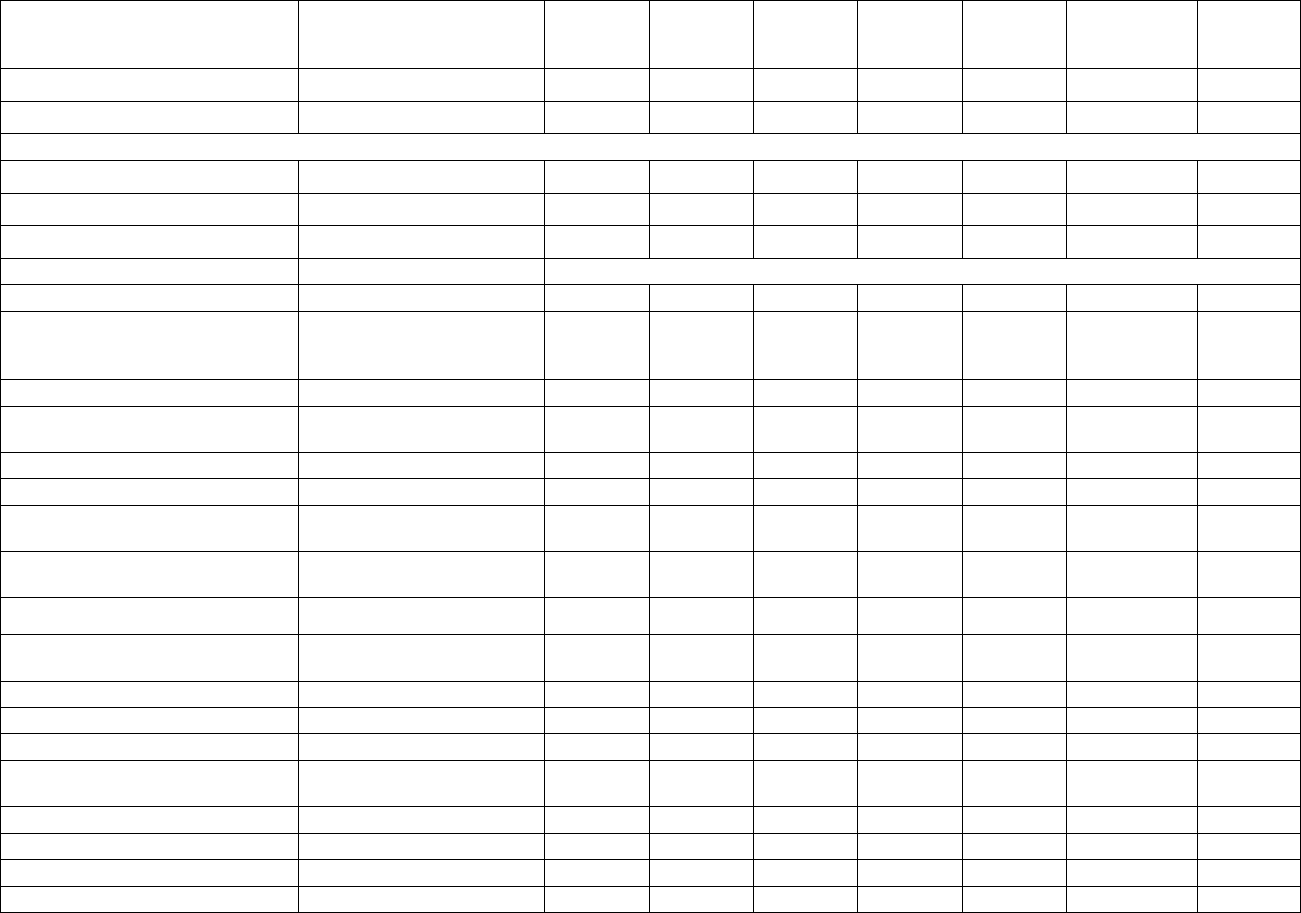
79
Variable
Description Label
Community,
NonDual,
Aged
Community,
NonDual,
Disabled
Community,
FBDual,
Aged
Community,
FBDual,
Disabled
Community,
PBDual,
Aged
Community,
PBDual,
Disabled
Institutional
90-94 Years
0.857
-
1.186
-
0.822
-
0.964
95 Years or Over
0.976
-
1.268
-
1.038
-
0.781
Medicaid and Originally Disabled
Medicaid
-
-
-
-
-
-
0.062
Originally Disabled, Female
0.244
-
0.172
-
0.126
-
-
Originally Disabled, Male
0.152
-
0.192
-
0.105
-
-
Disease Coefficients
Description Label
HCC1
HIV/AIDS
0.312
0.288
0.585
0.500
0.550
0.232
1.747
HCC2
Septicemia, Sepsis, Systemic
Inflammatory Response
Syndrome/Shock
0.455
0.532
0.596
0.811
0.409
0.417
0.346
HCC6
Opportunistic Infections
0.435
0.704
0.548
0.919
0.482
0.765
0.580
HCC8
Metastatic Cancer and Acute
Leukemia
2.625
2.644
2.542
2.767
2.442
2.582
1.143
HCC9
Lung and Other Severe Cancers
0.970
0.927
0.973
1.025
0.955
0.879
0.727
HCC10
Lymphoma and Other Cancers
0.677
0.656
0.713
0.761
0.667
0.577
0.401
HCC11
Colorectal, Bladder, and Other
Cancers
0.301
0.352
0.332
0.361
0.325
0.400
0.293
HCC12
Breast, Prostate, and Other
Cancers and Tumors
0.146
0.202
0.159
0.190
0.152
0.182
0.199
HCC17
Diabetes with Acute
Complications
0.318
0.371
0.346
0.431
0.354
0.423
0.441
HCC18
Diabetes with Chronic
Complications
0.318
0.371
0.346
0.431
0.354
0.423
0.441
HCC19
Diabetes without Complication
0.104
0.128
0.097
0.160
0.098
0.136
0.160
HCC21
Protein-Calorie Malnutrition
0.545
0.753
0.752
0.845
0.562
0.709
0.260
HCC22
Morbid Obesity
0.273
0.227
0.410
0.373
0.244
0.242
0.511
HCC23
Other Significant Endocrine and
Metabolic Disorders
0.228
0.444
0.228
0.353
0.193
0.351
0.337
HCC27
End-Stage Liver Disease
0.962
1.110
1.242
1.349
0.889
0.963
0.962
HCC28
Cirrhosis of Liver
0.390
0.394
0.342
0.491
0.460
0.324
0.390
HCC29
Chronic Hepatitis
0.165
0.267
0.038
0.400
0.263
0.324
0.390
HCC33
Intestinal Obstruction/Perforation
0.246
0.524
0.369
0.503
0.324
0.510
0.335

80
Variable
Description Label
Community,
NonDual,
Aged
Community,
NonDual,
Disabled
Community,
FBDual,
Aged
Community,
FBDual,
Disabled
Community,
PBDual,
Aged
Community,
PBDual,
Disabled
Institutional
HCC34
Chronic Pancreatitis
0.276
0.678
0.333
0.875
0.412
0.849
0.241
HCC35
Inflammatory Bowel Disease
0.294
0.483
0.334
0.613
0.209
0.496
0.244
HCC39
Bone/Joint/Muscle
Infections/Necrosis
0.425
0.474
0.552
0.713
0.418
0.491
0.345
HCC40
Rheumatoid Arthritis and
Inflammatory Connective Tissue
Disease
0.423
0.377
0.370
0.345
0.390
0.290
0.329
HCC46
Severe Hematological Disorders
1.388
3.188
1.219
4.256
1.226
3.529
0.680
HCC47
Disorders of Immunity
0.625
0.848
0.529
0.589
0.449
0.690
0.529
HCC48
Coagulation Defects and Other
Specified Hematological
Disorders
0.221
0.339
0.268
0.378
0.225
0.382
0.151
HCC54
Drug/Alcohol Psychosis
0.383
0.569
0.706
0.919
0.388
0.613
0.102
HCC55
Drug/Alcohol Dependence
0.383
0.285
0.522
0.366
0.377
0.286
0.102
HCC57
Schizophrenia
0.608
0.395
0.612
0.432
0.547
0.366
0.271
HCC58
Major Depressive, Bipolar, and
Paranoid Disorders
0.395
0.209
0.444
0.178
0.413
0.163
0.271
HCC70
Quadriplegia
1.314
1.053
1.098
1.056
1.274
1.328
0.497
HCC71
Paraplegia
1.007
0.704
0.920
1.019
0.958
0.908
0.467
HCC72
Spinal Cord Disorders/Injuries
0.528
0.456
0.552
0.407
0.556
0.384
0.229
HCC73
Amyotrophic Lateral Sclerosis and
Other Motor Neuron Disease
0.970
1.082
1.230
1.219
0.570
0.814
0.224
HCC74
Cerebral Palsy
0.280
0.132
-
-
0.158
0.052
-
HCC75
Myasthenia Gravis/Myoneural
Disorders and Guillain-Barre
Syndrome/Inflammatory and
Toxic Neuropathy
0.457
0.528
0.436
0.465
0.364
0.331
0.369
HCC76
Muscular Dystrophy
0.505
0.457
0.553
0.512
0.429
0.168
0.104
HCC77
Multiple Sclerosis
0.441
0.540
0.687
0.794
0.407
0.459
-
HCC78
Parkinson's and Huntington's
Diseases
0.674
0.585
0.751
0.516
0.629
0.394
0.145
HCC79
Seizure Disorders and
Convulsions
0.309
0.227
0.357
0.195
0.349
0.245
0.088
HCC80
Coma, Brain Compression/Anoxic
Damage
0.584
0.302
0.946
0.324
0.508
0.155
0.042

81
Variable
Description Label
Community,
NonDual,
Aged
Community,
NonDual,
Disabled
Community,
FBDual,
Aged
Community,
FBDual,
Disabled
Community,
PBDual,
Aged
Community,
PBDual,
Disabled
Institutional
HCC82
Respirator
Dependence/Tracheostomy Status
1.055
1.024
2.304
1.575
0.914
0.676
1.631
HCC83
Respiratory Arrest
0.658
0.781
1.033
0.484
0.704
0.429
0.727
HCC84
Cardio-Respiratory Failure and
Shock
0.302
0.578
0.471
0.484
0.301
0.429
0.297
HCC85
Congestive Heart Failure
0.323
0.412
0.355
0.415
0.320
0.367
0.191
HCC86
Acute Myocardial Infarction
0.233
0.306
0.473
0.618
0.280
0.438
0.497
HCC87
Unstable Angina and Other Acute
Ischemic Heart Disease
0.218
0.306
0.336
0.618
0.280
0.438
0.497
HCC88
Angina Pectoris
0.140
0.121
0.068
0.205
0.175
0.220
0.497
HCC96
Specified Heart Arrhythmias
0.268
0.284
0.369
0.377
0.283
0.258
0.224
HCC99
Cerebral Hemorrhage
0.263
0.282
0.474
0.690
0.278
0.280
0.114
HCC100
Ischemic or Unspecified Stroke
0.263
0.195
0.474
0.357
0.270
0.232
0.114
HCC103
Hemiplegia/Hemiparesis
0.538
0.324
0.548
0.435
0.603
0.401
0.031
HCC104
Monoplegia, Other Paralytic
Syndromes
0.395
0.258
0.374
0.381
0.559
0.401
0.031
HCC106
Atherosclerosis of the Extremities
with Ulceration or Gangrene
1.461
1.506
1.744
1.740
1.452
1.601
0.884
HCC107
Vascular Disease with
Complications
0.400
0.486
0.540
0.756
0.443
0.549
0.321
HCC108
Vascular Disease
0.298
0.333
0.324
0.319
0.316
0.326
0.094
HCC110
Cystic Fibrosis
0.620
2.538
0.985
3.365
0.358
2.861
0.305
HCC111
Chronic Obstructive Pulmonary
Disease
0.328
0.262
0.422
0.354
0.358
0.293
0.305
HCC112
Fibrosis of Lung and Other
Chronic Lung Disorders
0.209
0.262
0.134
0.322
0.172
0.174
0.057
HCC114
Aspiration and Specified Bacterial
Pneumonias
0.599
0.530
0.707
0.490
0.666
0.373
0.067
HCC115
Pneumococcal Pneumonia,
Empyema, Lung Abscess
0.221
0.128
0.162
0.049
0.302
0.220
0.067
HCC122
Proliferative Diabetic Retinopathy
and Vitreous Hemorrhage
0.217
0.171
0.223
0.284
0.276
0.195
0.460
HCC124
Exudative Macular Degeneration
0.499
0.385
0.278
0.090
0.336
0.115
0.228
HCC134
Dialysis Status
0.422
0.500
0.672
0.637
0.435
0.512
0.462
HCC135
Acute Renal Failure
0.422
0.500
0.672
0.637
0.435
0.512
0.462

82
Variable
Description Label
Community,
NonDual,
Aged
Community,
NonDual,
Disabled
Community,
FBDual,
Aged
Community,
FBDual,
Disabled
Community,
PBDual,
Aged
Community,
PBDual,
Disabled
Institutional
HCC136
Chronic Kidney Disease, Stage 5
0.237
0.141
0.244
0.167
0.184
0.147
0.436
HCC137
Chronic Kidney Disease, Severe
(Stage 4)
0.237
0.141
0.244
0.079
0.184
0.035
0.202
HCC157
Pressure Ulcer of Skin with
Necrosis Through to Muscle,
Tendon, or Bone
2.163
2.203
2.879
2.626
2.274
2.655
0.924
HCC158
Pressure Ulcer of Skin with Full
Thickness Skin Loss
1.204
1.393
1.576
1.559
1.074
1.237
0.295
HCC161
Chronic Ulcer of Skin, Except
Pressure
0.535
0.636
0.757
0.631
0.586
0.620
0.294
HCC162
Severe Skin Burn or Condition
0.321
0.348
0.003
0.537
0.525
0.119
0.076
HCC166
Severe Head Injury
0.584
0.302
0.946
0.324
1.065
0.155
0.042
HCC167
Major Head Injury
0.191
0.044
0.274
0.171
0.133
0.049
-
HCC169
Vertebral Fractures without Spinal
Cord Injury
0.495
0.456
0.552
0.407
0.516
0.384
0.209
HCC170
Hip Fracture/Dislocation
0.418
0.513
0.520
0.668
0.383
0.484
-
HCC173
Traumatic Amputations and
Complications
0.266
0.340
0.412
0.383
0.233
0.232
0.267
HCC176
Complications of Specified
Implanted Device or Graft
0.597
0.871
0.721
1.156
0.584
0.876
0.502
HCC186
Major Organ Transplant or
Replacement Status
1.000
0.618
0.816
1.075
0.795
0.655
0.962
HCC188
Artificial Openings for Feeding or
Elimination
0.571
0.785
0.775
0.870
0.579
0.867
0.500
HCC189
Amputation Status, Lower
Limb/Amputation Complications
0.588
0.455
0.787
1.065
0.737
0.696
0.407
Disease Interactions
HCC47_gCancer
Immune Disorders*Cancer Group
0.893
0.675
0.815
0.652
0.776
0.808
-
HCC85_gDiabetesMellit
Congestive Heart
Failure*Diabetes Group
0.154
0.096
0.205
0.160
0.178
0.139
0.154
HCC85_gCopdCF
Congestive Heart Failure*Chronic
Obstructive Pulmonary Disease
Group
0.190
0.174
0.240
0.217
0.186
0.181
0.164
HCC85_gRenal
Congestive Heart Failure*Renal
Group
0.270
0.493
0.271
0.711
0.299
0.609
-

83
Variable
Description Label
Community,
NonDual,
Aged
Community,
NonDual,
Disabled
Community,
FBDual,
Aged
Community,
FBDual,
Disabled
Community,
PBDual,
Aged
Community,
PBDual,
Disabled
Institutional
gRespDepandArre_gCopdCF
Cardiorespiratory Failure
Group*Chronic Obstructive
Pulmonary Disease Group
0.336
0.256
0.564
0.524
0.460
0.449
0.423
HCC85_HCC96
Congestive Heart
Failure*Specified Heart
Arrhythmias
0.105
0.285
0.200
0.405
0.116
0.318
-
gSubstanceAbuse_gPsychiatric
Substance Abuse
Group*Psychiatric Group
-
0.191
-
0.233
-
0.230
-
SEPSIS_PRESSURE_ULCER
Sepsis*Pressure Ulcer
-
-
-
-
-
-
0.252
SEPSIS_ARTIF_OPENINGS
Sepsis*Artificial Openings for
Feeding or Elimination
-
-
-
-
-
-
0.568
ART_OPENINGS_PRESSURE_ULCER
Artificial Openings for Feeding or
Elimination*Pressure Ulcer
-
-
-
-
-
-
0.331
gCopdCF_ASP_SPEC_BACT_PNEUM
Chronic Obstructive Pulmonary
Disease*Aspiration and Specified
Bacterial Pneumonias
-
-
-
-
-
-
0.254
ASP_SPEC_BACT_PNEUM_PRES_ULC
Aspiration and Specified Bacterial
Pneumonias*Pressure Ulcer
-
-
-
-
-
-
0.366
SEPSIS_ASP_SPEC_BACT_PNEUM
Sepsis*Aspiration and Specified
Bacterial Pneumonias
-
-
-
-
-
-
0.321
SCHIZOPHRENIA_gCopdCF
Schizophrenia*Chronic
Obstructive Pulmonary Disease
-
-
-
-
-
-
0.363
SCHIZOPHRENIA_CHF
Schizophrenia*Congestive Heart
Failure
-
-
-
-
-
-
0.173
SCHIZOPHRENIA_SEIZURES
Schizophrenia*Seizure Disorders
and Convulsions
-
-
-
-
-
-
0.483
Disabled/Disease Interactions
DISABLED_HCC85
Disabled, Congestive Heart
Failure
-
-
-
-
-
-
0.321
DISABLED_PRESSURE_ULCER
Disabled, Pressure Ulcer
-
-
-
-
-
-
0.608
DISABLED_HCC161
Disabled, Chronic Ulcer of the
Skin, Except Pressure Ulcer
-
-
-
-
-
-
0.369
DISABLED_HCC39
Disabled, Bone/Joint Muscle
Infections/Necrosis
-
-
-
-
-
-
0.567
DISABLED_HCC77
Disabled, Multiple Sclerosis
-
-
-
-
-
-
0.425

84
Variable
Description Label
Community,
NonDual,
Aged
Community,
NonDual,
Disabled
Community,
FBDual,
Aged
Community,
FBDual,
Disabled
Community,
PBDual,
Aged
Community,
PBDual,
Disabled
Institutional
DISABLED_HCC6
Disabled, Opportunistic Infections
-
-
-
-
-
-
0.277
NOTES:
1. The denominator is $9,185.29
2. In the “disease interactions” and “disabled interactions,” the variables are defined as follows:
Immune Disorders = HCC 47
Cancer = HCCs 8-12
Congestive Heart Failure = HCC 85
Diabetes = HCCs 17-19
Chronic Obstructive Pulmonary Disease = HCCs 110-112
Renal = HCCs 134 – 137
Cardiorespiratory Failure = HCCs 82-84
Specified Heart Arrhythmias = HCC 96
Substance Abuse = HCCs 54-55
Psychiatric = HCCs 57-58
Sepsis = HCC 2
Pressure Ulcer = HCCs 157-158
Artificial Openings for Feeding or Elimination = HCC 188
Aspiration and Specified Bacterial Pneumonias = HCC 114
Schizophrenia = HCC 57
Seizure Disorders and Convulsions = HCC 79
Chronic Ulcer of Skin, except Pressure = HCC 161
Bone/Joint/Muscle Infections/Necrosis = HCC 39
Multiple Sclerosis = HCC 77
Opportunistic Infections = HCC 6
SOURCE: RTI International analysis of 2013-2014 Medicare 100% data and RTI International analysis of 2013-2014 Medicare 100% institutional
sample.

85
Table VI-2. 2017 CMS-HCC Model Relative Factors for Aged and Disabled New Enrollees
Non-Medicaid &
Non-Originally
Disabled
Medicaid &
Non-Originally
Disabled
Non-Medicaid &
Originally
Disabled
Medicaid &
Originally
Disabled
Female
0-34 Years
0.664
0.985
-
-
35-44 Years
0.936
1.221
-
-
45-54 Years
1.035
1.337
-
-
55-59 Years
1.004
1.342
-
-
60-64 Years
1.122
1.438
-
-
65 Years
0.522
1.059
1.130
1.566
66 Years
0.516
0.946
1.167
1.619
67 Years
0.544
0.946
1.167
1.619
68 Years
0.581
0.946
1.167
1.619
69 Years
0.605
0.946
1.167
1.619
70-74 Years
0.674
0.975
1.167
1.619
75-79 Years
0.892
1.092
1.167
1.619
80-84 Years
1.066
1.395
1.167
1.619
85-89 Years
1.324
1.458
1.167
1.619
90-94 Years
1.324
1.678
1.167
1.619
95 Years or Over
1.324
1.678
1.167
1.619
Male
0-34 Years
0.456
0.766
-
-
35-44 Years
0.665
1.095
-
-
45-54 Years
0.834
1.357
-
-
55-59 Years
0.889
1.422
-
-
60-64 Years
0.923
1.582
-
-
65 Years
0.514
1.201
0.790
1.613
66 Years
0.533
1.208
0.957
1.613
67 Years
0.575
1.208
1.005
2.202
68 Years
0.641
1.208
1.074
2.202
69 Years
0.671
1.311
1.398
2.202
70-74 Years
0.776
1.311
1.398
2.202
75-79 Years
1.040
1.361
1.398
2.202
80-84 Years
1.270
1.603
1.398
2.202
85-89 Years
1.511
1.850
1.398
2.202
90-94 Years
1.511
1.850
1.398
2.202
95 Years or Over
1.511
1.850
1.398
2.202
NOTES:
1. The denominator is $9,185.29
2. For payment purposes, a new enrollee is a beneficiary who did not have 12 months of Part B eligibility in
the data collection year. CMS-HCC new enrollee models are not based on diagnoses, but include factors for
different age and gender combinations by Medicaid and the original reason for Medicare entitlement.
SOURCE: RTI International analysis of 2013-2014 100% Medicare data.

86
Table VI-3. 2017 CMS-HCC Model Relative Factors for New Enrollees in Chronic
Condition Special Needs Plans (C-SNPs)
Non-Medicaid &
Non-Originally
Disabled
Medicaid &
Non-Originally
Disabled
Non-Medicaid &
Originally
Disabled
Medicaid &
Originally
Disabled
Female
0-34 Years
1.136
1.633
-
-
35-44 Years
1.409
1.868
-
-
45-54 Years
1.507
2.068
-
-
55-59 Years
1.618
2.123
-
-
60-64 Years
1.689
2.177
-
-
65 Years
1.003
1.546
1.747
2.161
66 Years
0.997
1.546
1.785
2.214
67 Years
1.063
1.569
1.805
2.272
68 Years
1.100
1.569
1.805
2.272
69 Years
1.123
1.569
1.805
2.272
70-74 Years
1.269
1.776
1.932
2.415
75-79 Years
1.480
1.973
2.096
2.576
80-84 Years
1.687
2.162
2.252
2.844
85-89 Years
1.920
2.381
2.252
2.844
90-94 Years
1.920
2.602
2.252
2.844
95 Years or Over
1.920
2.602
2.252
2.844
Male
0-34 Years
1.045
1.329
-
-
35-44 Years
1.254
1.658
-
-
45-54 Years
1.503
1.954
-
-
55-59 Years
1.630
2.091
-
-
60-64 Years
1.670
2.187
-
-
65 Years
0.971
1.478
1.655
2.224
66 Years
0.989
1.485
1.691
2.224
67 Years
1.015
1.600
1.705
2.360
68 Years
1.082
1.600
1.734
2.360
69 Years
1.111
1.703
1.780
2.360
70-74 Years
1.302
1.898
1.874
2.356
75-79 Years
1.522
2.080
2.000
2.582
80-84 Years
1.758
2.229
2.254
2.582
85-89 Years
2.047
2.544
2.254
2.582
90-94 Years
2.047
2.544
2.254
2.582
95 Years or Over
2.047
2.544
2.254
2.582
NOTES:
1. The denominator is $9,185.29
2. For payment purposes, a new enrollee is a beneficiary who did not have 12 months of Part B eligibility in the data
collection year. CMS-HCC new enrollee models are not based on diagnoses, but include factors for different age and
gender combinations by Medicaid and the original reason for Medicare entitlement.
3. The relative factors in this table were calculated by estimating the incremental amount to the standard new enrollee risk
model needed to predict the risk scores of continuing enrollees in C-SNPs.
SOURCE: RTI International analysis of 2013-2014 100% Medicare data.

87
Table VI-4. Disease Hierarchies for the 2017 CMS-HCC Model
Hierarchical
Condition
Category
(HCC)
If the Disease Group is Listed in this column…
…Then drop the Disease
Group(s) listed in this
column
Hierarchical Condition Category (HCC) LABEL
8
Metastatic Cancer and Acute Leukemia
9,10,11,12
9
Lung and Other Severe Cancers
10,11,12
10
Lymphoma and Other Cancers
11,12
11
Colorectal, Bladder, and Other Cancers
12
17
Diabetes with Acute Complications
18,19
18
Diabetes with Chronic Complications
19
27
End-Stage Liver Disease
28,29,80
28
Cirrhosis of Liver
29
46
Severe Hematological Disorders
48
54
Drug/Alcohol Psychosis
55
57
Schizophrenia
58
70
Quadriplegia
71,72,103,104,169
71
Paraplegia
72,104,169
72
Spinal Cord Disorders/Injuries
169
82
Respirator Dependence/Tracheostomy Status
83,84
83
Respiratory Arrest
84
86
Acute Myocardial Infarction
87,88
87
Unstable Angina and Other Acute Ischemic Heart
Disease
88
99
Cerebral Hemorrhage
100
103
Hemiplegia/Hemiparesis
104
106
Atherosclerosis of the Extremities with Ulceration or
Gangrene
107,108,161,189
107
Vascular Disease with Complications
108
110
Cystic Fibrosis
111,112
111
Chronic Obstructive Pulmonary Disease
112
114
Aspiration and Specified Bacterial Pneumonias
115
134
Dialysis Status
135,136,137
135
Acute Renal Failure
136,137
136
Chronic Kidney Disease, Stage 5
137
157
Pressure Ulcer of Skin with Necrosis Through to
Muscle, Tendon, or Bone
158,161
158
Pressure Ulcer of Skin with Full Thickness Skin Loss
161
166
Severe Head Injury
80,167
How Payments are Made with a Disease Hierarchy: If a beneficiary triggers Disease Groups 135 (Acute Renal
Failure) and 136 (Chronic Kidney Disease, Stage 5), then DG 136 will be dropped. In other words, payment will
always be associated with the DG in column 1, if a DG in column 3 also occurs during the same collection period.
Therefore, the organization’s payment will be based on DG 135 rather than DG 136.

88
Table VI-5. RxHCC Model Relative Factors for Continuing Enrollees
Continuing Enrollees (CE) RxHCC Model Segments
Variable
Disease Group
Community,
Non-Low
Income,
Age≥65
Community,
Non-Low
Income,
Age<65
Community,
Low
Income,
Age≥65
Community,
Low
Income,
Age<65
Institutional
Female
0-34 Years
-
0.290
-
0.423
1.918
35-44 Years
-
0.477
-
0.637
1.886
45-54 Years
-
0.563
-
0.735
1.682
55-59 Years
-
0.543
-
0.710
1.556
60-64 Years
-
0.504
-
0.645
1.414
65-69 Years
0.264
-
0.407
-
1.491
70-74 Years
0.264
-
0.396
-
1.382
75-79 Years
0.251
-
0.385
-
1.285
80-84 Years
0.237
-
0.357
-
1.197
85-89 Years
0.221
-
0.328
-
1.113
90-94 Years
0.183
-
0.268
-
1.002
95 Years or Over
0.126
-
0.178
-
0.813
Male
0-34 Years
-
0.227
-
0.470
1.660
35-44 Years
-
0.382
-
0.606
1.791
45-54 Years
-
0.498
-
0.660
1.618
55-59 Years
-
0.519
-
0.649
1.450
60-64 Years
-
0.478
-
0.595
1.334
65-69 Years
0.274
-
0.351
-
1.332
70-74 Years
0.279
-
0.353
-
1.275
75-79 Years
0.246
-
0.347
-
1.218
80-84 Years
0.188
-
0.317
-
1.167
85-89 Years
0.149
-
0.289
-
1.098
90-94 Years
0.093
-
0.260
-
1.021
95 Years or Over
0.071
-
0.216
-
0.864
Originally Disabled Interactions with Sex
Originally Disabled_Female
0.101
-
0.180
-
0.066
Originally Disabled_Male
-
-
0.127
-
0.066
Disease Coefficients
Description Label
RXHCC1
HIV/AIDS
2.913
3.350
3.437
3.881
2.206
RXHCC5
Opportunistic Infections
0.221
0.011
0.145
0.148
0.160
RXHCC15
Chronic Myeloid Leukemia
6.271
6.682
7.000
8.912
4.011
RXHCC16
Multiple Myeloma and Other
Neoplastic Disorders
3.405
3.628
2.791
3.246
1.044

89
Continuing Enrollees (CE) RxHCC Model Segments
Variable
Disease Group
Community,
Non-Low
Income,
Age≥65
Community,
Non-Low
Income,
Age<65
Community,
Low
Income,
Age≥65
Community,
Low
Income,
Age<65
Institutional
RXHCC17
Secondary Cancers of Bone,
Lung, Brain, and Other Specified
Sites; Liver Cancer
1.435
1.390
1.346
1.385
0.421
RXHCC18
Lung, Kidney, and Other
Cancers
0.255
0.281
0.280
0.287
0.050
RXHCC19
Breast and Other Cancers and
Tumors
0.087
0.029
0.078
0.085
0.050
RXHCC30
Diabetes with Complications
0.396
0.437
0.461
0.608
0.431
RXHCC31
Diabetes without Complication
0.263
0.259
0.300
0.354
0.299
RXHCC40
Specified Hereditary
Metabolic/Immune Disorders
2.785
11.019
2.945
9.727
0.138
RXHCC41
Pituitary, Adrenal Gland, and
Other Endocrine and Metabolic
Disorders
0.111
0.179
0.052
0.183
0.064
RXHCC42
Thyroid Disorders
0.095
0.160
0.092
0.155
0.065
RXHCC43
Morbid Obesity
0.067
-
0.066
0.068
0.169
RXHCC45
Disorders of Lipoid Metabolism
0.054
0.038
0.094
0.126
0.063
RXHCC54
Chronic Viral Hepatitis C
1.921
2.461
1.713
1.989
0.508
RXHCC55
Chronic Viral Hepatitis, Except
Hepatitis C
0.322
0.396
0.860
0.586
0.251
RXHCC65
Chronic Pancreatitis
0.239
0.238
0.148
0.163
0.143
RXHCC66
Pancreatic Disorders and
Intestinal Malabsorption, Except
Pancreatitis
0.094
0.238
0.084
0.163
0.106
RXHCC67
Inflammatory Bowel Disease
0.470
0.403
0.388
0.718
0.205
RXHCC68
Esophageal Reflux and Other
Disorders of Esophagus
0.098
0.074
0.151
0.170
0.076
RXHCC80
Aseptic Necrosis of Bone
0.162
0.201
0.149
0.135
0.108
RXHCC82
Psoriatic Arthropathy and
Systemic Sclerosis
0.720
0.792
1.116
1.802
0.538
RXHCC83
Rheumatoid Arthritis and Other
Inflammatory Polyarthropathy
0.318
0.383
0.406
0.710
0.172
RXHCC84
Systemic Lupus Erythematosus,
Other Connective Tissue
Disorders, and Inflammatory
Spondylopathies
0.202
0.331
0.233
0.341
0.107
RXHCC87
Osteoporosis, Vertebral and
Pathological Fractures
0.054
0.152
0.121
0.195
-
RXHCC95
Sickle Cell Anemia
0.085
0.185
0.070
0.777
0.482
RXHCC96
Myelodysplastic Syndromes and
Myelofibrosis
0.738
0.883
0.653
0.682
0.518
RXHCC97
Immune Disorders
0.428
0.448
0.484
0.403
0.377
RXHCC98
Aplastic Anemia and Other
Significant Blood Disorders
0.085
0.180
0.070
0.228
0.039
RXHCC111
Alzheimer`s Disease
0.475
0.206
0.180
0.093
-

90
Continuing Enrollees (CE) RxHCC Model Segments
Variable
Disease Group
Community,
Non-Low
Income,
Age≥65
Community,
Non-Low
Income,
Age<65
Community,
Low
Income,
Age≥65
Community,
Low
Income,
Age<65
Institutional
RXHCC112
Dementia, Except Alzheimer`s
Disease
0.198
0.094
0.040
-
-
RXHCC130
Schizophrenia
0.291
0.336
0.457
0.756
0.203
RXHCC131
Bipolar Disorders
0.291
0.319
0.317
0.509
0.203
RXHCC132
Major Depression
0.154
0.269
0.185
0.364
0.189
RXHCC133
Specified Anxiety, Personality,
and Behavior Disorders
0.154
0.239
0.179
0.362
0.106
RXHCC134
Depression
0.150
0.191
0.140
0.227
0.106
RXHCC135
Anxiety Disorders
0.060
0.112
0.092
0.197
0.101
RXHCC145
Autism
0.154
0.239
0.374
0.410
0.106
RXHCC146
Profound or Severe Intellectual
Disability/Developmental
Disorder
0.026
0.114
0.374
0.309
-
RXHCC147
Moderate Intellectual
Disability/Developmental
Disorder
0.026
-
0.224
0.172
-
RXHCC148
Mild or Unspecified Intellectual
Disability/Developmental
Disorder
-
-
0.098
0.030
-
RXHCC156
Myasthenia Gravis,
Amyotrophic Lateral Sclerosis
and Other Motor Neuron Disease
0.316
0.632
0.323
0.542
0.142
RXHCC157
Spinal Cord Disorders
0.138
0.161
0.082
0.059
0.074
RXHCC159
Inflammatory and Toxic
Neuropathy
0.212
0.421
0.219
0.388
0.088
RXHCC160
Multiple Sclerosis
1.904
3.250
1.807
3.809
0.856
RXHCC161
Parkinson`s and Huntington`s
Diseases
0.496
0.716
0.313
0.430
0.208
RXHCC163
Intractable Epilepsy
0.293
0.494
0.260
0.899
0.078
RXHCC164
Epilepsy and Other Seizure
Disorders, Except Intractable
Epilepsy
0.112
0.046
0.034
0.139
-
RXHCC165
Convulsions
0.062
-
0.034
0.087
-
RXHCC166
Migraine Headaches
0.142
0.257
0.126
0.150
0.126
RXHCC168
Trigeminal and Postherpetic
Neuralgia
0.133
0.260
0.149
0.181
0.185
RXHCC185
Primary Pulmonary
Hypertension
0.621
1.784
0.570
1.468
0.229
RXHCC186
Congestive Heart Failure
0.176
0.120
0.230
0.136
0.135
RXHCC187
Hypertension
0.141
0.078
0.204
0.109
0.065
RXHCC188
Coronary Artery Disease
0.130
0.035
0.142
-
0.012
RXHCC193
Atrial Arrhythmias
0.230
0.097
0.098
0.014
0.068

91
Continuing Enrollees (CE) RxHCC Model Segments
Variable
Disease Group
Community,
Non-Low
Income,
Age≥65
Community,
Non-Low
Income,
Age<65
Community,
Low
Income,
Age≥65
Community,
Low
Income,
Age<65
Institutional
RXHCC206
Cerebrovascular Disease, Except
Hemorrhage or Aneurysm
0.052
-
0.039
-
-
RXHCC207
Spastic Hemiplegia
0.174
0.167
0.067
0.193
-
RXHCC215
Venous Thromboembolism
0.111
0.151
0.069
0.115
0.039
RXHCC216
Peripheral Vascular Disease
-
-
0.037
-
-
RXHCC225
Cystic Fibrosis
0.365
3.541
0.352
3.683
0.775
RXHCC226
Chronic Obstructive Pulmonary
Disease and Asthma
0.311
0.144
0.352
0.249
0.200
RXHCC227
Pulmonary Fibrosis and Other
Chronic Lung Disorders
0.159
0.144
0.128
0.249
0.029
RXHCC241
Diabetic Retinopathy
0.260
0.202
0.191
0.119
0.151
RXHCC243
Open-Angle Glaucoma
0.266
0.199
0.306
0.260
0.222
RXHCC260
Kidney Transplant Status
0.328
0.070
0.407
0.393
0.201
RXHCC261
Dialysis Status
0.183
0.274
0.389
0.757
0.301
RXHCC262
Chronic Kidney Disease Stage 5
0.086
0.030
0.091
0.033
0.065
RXHCC263
Chronic Kidney Disease Stage 4
0.086
0.030
0.086
0.033
0.065
RXHCC311
Chronic Ulcer of Skin, Except
Pressure
0.143
0.131
0.071
0.090
0.048
RXHCC314
Pemphigus
0.271
1.212
0.203
0.193
0.048
RXHCC316
Psoriasis, Except with
Arthropathy
0.188
0.219
0.345
0.630
0.228
RXHCC355
Narcolepsy and Cataplexy
0.780
1.325
0.641
1.302
0.350
RXHCC395
Lung Transplant Status
1.126
0.954
1.169
1.160
0.639
RXHCC396
Major Organ Transplant Status,
Except Lung, Kidney, and
Pancreas
1.098
0.954
1.169
1.160
0.457
RXHCC397
Pancreas Transplant Status
0.251
0.070
0.407
0.393
0.201
Non-Aged Disease Interactions
NonAged_RXHCC1
NonAged * HIV/AIDS
-
-
-
-
1.009
NonAged_RXHCC130
NonAged * Schizophrenia
-
-
-
-
0.268
NonAged_RXHCC131
NonAged * Bipolar Disorders
-
-
-
-
0.268
NonAged_RXHCC132
NonAged * Major Depression
-
-
-
-
0.206
NonAged_RXHCC133
NonAged * Specified Anxiety,
Personality, and Behavior
Disorders
-
-
-
-
0.130
NonAged_RXHCC134
NonAged * Depression
-
-
-
-
0.122
NonAged_RXHCC135
NonAged * Anxiety Disorders
-
-
-
-
0.049
NonAged_RXHCC145
NonAged * Autism
-
-
-
-
0.130
NonAged_RXHCC160
NonAged * Multiple Sclerosis
-
-
-
-
1.227
NonAged_RXHCC163
NonAged * Intractable Epilepsy
-
-
-
-
0.111
92
Note: The Part D Denominator used to calculate relative factors is $1,014.31. This Part D Denominator is based on
the combined PDP and MA-PD populations.
Source: RTI Analysis of 100% 2014 PDE, 2013 Carrier NCH, 2013 Inpatient SAF, 2013 Outpatient SAF, 2014
HPMS, 2014 CME, 2013-2014 Denominator, Part D Intermediate File, and 2013 Medicare Advantage Diagnoses
File.
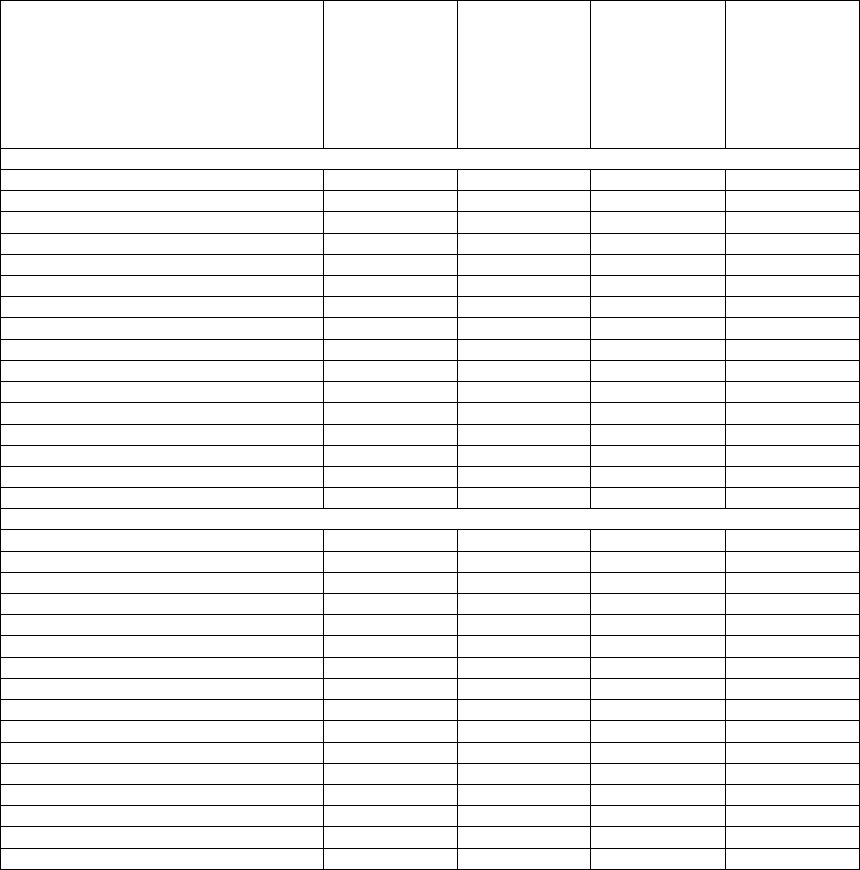
93
Table VI-6. RxHCC Model Relative Factors for New Enrollees, Non‑Low Income
Variable
Not
Concurrently
ESRD, Not
Originally
Disabled
Concurrently
ESRD, Not
Originally
Disabled
Originally
Disabled, Not
Concurrently
ESRD
Originally
Disabled,
Concurrently
ESRD
Female
0-34 Years
0.653
0.653
-
-
35-44 Years
1.074
1.100
-
-
45-54 Years
1.290
1.536
-
-
55-59 Years
1.228
1.732
-
-
60-64 Years
1.227
1.898
-
-
65 Years
0.562
1.756
1.163
1.756
66 Years
0.616
1.756
1.111
1.756
67 Years
0.623
1.756
1.111
1.756
68 Years
0.645
1.756
1.111
1.756
69 Years
0.669
1.756
1.111
1.756
70-74 Years
0.688
1.756
1.100
1.756
75-79 Years
0.687
1.756
0.687
1.756
80-84 Years
0.643
1.756
0.643
1.756
85-89 Years
0.537
1.756
0.537
1.756
90-94 Years
0.317
1.756
0.317
1.756
95 Years or Over
0.317
1.756
0.317
1.756
Male
0-34 Years
0.427
0.714
-
-
35-44 Years
0.803
0.885
-
-
45-54 Years
1.091
1.493
-
-
55-59 Years
1.152
1.493
-
-
60-64 Years
1.110
1.836
-
-
65 Years
0.595
1.773
0.961
1.773
66 Years
0.657
1.773
0.925
1.773
67 Years
0.668
1.773
0.925
1.773
68 Years
0.686
1.773
0.925
1.773
69 Years
0.714
1.773
0.925
1.773
70-74 Years
0.745
1.773
0.762
1.773
75-79 Years
0.737
1.773
0.737
1.773
80-84 Years
0.657
1.773
0.657
1.773
85-89 Years
0.545
1.773
0.545
1.773
90-94 Years
0.332
1.773
0.332
1.773
95 Years or Over
0.332
1.773
0.332
1.773
Notes:
1. The Part D Denominator used to calculate relative factors is $1,014.31. This Part D Denominator is based on
the combined PDP and MA-PD populations.
2. Originally Disabled is defined as originally entitled to Medicare by disability only (OREC = 1).
3. For new enrollees, the concurrent ESRD marker is defined as at least one month in the payment year of ESRD
status—dialysis, transplant, or post-graft.
Source: RTI Analysis of 100% 2014 PDE, 2013 Carrier NCH, 2013 Inpatient SAF, 2013 Outpatient SAF, 2014
HPMS, 2014 CME, 2013-2014 Denominator, Part D Intermediate File, and 2013 Medicare Advantage Diagnoses
File.

94
Table VI-7. RxHCC Model Relative Factors for New Enrollees, Low Income
Variable
Not
Concurrently
ESRD, Not
Originally
Disabled
Concurrently
ESRD, Not
Originally
Disabled
Originally
Disabled, Not
Concurrently
ESRD
Originally
Disabled,
Concurrently
ESRD
Female
0-34 Years
1.003
2.079
-
-
35-44 Years
1.494
2.079
-
-
45-54 Years
1.538
2.170
-
-
55-59 Years
1.428
2.224
-
-
60-64 Years
1.325
2.081
-
-
65 Years
0.924
2.084
1.186
2.084
66 Years
0.600
2.084
0.906
2.084
67 Years
0.600
2.084
0.906
2.084
68 Years
0.600
2.084
0.906
2.084
69 Years
0.600
2.084
0.906
2.084
70-74 Years
0.616
2.084
0.749
2.084
75-79 Years
0.683
2.084
0.683
2.084
80-84 Years
0.683
2.084
0.683
2.084
85-89 Years
0.683
2.084
0.683
2.084
90-94 Years
0.534
2.084
0.534
2.084
95 Years or Over
0.534
2.084
0.534
2.084
Male
0-34 Years
0.869
2.154
-
-
35-44 Years
1.265
2.125
-
-
45-54 Years
1.390
2.131
-
-
55-59 Years
1.251
1.968
-
-
60-64 Years
1.161
1.847
-
-
65 Years
0.831
1.921
0.978
1.921
66 Years
0.507
1.921
0.569
1.921
67 Years
0.507
1.921
0.569
1.921
68 Years
0.507
1.921
0.569
1.921
69 Years
0.507
1.921
0.569
1.921
70-74 Years
0.523
1.921
0.612
1.921
75-79 Years
0.536
1.921
0.536
1.921
80-84 Years
0.559
1.921
0.559
1.921
85-89 Years
0.487
1.921
0.487
1.921
90-94 Years
0.362
1.921
0.362
1.921
95 Years or Over
0.362
1.921
0.362
1.921
Notes:
1. The Part D Denominator used to calculate relative factors is $1,014.31. This Part D Denominator is based on
the combined PDP and MA-PD populations.
2. Originally Disabled is defined as originally entitled to Medicare by disability only (OREC = 1).
3. For new enrollees, the concurrent ESRD marker is defined as at least one month in the payment year of ESRD
status—dialysis, transplant, or post-graft.
Source: RTI Analysis of 100% 2014 PDE, 2013 Carrier NCH, 2013 Inpatient SAF, 2013 Outpatient SAF, 2014
HPMS, 2014 CME, 2013-2014 Denominator, Part D Intermediate File, and 2013 Medicare Advantage Diagnoses
File.

95
Table VI-8. RxHCC Model Relative Factors for New Enrollees, Institutional
Variable
Not
Concurrently
ESRD
Concurrently
ESRD
Female
0-34 Years
2.353
2.767
35-44 Years
2.353
2.767
45-54 Years
2.405
2.767
55-59 Years
2.400
2.767
60-64 Years
2.137
2.767
65 Years
2.280
2.767
66 Years
1.970
2.767
67 Years
1.970
2.767
68 Years
1.970
2.767
69 Years
1.970
2.767
70-74 Years
1.820
2.767
75-79 Years
1.545
2.767
80-84 Years
1.514
2.767
85-89 Years
1.321
2.767
90-94 Years
1.082
2.767
95 Years or Over
1.082
2.767
Male
0-34 Years
2.290
2.614
35-44 Years
2.692
2.614
45-54 Years
2.340
2.614
55-59 Years
2.124
2.614
60-64 Years
2.011
2.614
65 Years
2.002
2.614
66 Years
1.889
2.614
67 Years
1.889
2.614
68 Years
1.889
2.614
69 Years
1.889
2.614
70-74 Years
1.791
2.614
75-79 Years
1.676
2.614
80-84 Years
1.467
2.614
85-89 Years
1.343
2.614
90-94 Years
1.343
2.614
95 Years or Over
1.343
2.614
Notes:
1. The Part D Denominator used to calculate relative factors is $1,014.31. This Part D Denominator is based on
the combined PDP and MA-PD populations.
2. For new enrollees, the concurrent ESRD marker is defined as at least one month in the payment year of ESRD
status—dialysis, transplant, or post-graft.
Source: RTI Analysis of 100% 2014 PDE, 2013 Carrier NCH, 2013 Inpatient SAF, 2013 Outpatient SAF, 2014
HPMS, 2014 CME, 2013-2014 Denominator, Part D Intermediate File, and 2013 Medicare Advantage Diagnoses
File.

96
Table VI-9. List of Disease Hierarchies for RxHCC Model
Rx Hierarchical Condition
Category (RxHCC)
If the Disease Group is listed in this column…
…Then drop the Disease Group(s) listed in
this column
Rx Hierarchical Condition Category (RxHCC) LABEL
15
Chronic Myeloid Leukemia
16 ,17 ,18 ,19 ,96 ,98
16
Multiple Myeloma and Other Neoplastic Disorders
17 ,18 ,19 ,96 ,98
17
Secondary Cancers of Bone, Lung, Brain, and Other Specified Sites; Liver
Cancer
18 ,19
18
Lung, Kidney, and Other Cancers
19
30
Diabetes with Complications
31
54
Chronic Viral Hepatitis C
55
65
Chronic Pancreatitis
66
82
Psoriatic Arthropathy and Systemic Sclerosis
83 ,84 ,316
83
Rheumatoid Arthritis and Other Inflammatory Polyarthropathy
84
95
Sickle Cell Anemia
98
96
Myelodysplastic Syndromes and Myelofibrosis
98
111
Alzheimer's Disease
112
130
Schizophrenia
131 ,132 ,133 ,134 ,135 ,145 ,146 ,147 ,148
131
Bipolar Disorders
132 ,133 ,134 ,135
132
Major Depression
133 ,134 ,135
133
Specified Anxiety, Personality, and Behavior Disorders
134 ,135
134
Depression
135
145
Autism
133 ,134 ,135 ,146 ,147 ,148
146
Profound or Severe Intellectual Disability/Developmental Disorder
147 ,148
147
Moderate Intellectual Disability/Developmental Disorder
148
163
Intractable Epilepsy
164 ,165
164
Epilepsy and Other Seizure Disorders, Except Intractable Epilepsy
165
185
Primary Pulmonary Hypertension
186 ,187
186
Congestive Heart Failure
187
225
Cystic Fibrosis
226 ,227
226
Chronic Obstructive Pulmonary Disease and Asthma
227
260
Kidney Transplant Status
261 ,262 ,263 ,397
261
Dialysis Status
262 ,263
262
Chronic Kidney Disease Stage 5
263
395
Lung Transplant Status
396 ,397
396
Major Organ Transplant Status, Except Lung, Kidney, and Pancreas
397
How Payments are made with a Disease Hierarchy: EXAMPLE: If a beneficiary triggers Disease Groups 163
(Intractable Epilepsy) and 164 (Epilepsy and Other Seizure Disorders, Except Intractable Epilepsy), then DG 164
will be dropped. In other words, payment will always be associated with the DG in column 1, if a DG in column 3
also occurs during the same collection period. Therefore, the organization’s payment will be based on DG 163 rather
than DG 164.
Source: RTI International.
97
Attachment VII: CY 2017 Final Call Letter
CY 2017 Call Letter
Table of Contents
Attachment VII: CY 2017 Final Call Letter ..................................... 97
How to Use This Call Letter ............................................... 101
Section I – Parts C and D .................................................. 102
Annual Calendar ..................................................... 102
Incomplete and Inaccurate Bid Submissions ................................. 109
Incomplete Submissions ............................................. 109
Inaccurate Submissions ............................................. 110
Plan Corrections ..................................................... 110
Contracting Organizations with Ratings of Fewer Than Three Stars in Three Consecutive
Years – Timeline for Application of Termination Authority ................. 111
Enhancements to the 2017 Star Ratings and Beyond ........................... 112
Changes to Measures for 2017 ........................................ 113
Removal of Measures from Star Ratings ................................. 115
Data Integrity..................................................... 117
Impact of Socio-economic and Disability Status on Star Ratings ............... 118
CMS Research .................................................... 119
Interim Analytical Adjustments ....................................... 121
Categorical Adjustment Index Methodology .............................. 125
2017 Categorical Adjustment Index Values ............................... 128
2017 CMS Display Measures ......................................... 138
Forecasting to 2018 and Beyond ....................................... 140
New Measures ................................................. 140
Changes to Existing Star Ratings and Display Measures and Potential Future
Changes ................................................... 144
Measurement and Methodological Enhancements .......................... 150
Medicare Parts C & D Program Audits ..................................... 151
Proposed Release Date for the 2017 Part C and Part D Program Audit Protocols .... 151
Medicare Parts C & D Enforcement Actions ................................. 152
Civil Money Penalty (CMP) Calculation Methodology ...................... 152
Compliance and Enforcement Actions Related to Part D Auto-Forwards ......... 153
Enforcement Actions Related to One Third Financial Audit Findings ............ 154
Innovations in Health Plan Design ........................................ 154
Medicare Advantage Value-Based Insurance Design Model Test ............... 154
Part D Enhanced MTM Model ........................................ 155
Section II – Part C ....................................................... 156
98
Guidance on the Future of Provider Directory Requirements and Best Practices ....... 156
Overview of CY 2017 Benefits and Bid Review .............................. 158
Plans with Low Enrollment ............................................. 160
Meaningful Difference (Substantially Duplicative Plan Offerings) ................. 161
Total Beneficiary Cost (TBC) ........................................... 163
Maximum Out-of-Pocket (MOOP) Limits .................................. 167
Per Member Per Month (PMPM) Actuarial Equivalent (AE) Cost Sharing Limits ...... 168
Part C Cost Sharing Standards ........................................... 170
Part C Optional Supplemental Benefits ..................................... 174
Plan Benefit Package (PBP) Updates and Guidance ............................ 174
Projected Member Months ........................................... 174
Medical Services Performed in Multiple Health Care Settings ................. 174
Medicare-Covered Preventive Services .................................. 177
Policy Updates ...................................................... 178
Tiered Cost Sharing of Medical Benefits ................................. 178
Cost Sharing /Bundling and Facility .................................... 178
Interoperability-MA Plans and Contracted Providers ........................ 179
Alternative Payment Models (APMs) ................................... 180
Connecting Beneficiaries to Care ...................................... 181
Counseling and Related Support Services ................................ 181
Prohibition on Billing Medicare-Medicaid Enrollees for Medicare Cost-Sharing .... 181
Medicare Advantage Organization Responsibilities for Clinical Trials ........... 183
Dual-Eligible Special Needs Plans ........................................ 184
D-SNP Non-Renewals .............................................. 185
D-SNP Model of Care .............................................. 185
Section III – Part D ...................................................... 186
Formulary Submissions ................................................ 186
CY 2017 Formulary Submission Window ................................ 186
CY 2017 Formulary Reference File..................................... 186
Appropriate Utilization of Prior Authorization Requirements to Determine Part D
Drug Status ................................................ 188
Medication Therapy Management (MTM) .................................. 189
Annual MTM Eligibility Cost Threshold ................................. 189
Annual MTM Submission and Approval Process ........................... 189
Submission Requirements for Enhanced MTM Model Participants .............. 190
Part D Reporting Requirements for MTM ................................ 191
Improving Clinical Decision-Making for Certain Part D Coverage Determinations ..... 191
Access to Preferred Cost-Sharing Pharmacies ................................ 194
Part D Benefit Parameters for Non-Defined Standard Plans ...................... 195
Tier Labeling and Composition ........................................ 196
99
Benefit Review ................................................... 198
Specialty Tiers .................................................... 202
Generic Tier $0 Copay Plans ......................................... 203
Part D Employer Group Waiver Plans (EGWPs) .............................. 204
Improving Drug Utilization Review Controls in Medicare Part D .................. 206
New Expectation for Entering Opioid Point of Sale Claims Edit Information in the
Medicare Advantage and Prescription Drug System (MARx) ............ 207
Results of Overutilization Policy....................................... 208
Updates to Overutilization Policy for Contract Year (CY) 2017 ................... 209
Discontinuation of APAP Reporting through the OMS....................... 209
Opioids ......................................................... 209
Compliance Activities and Changes to the OMS Opioid Overutilization
Methodology ............................................... 209
CMS’ Expectation for Formulary-Level Cumulative Opioid POS Edits in CY
2017 ...................................................... 212
Concurrent Use of Opioids and Buprenorphine ......................... 214
Concurrent Use of Opioids and Benzodiazepines ........................ 214
Access to Medication-Assisted Treatment ............................. 215
A Note about the Centers for Disease Control and Prevention (CDC) Guideline
for Prescribing Opioids for Chronic Pain ........................... 216
Point of Sale Pilot .................................................... 217
Extended Days’ Supply and First Fill Quantity Limits .......................... 220
Establishing Mail Order Protocols for Urgent Need Fills to Prevent Gaps in Therapy ... 221
Coordination of Benefits (COB) User Fee ................................... 222
Part D Low Enrollment ................................................ 222
Section IV – Medicare-Medicaid Plans........................................ 223
Medicare-Medicaid Plan Annual Requirements and Timeline for CY 2017 .......... 223
Network Adequacy Determinations..................................... 224
Model of Care (MOC) .............................................. 224
Formulary and Supplemental Drug Files ................................. 225
Plan Benefit Package (PBP) .......................................... 226
Past Performance Information and Eligibility for Passive and Opt-in Enrollment .... 227
Appendix 1 – Contract Year 2017 Guidance for Prescription Drug Plan (PDP) Renewals and
Non-Renewals (Updated) ............................................ 228
1. New Plan Added ................................................... 229
2. Renewal Plan ...................................................... 229
3. Consolidated Renewal Plan ........................................... 229
4. Renewal Plan with a Service Area Expansion (“800 Series” EGWPs only) ........ 230
5. Terminated Plan (Non-Renewal)........................................ 230
100
6. Consolidated Plans under a Parent Organization ............................ 230
Appendix 2 – Contract Year 2017 Guidance for Prescription Drug Plan (PDP) Renewals and
Non-Renewals Table ............................................... 232
Appendix 3 – Improvement Measures (Part C & D) .............................. 237
Appendix 4 - 2017 Draft Call Letter Star Ratings Summary of Comments and Responses .. 240
Appendix 5 – Adjusted Measure Selection Criteria ............................... 250

101
How to Use This Call Letter
The 2017 Call Letter contains information on the Part C and Part D programs that Medicare
Advantage Organizations (MAOs), Part D sponsors, and Medicare-Medicaid Plans (MMPs) need
to take into consideration in preparing their 2017 bids.
CMS has designed the policies contained in this Call Letter to improve the overall management
of the Medicare Advantage and Prescription Drug programs with four major outcomes in mind.
These outcomes are: 1) improvement in quality of care for individuals, 2) promotion of
alternative payment models, 3) program integrity and beneficiary/tax-payer value, and 4)
improvement in beneficiary experience. This year, to achieve these outcomes, CMS’s Call Letter
activities follow four major themes: improving bid review, decreasing costs, promoting creative
benefit designs, and improving beneficiary protections.
If you have questions concerning this Call Letter, please contact: Wanda Pigatt-Canty at
(Part D issues) and [email protected] (MMP issues).

102
Section I – Parts C and D
Annual Calendar
Below is a combined calendar listing of side-by-side key dates and timelines for
operational activities that pertain to Medicare Advantage (MA), Medicare Advantage-
Prescription Drug) (MA-PD), Prescription Drug Plan (PDP), Medicare-Medicaid Plan
(MMP), and cost-based plans. The calendar provides important operational dates for
all organizations such as the date bids are due to CMS, the date that organizations
must inform CMS of their contract non-renewal, and dates for beneficiary mailings.
2017*Note: The dates listed under Part C include MA and MA-PD plans.
The
dates listed under Part D also apply to MA and cost-based plans
offering a Part D benefit.
*Part
C
*Part
D
Cost
MMP
January 12, 2016
Release of Contract Year CY 2017 Initial and Service Area
Applications for MA/MA-PD/PDP, SNP, EGWP, 1876
Cost Plan Expansions
January 12, 2016
MOC Renewal Submission period begins for SNP and
MMP MOCs with approvals ending at the end of CY 2016
January 12 & 14,
2016
Industry Training and Technical Assistance for CY 2017
Model
of Care (MOC) Submissions
January 13 & 20,
2016
Industry training on 2017 Applications
January 15, 2016
Deadline for D-SNPs meeting a high level of integration, as
determined by CMS, to submit a request to CMS to offer
additional supplemental benefits
February 17, 2016
CY 2017 Initial and Service Area Expansion Application
for MA/MA-PD/PDP, SNP, EGWP, 1876 Cost Plan
Expansion are due in HPMS by 8pm EST
February 17, 2016
MOC Renewals Submissions for SNP and MMP MOCs
with approvals ending at the end of CY 2016 are due in
HPMS by 8pm EST.
Late February,
2016
Submission of meaningful use HITECH attestation for
qualifying MA Employer Plans and MA-affiliated hospitals
Early-Mid
February,
2016
D-SNPs that requested to offer additional supplemental
benefits
are notified by CMS as to whether they meet
required
qualifications
February 2016
CMS notifies MA, MA-PDs and PDPs regarding non-
renewal of their contract(s) for CY 2017 due to consistently
low star ratings
February 2016
CMS releases guidance concerning updates to Parent
Organization designations in HPMS
March 17, 2016
Parent Organization Update requests from sponsors due to
CMS
(instructional memo released in February 2016)
Mid-Late March,
2016
Release of CY 2017 Formulary Training Video and 2017
Formulary Reference File (FRF)
March 25, 2016
Release of the Fiscal Soundness Module in HPMS
March/April, 2016
CMS coordinates with MAOs and PDP Sponsors to resolve
low
enrollment issues for CY 2017

103
2017*Note: The dates listed under Part C include MA and MA-PD plans.
The
dates listed under Part D also apply to MA and cost-based plans
offering a Part D benefit.
*Part
C
*Part
D
Cost
MMP
Early April, 2016
CY 2017 Out Of Pocket Cost (OOPC) model and OOPC
estimates for each plan made available to MAOs, 1876 Cost
Plans submitting MA conversion bids, and Part D
sponsors
for download from the CMS website. Information will
assist
plans in meeting meaningful difference and Total
Beneficiary Cost (TBC) requirements prior to bid
submission
Early April, 2016
Information about renewal options for contract year 2017
(including HPMS crosswalk charts) provided to plans
April 2016
Summary of Benefits guidance released
April 2016
Conference call with industry to discuss the 2017 Call
Letter
April 4, 2016
Release of the 2017 Final Announcement of Medicare
Advantage Capitation
Rates and MA and Part D Payment
Policies released, including the CY 2017 Call Letter
April 6, 2016
Industry training on CY 2017 Formulary Submission
April 8, 2016
Release of the 2017 Plan Benefit Package (PBP) online
training
module
April 8, 2016
Release of the 2017 Plan Creation Module, PBP, and Bid
Pricing Tool (BPT) software in HPMS
April 8, 2016
Deadline for upload of Provider Specific Plan (PSP) full
network
April 11, 2016
Deadline for MAOs to submit requests for full contract
consolidations for CY 2017
Mid-April, 2016
Release of HPMS Memo: Contract Year 2017 Medicare
Advantage Bid Review and Operations Guidance
April 18, 2016
Release of the 2017 Medication Therapy Management
(MTM)
Program Submission in HPMS
April 20, 2016
Industry training dedicated to Annual Part D Formulary and
Benefit Compliance Training
Mid-Late April,
2016
MAOs submit plan requests for tiering of medical benefits
and
justifications to CMS for review and consideration
Late April, 2016
Total Beneficiary Cost data for CY 2017 Bid Preparation
Release
May, 2016
Final ANOC/EOC, LIS rider, Part D EOB, formularies,
transition notice, provider directory, pharmacy directory,
and MMP models for 2017 available for all organizations
May 1, 2016
MA, MA-PD and PDP plans to notify CMS of intention to
non-
renew a county (ies) for individuals, but continue the
county
(ies) for “800 series” EGWP members, convert to
offering
employer-only contracts, or reduce its service area
at the
contract level. This will allow CMS to make the
required
changes in HPMS to facilitate the correct upload of
bids in June

104
2017*Note: The dates listed under Part C include MA and MA-PD plans.
The
dates listed under Part D also apply to MA and cost-based plans
offering a Part D benefit.
*Part
C
*Part
D
Cost
MMP
May 2, 2016
Deadline for submission of CY 2017 MTM Programs from
all
sponsors offering Part D including Medicare-Medicaid
Plans
(except those participating in the Enhanced MTM
Model test) (11:59pm PDT)
May 5, 2016
2016 Medicare Advantage & Prescription Drug Plan Spring
Conference & Webcast
May 6, 2016
Release of the 2017 Bid Upload Functionality in HPMS
May 6, 2016
Release of 2017 Actuarial Certification Module in HPMS
May 16, 2016
Release of 2017 Formulary Submission Module in HPMS
May 18, 2016
Deadline for submission of CY 2017 MTM Program
attestations from all sponsors offering Part D including
Medicare-Medicaid Plans (except those participating in the
Enhanced MTM Model test) (11:59pm PDT)
Mid-Late May,
2016
Release of CY 2017 Formulary Reference File Update
May 27, 2016
Plans/Part D sponsors begin to upload agent/broker
compensation information in HPMS
May 27, 2016
Release of the 2017 Marketing Module in HPMS.
Plans/Part D sponsors begin to submit 2017 marketing
materials
Late May/Early
June, 2016
Release of the 2017 Medicare Marketing Guidelines in
HPMS
Late May, 2016
CMS sends qualification determinations to applicants based
on
review of the 2017 applications for new contracts or
service
area expansions
May 31, 2016
Release of CY 2015 Medical Loss Ratio (MLR) Report
software in HPMS
June 2016
Release of state-specific marketing guidance for MMPs.
June 1, 2016
Release of the 2015 DIR Submission Module in HPMS
June 6, 2016
Deadline for submission of CY 2017 bids (including
Service Area Verification) for all MA plans,
MA-PD plans,
PDP, cost-based plans offering a Part D benefit,
Medicare-
Medicaid Plans (MMPs), “800 series” EGWP and
direct
contract EGWP applicants and renewing organizations;
deadline for cost-based plans wishing to appear in the 2017
Medicare Plan Finder to submit PBPs (11:59 p.m. PDT)
Deadline for submission of CY 2017 Formularies,
Transition
Attestations, Prior Authorization/Step Therapy
(PA/ST)
Attestations, and P&T Attestations due from all
sponsors
offering Part D including Medicare-Medicaid
Plans (11:59 p.m.
PDT)
Deadline for submission of a CY 2017 contract non-
renewal,
service area reduction notice to CMS from MA
plans, MA-PD
plans, PDPs and Medicare cost-based
contractors and cost-
based sponsors to Deadline also
applies to an MAO that intends
to terminate a current MA
and/or MA-PD plan benefit package
(i.e., Plan 01, Plan 02)
for CY 2017
Non-
bid
related
items
only

105
2017*Note: The dates listed under Part C include MA and MA-PD plans.
The
dates listed under Part D also apply to MA and cost-based plans
offering a Part D benefit.
*Part
C
*Part
D
Cost
MMP
Early June to
Early
September,
2016
CMS completes review and approval of 2017 bid data.
Plans/Part D sponsors submit attestations, contracts, initial
actuarial certifications, and
final actuarial certifications
June 7-10, 2016
Window for submitting first round of crosswalk exception
requests through HPMS
June 10, 2016
Deadline for submission of CY 2017 Supplemental
Formulary
files, Free First Fill file, Partial Gap file,
Excluded Drug file,
Over the Counter (OTC) drug file,
Home Infusion file, and Non-Extended Day Supply file
through HPMS (11:59 a.m. EDT)
June 10, 2016
Deadline for submission of Medicare Advantage Value
Based Insurance Design (VBID) file (Only applicable to
Medicare Advantage Plans that have been preapproved for
Part D VBID benefits) (11:59 a.m. EDT)
June 10, 2016
Deadline for submission of Additional Demonstration Drug
(ADD) file (Medicare-Medicaid Plans Only) (11:59 a.m.
EDT)
June 10, 2016
Deadline for upload of Provider Specific Plan (PSP)
specific networks
June 16, 2016
2016 MA and PDP Audit and Enforcement Conference and
Webcast
Late June, 2016
CMS sends an acknowledgement letter to all MA, MA-PD,
MMP, PDP
and Medicare cost-based plans that are non-
renewing or
reducing their service area
Early July, 2016
2017 Plan Finder pricing test submissions begin
July 1, 2016
Deadline for D-SNPs to upload required State Medicaid
Agency
Contract and Contract Matrix to HPMS
July 1, 2016
Deadline for D-SNPs requesting to be reviewed as Fully
Integrated Dual-Eligible (FIDE) SNPs to submit their FIDE
SNP Matrix to HPMS.
July 5, 2016
Plans’ deadline to submit non-model Low Income Subsidy
(LIS) riders to the appropriate Regional Office for review.
Mid July 2016
Release of CY 2017 FRF Update in advance of the Limited
Formulary Update Window
Mid-Late July,
2016
CY 2017 Limited Formulary Update Window
Late July, 2016
Submission deadline for agent/broker compensation
information
via HPMS
Mid-Late July 2016
Second window for submitting HPMS crosswalk exceptions
Late July / Early
August, 2016
CMS releases the 2017 Part D national average monthly bid
amount, the Medicare Part D base beneficiary premium, the
Part
D regional low-income premium subsidy amounts, the
Medicare
Advantage regional PPO benchmarks, and the de
minimis
amount
Late July / Early
August, 2016
Rebate reallocation period begins after release of the above
bid
amounts

106
2017*Note: The dates listed under Part C include MA and MA-PD plans.
The
dates listed under Part D also apply to MA and cost-based plans
offering a Part D benefit.
*Part
C
*Part
D
Cost
MMP
No Later Than
July
29, 2016
CMS informs currently contracted organizations of its
decision
to not renew a contract for 2017
August 1, 2016
Plans expected to submit model Low Income Subsidy (LIS)
riders in HPMS
August 16, 2016
Deadline for organizations to complete the plan
connectivity data in HPMS to ensure timely approval of
contracts.
August 18-22,
2016
CY 2017 preview of the 2017 Medicare & You plan data in
HPMS prior to printing of the CMS publication (not
applicable
to EGWPs)
August 24-26, 2016
First CY 2017 Medicare Plan Finder (MPF) Preview and
Out-
of-Pocket Cost (OOPC) Preview in HPMS
MPF
only
August 31, 2016
2017 MTM Program Annual Review completed
Late August 2016
Contracting Materials submitted to CMS
End of
August/Early
September 2016
Plan preview periods of Part C & D Star Ratings in HPMS
September 1, 2016
Deadline for submission of detailed operational information
on soft and/or hard formulary-level cumulative morphine
equivalent dose (MED) opioid point of sale (POS) edit(s).
Early September
2016
CMS begins accepting plan correction requests upon
contract
approval
Mid- September
2016
All 2017 contracts fully executed (signed by both parties:
Part
C/Part D Sponsor and CMS)
Mid-September
2016
Release of the non-renewal /service area reduction models
September 6-9,
2016
Second CY 2017Medicare Plan Finder (MPF) Preview and
Out-of-Pocket Cost (OOPC) Preview in HPMS
MPF
only
September 16 -30,
2016
CMS mails the 2017 Medicare & You handbook to
Medicare
beneficiaries
Late September,
2016
D-SNPs that requested review for FIDE SNP determination
notified as to whether they meet required qualifications
September 21,
2016
Deadline for Part D sponsors, cost-based, MA and MA-PD
organizations to request a plan correction to the plan benefit
package (PBP) via HPMS.

107
2017*Note: The dates listed under Part C include MA and MA-PD plans.
The
dates listed under Part D also apply to MA and cost-based plans
offering a Part D benefit.
*Part
C
*Part
D
Cost
MMP
September 30,
2016
The following documents are due to current enrollees by
September 30, 2016:
Standardized Annual Notice of Change/Evidence of
Coverage (ANOC/EOC) for all MA, MA-PD, PDP,
and
cost-based plans (including those not offering Part D and
those that do offer Part D).
Standardized ANOC with the Summary of Benefits for
D-SNPs and MMPs that choose to separate the ANOC
from the EOC.
Abridged or comprehensive formularies
LIS rider
Pharmacy/Provider directories
The multi-language insert should be sent with the
ANOC/EOC
and the SB.
The documents identified above are the only CY 2017
documents
permitted to be sent prior to October 1, 2016
October 1, 2016
Organizations may begin marketing their CY 2017 plan
benefits.
Note: Once an organization begins marketing CY 2017
plans,
the organization must cease marketing CY 2016
plans through
mass media or direct mail marketing (except
for age-in
mailings). Organizations may still provide CY
2016 materials
upon request, conduct one-on-one sales
appointments, and
process enrollment applications
October 1, 2016
Tentative date for 2017 plan and drug benefit data to be
displayed on Medicare Plan Finder on Medicare.gov (not
applicable to EGWPs)
October 2, 2016
The final personalized beneficiary non-renewal notification
letter must be received by PDP, MA plan, MA-PD plan, and
cost-based plan enrollees.
PDPs, MA plans, MA-PD plans, and Medicare cost-based
organizations may not market to beneficiaries of non-
renewing
plans until after October 2, 2016
October 13, 2016
Part C & D Star Ratings go live on medicare.gov on or
around October 13,
2016
October 15, 2016
Part D sponsors must post PA and ST criteria on their
websites
for the 2017 contract year
October 15, 2016
2017 Annual Election Period begins
All organizations/sponsors must hold open enrollment (for
EGWPs, see Chapter 2 of the Medicare Managed Care
Manual,
Section 30.1)

108
2017*Note: The dates listed under Part C include MA and MA-PD plans.
The
dates listed under Part D also apply to MA and cost-based plans
offering a Part D benefit.
*Part
C
*Part
D
Cost
MMP
Mid October,
2016
Release of the online CY 2018 Notice of Intent to Apply for
a
New Contract or a Contract Expansion (MA, MA-PD,
MMP, PDPs,
and “800 series” EGWPs and Direct Contract
EGWPs)
November 4, 2016
Release of CY 2015 MLR Report Upload Functionality in
HPMS
November 14, 2016
Notices of Intent to Apply (NOIA) for CY 2018 due for MA
and MA-PD plans, MMP, PDPs, and “800 series” EGWPs
and Direct
Contract EGWPs.
Early November,
2016
First display of Plan Finder data for sponsors/MA
organizations
that submitted a plan correction request after
bid approval
Late November,
2016
Part C & D display measures data are posted in HPMS for
plan preview
November –
December, 2016
CMS issues “close out” information and instructions to MA
plans, MA-PD plans, MMPs, PDPs, and cost-based plans
that are non-
renewing or reducing service areas
December 1, 2016
Cost-based plans must publish notice of non-renewal, as per
§417.494 of Title 42 of the CFR.
December 2, 2016
Deadline for submission of CY 2015 MLR Reports (11:59
PT)
December 5, 2016
Release of CY 2015 MLR Attestation Module in HPMS
December 7, 2016
End of the Annual Election Period
December 9, 2016
Deadline for submission of CY 2015 MLR Attestations
(11:59 PT)
Mid December,
2016
Part C & D display measures data on cms.gov updated
December 31, 2016
Deadline for MMPs that separated the ANOC from
the
EOC to provide the EOC to enrollees
2017
January 1, 2017
Plan Benefit Period Begins
January 1 –
February 14, 2017
Annual 45-Day Medicare Advantage Disenrollment Period
(MADP)
Early January
2017
Release of CY 2018 MAO/MA-PD/MMP/PDP/SAE/EGWP
applications
Mid-January, 2017
Industry training on CY 2018 applications
Mid-February
2017
Applications due for CY 2018
109
Incomplete and Inaccurate Bid Submissions
Incomplete Submissions
Under Sections 1854(a)(1)(A) and 1860D-11(b) of the Social Security Act, initial bid
submissions for all MA, MA-PD, PDPs and cost-based plans are due the first Monday in June
and shall be in a form and manner specified by the Secretary. Therefore, for CY 2017, the bid
submission deadline is June 6, 2016 at 11:59 PM Pacific Daylight Time.
The following components are required, if applicable, to constitute a complete bid submission:
Plan Benefit Package (PBP) and Bid Pricing Tool (BPT)
Service Area Verification (SAV)
Plan Crosswalk (if applicable)
Formulary Submission (if offering a Part D plan with a formulary)
Formulary Crosswalk (if offering a Part D plan with a formulary)
Substantiation (supporting documentation for bid pricing) including cost-sharing
justification that supports benefit designs which use a coinsurance or copayment amount
for which CMS does not have an established amount (if applicable) for MA plans as
described in the “Part C Cost Sharing Standards” of this Call Letter.
MA, MA-PD, PDP, and cost-based plans are responsible for confirming that complete and
accurate bids are submitted by the June deadline. Consistent with past years, CMS reminds
organizations that all required components of an organization’s bid must be submitted by the
deadline in order for the bid to be considered complete. If any of the required components are
not submitted by the deadline, the bid submission will be considered incomplete and not
accepted by CMS absent extraordinary circumstances. This policy is consistent with previous
years (for example, please refer to the memo “Release of Contract Year (CY) 2016 Bid Upload
Functionality in HPMS,” dated May 8, 2015).
The Health Plan Management System (HPMS) Bid Upload functionality, which is made
available to organizations in May, allows organizations to submit each required bid component
well in advance of the deadline. The Bid Upload functionality includes reporting tools that track
those components that were successfully submitted and those that are still outstanding. CMS
expects organizations to take advantage of these resources and make certain that all components
of their bid are submitted successfully and accurately by the submission deadline.
All organizations are expected to contact CMS about any technical upload or validation errors
well in advance of the bid submission deadline. CMS will not accept late submissions unless
they are the result of a technical issue beyond the organization’s control, in what is expected to
110
be very rare and unique circumstances. All organizations should make sure that appropriate
personnel are available both before and after the bid submission deadline to address any ongoing
bid upload and/or validation issues that might prevent the bid from proceeding to desk review.
Inaccurate Submissions
CMS reminds organizations that it will only approve a Part D bid under 42 CFR §423.272(b) if
the organization offering the plan’s bid complies with all applicable Part D requirements,
including those related to the provision of qualified prescription drug coverage and actuarial
determinations. In addition, all Part C bids under §422.254 (a)(3) must be complete, timely, and
accurate or CMS has the authority to impose sanctions or may choose not to renew the contract.
See also §§ 422.256 and 423.265. Bids that contain inaccurate information and/or fail to meet
established thresholds may, among other things, result in an unnecessary diversion of CMS and
organizations’ time and resources and call into question an organization’s ability and intention to
fully comply with Part C and D requirements.
Examples of bids containing information that is clearly inaccurate under Part D requirements and
established thresholds are:
An MA-PD bid that does not offer required prescription drug coverage throughout its
service area as required under §423.104(f)(2) (see also section 20.4.4 of Chapter 5 of the
Prescription Drug Benefit Manual),
A PDP bid for a non-defined standard plan that does not meet the Part D Benefit
Parameters set forth in the applicable law and defined benefit thresholds specified in this
Call Letter, or
A Part D bid that includes an incorrect PBP-to-formulary crosswalk.
Organizations and sponsors that submit clearly inaccurate bids on June 6, 2016 and organizations
that resubmit bids prior to approval to change or correct items, such as rebate reallocation and
fail to meet Part C and D requirements, and/or established thresholds, will receive a compliance
notice in the form of a letter and/or a corrective action plan. In addition, organizations and
sponsors that submit inaccurate bids may not be allowed to revise their bids to correct
inaccuracies, and the bids may be denied. Organizations and sponsors should engage in sufficient
due diligence to make certain their bids are accurate before submission.
Plan Corrections
As required by 42 CFR §§422.254, 423.265(c)(3) and 423.505(k)(4), submission of the final
actuarial certification serves as documentation that the final bid submission has been verified and
is complete and accurate at the time of submission. A request by an organization or sponsor for
a plan correction indicates the presence of inaccuracies and/or the incompleteness of a bid and
111
calls into question an organization’s or sponsor’s ability to submit correct bids and the validity of
the final actuarial certification and bid attestation.
After bids are approved, CMS will not reopen the submission gates to correct errors identified by
the organization or sponsor until the plan correction window in September. The plan correction
window will be open from early September to late September 2016. The only changes to the
PBP that will be allowed during the plan correction period are those that modify the PBP data to
align with the BPT. No changes to the BPT are permitted during the plan correction period.
In advance of the bid submission deadline, CMS will provide organizations and sponsors the
guidance and tools necessary for a complete and accurate bid submission. These tools will
include a Medicare Plan Finder (MPF) summary table report that will be released in HPMS in
May. Organizations and sponsors can upload their bid multiple times in HPMS prior to bid
submission so that they can confirm that MPF data are being displayed accurately.
Organizations and sponsors are encouraged to use this time prior to the submission deadline to
verify their bid will not require a plan correction. Organizations and sponsors submitting plan
corrections will receive a compliance action and will be suppressed in MPF until the first MPF
update in November. In addition, CMS may issue more severe compliance actions such as
warning letters and corrective action plans to organizations/sponsors that have demonstrated a
consistent pattern of bid submission errors over multiple contract years and/or previously
received a compliance notice for CY 2016.
We received comments expressing concern about organizations and sponsors receiving
compliance actions for simple data input errors. CMS reminds organizations and sponsors that
they should take this opportunity to conduct quality assurance activities prior to bid submission.
Contracting Organizations with Ratings of Fewer Than Three Stars in Three Consecutive
Years – Timeline for Application of Termination Authority
CMS may, under our regulatory authority at 42 C.F.R. §§ 422.510(a)(4)(xi) and
423.509(a)(4)(x), terminate the contracts of organizations that have failed to achieve a rating of
three stars or better on their Part C or Part D performance in three consecutive years. Since CMS
announced through rulemaking in 2012 that we would consider consistently low Star Ratings as
a basis for terminating a Part C or Part D contract, a significant number of organizations have
taken steps to improve the performance of their poor performing contracts. In other instances,
organizations have non-renewed low-rated contracts or consolidated their operations into
different, higher-rated contracts. As a result, the overall quality of Medicare plan options
available to beneficiaries continues to improve.
In the CY 2016 final Call Letter, CMS announced that contracts that earned their third
consecutive Part C or Part D rating of less than three stars with the release of the 2016 ratings in
the fall of 2015 would receive non-renewal notices from CMS in February 2016 with an

112
effective date of December 31, 2016, at 11:59 pm EST. We also announced that we would not
calculate or publish 2017 Star Ratings associated with the non-renewed contracts.
CMS advises MAOs and PDP sponsors that we will conduct future star rating-based terminations
according to a similar timeline. That is, CMS will issue contract non-renewal notices in
February of each year, with an effective date of December 31st of the same year, to all contracts
that meet the criteria for a Star Rating-based termination with the release of the set of Star
Ratings issued in October of the preceding year. In March, following the issuance of the non-
renewal notices, beneficiaries enrolled in plans offered under the non-renewed contracts will
receive notices advising them that they will need to choose a new plan during the next annual
election period to continue their Part C and Part D plan enrollment without interruption during
the following benefit year. CMS may stay the issuance of non-renewal and beneficiary notices
in instances where the organization that holds the contract eligible for non-renewal is prepared to
complete a consolidation of that contract into a higher-rated contract during the bid cycle for the
upcoming plan year. In that situation, CMS will allow the organization to complete the contract
consolidation process during the bid submission and review cycle, but we will retain the right to
issue the notices at the conclusion of the review cycle should the organization fail to complete
the consolidation process. Finally, CMS will not calculate or publish Star Ratings for non-
renewed contracts during the year in which CMS issues the non-renewal notice, so terminated
contracts should not expect there to be an opportunity for CMS to reverse its determination based
on the contract’s improved Star Rating performance during its last year of operation.
Enhancements to the 2017 Star Ratings and Beyond
One of CMS’ most important strategic goals is to improve the quality of care and health status of
Medicare beneficiaries. For the 2017 Star Ratings, CMS continues to enhance the Star Ratings
methodology to further align with our policy goals. Our priorities include enhancing the
measures and methodology to reflect the true performance of organizations and sponsors,
ensuring stability due to the link to payment, and providing advance notice of future proposals.
In this document, we describe enhancements for the 2017 Star Ratings and beyond. CMS is not
adding any new measures for 2017 Star Ratings. Except as noted below, the methodology will
remain the same as the 2016 Star Ratings.
For reference, the list of measures and a description of the methodology for the 2016 Star
Ratings are included in the Technical Notes available on the CMS webpage:
https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovGenIn/
PerformanceData.html.
The cut points to determine star assignments for all measures and case-mix coefficients for the
Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey and Health
Outcomes Survey (HOS) will be updated for 2017 using the most current data available.
113
As announced in previous years, we will review data quality across all measures, variation
among organizations and sponsors, and measures’ accuracy and validity before making a final
determination about inclusion of measures in the Star Ratings.
We appreciate the feedback we received on the 2017 Request for Comments and the draft Call
Letter. In addition to noting some of the more significant comments below, summaries of
comments to the draft Call Letter and responses are included in Appendix 4 to this final Call
Letter.
Changes to Measures for 2017
CMS’ general policies regarding specification changes to Star Ratings measures include the
following:
If a specification change to an existing measure is announced in advance of the
measurement period, the measure remains in the Star Ratings, it will not be moved to the
display page.
If the change announced during the measurement period significantly expands the
denominator or population covered by the measure, the measure is moved to the display
page for at least one year.
If the change announced during the measurement period does not significantly impact the
numerator or denominator of the measure, the measure will continue to be included in the
Star Ratings (e.g., when during the measurement period additional codes are added that
would increase the number of numerator hits for a measure).
The methodology for the following measures is being modified:
Improvement measures (Part C & D). While the methodology for incorporating measures
into the calculation of the two improvement measures (one each for Part C and D) remains
the same as in prior years, we have updated the measures used for each improvement
measure to account for measures with at least two years of data. Refer to Appendix 3 for
updates to the measures to be used to calculate the 2017 improvement measures. If a
contract’s CAHPS measure score moved to very low reliability with the exclusion of
enrollees with less than 6 months of continuous enrollment for the 2015 survey
administration, then the 2014 CAHPS measure score (used in 2015 Star Ratings) will be
used instead as the baseline for the 2017 improvement calculation for that measure. If the
contract has missing 2015 CAHPS data due to very low reliability, we would use the 2014
CAHPS data only if there is a significant improvement from 2014 to 2016. This policy
should affect very few contracts but will hold contracts harmless from missing data.
Appeals Timeliness/Reviewing Appeals Decisions measures (Part C) and Appeals
Upheld measure (Part D). Currently, these measures include cases that are reopened and
114
decided by April 1 of the following contract year. In some instances, appeals filed in the 4
th
quarter of the year and then subsequently reopened may not be determined by the IRE by
April 1. We will modify these measure specifications so that if a reopening occurs and is
decided prior to May 1, 2016, the reopened decision will be used. Reopenings decided on
or after May 1, 2016 will not be reflected in these data, and the original decision result will
be used.
Transition from ICD-9 to ICD-10 (Part C & D). The measure stewards, such as the
National Committee for Quality Assurance (NCQA) and the Pharmacy Quality Alliance
(PQA), have reviewed their measure specifications with diagnosis-related requirements to
transition from ICD-9 to ICD-10.
NCQA has incorporated the ICD-10 codes in the 2016 Healthcare Effectiveness Data and
Information Set (HEDIS). During the period that spans the use of both ICD-9 and ICD-10
codes due to look-back periods for some measures, both ICD-9 and ICD-10 codes will be
used.
Appeals Upheld measure (Part D). This measure shows how often the IRE decided the
drug plan’s denial of an appeal was appropriate. For the 2016 Star Rating Upheld measure,
we excluded appeal cases for beneficiaries enrolled in hospice at any point during 2014. As
noted in the 2016 Call Letter, this exclusion was only necessary for the 2016 measure as it
was based on 2014 data that may have been affected by hospice policy changes in 2014.
CMS hospice policy has not changed since 2014, so it is no longer necessary to exclude
hospice appeal cases. This exclusion will not be continued for the 2017 Star Rating Appeals
Upheld measure.
Medication Therapy Management (MTM) Program Completion Rate for
Comprehensive Medication Reviews (CMR) measure (Part D). We will add a detailed
file during each HPMS plan preview period to list each contract’s underlying denominator,
numerator, and Data Validation score since exclusions are applied to the plan-reported
MTM data.
The CMR rate measure is an initial measure of the delivery of MTM services, and we
continue to look forward to the development and endorsement of outcomes-based MTM
measures as potential companion measures to the current MTM Star Rating. More
information is provided later in this section about the Center for Medicare and Medicaid
Innovation’s Part D Enhanced MTM Model. Lastly, we will be implementing additional
data integrity checks (discussed later in this section) to safeguard against inappropriate
attempts to bias the data used for this measure.
Medication Adherence for Hypertension (RAS Antagonists) (Part D Star Rating).
Based on PQA specification change, the measure will exclude from the denominator those
115
patients with one or more claims for sacubitril/valsartan. This exclusion will be applied for
the 2017 Star Ratings.
Removal of Measures from Star Ratings
1. Improving Bladder Control (Part C). This measure, collected through the Health
Outcomes Survey (HOS), assesses the percentage of beneficiaries with urine leakage who
discussed their problem with their provider and received treatment for the issue. NCQA made
three changes to this measure. First, NCQA changed the denominator of both indicators to
include all adults with urinary incontinence, as opposed to limiting the denominator to those
who consider urinary incontinence to be a problem. This action will remove a potential bias
towards only sampling patients who were treated unsuccessfully. Second, NCQA changed
the treatment indicator to assess whether treatment was discussed, as opposed to it being
received. This will change the measure focus from receiving potentially inappropriate
treatments, which often have adverse side effects, to shared decision making between the
patient and provider about the appropriateness of treatment. Third, NCQA added an outcome
indicator to assess the degree to which urinary incontinence impacts beneficiaries’ quality of
life. Data from this outcome indicator will be analyzed further before any new measure (or
measure specification change) is proposed as part of the Star Ratings. CMS will request
further input on this measure in the 2018 Request for Comments.
These changes required revising the underlying survey questions in HOS. The revised
questions were first collected in 2015. As a result of these changes, this measure will not be
reported in the 2017 Star Ratings. The revised measure will be reported on the 2017 display
page. The 2016 display measure uses data from the old questions.
2. High Risk Medication (Part D). The High Risk Medication (HRM) measure calculates the
percent of Medicare Part D beneficiaries 65 and older who received two or more prescription
fills for the same HRM drug with a high risk of serious side effects in the elderly. The
measure is endorsed by the PQA and National Quality Forum (NQF), and the HRM rate is
calculated using the PQA specifications and medication list based on American Geriatrics
Society (AGS) recommendations. The AGS recently released the 2015 update of the Beers
Criteria, which serve as the foundation for the AGS recommendations.
In the draft 2017 Call Letter, CMS proposed to remove the HRM measure from the Star
Ratings and move it to the display measures for 2017. This proposal was based on a number
of factors. While the AGS states that the criteria may be used as both an educational tool and
quality measure, it also states that the intent is not to apply the criteria in a punitive manner
(i.e., penalizing prescribers that are trying to do the best for their patients). Specifically, the
addition of a drug to the HRM list is not a contraindication to use, rather an encouragement
to avoid use in the senior population without consideration of risks and benefits based on
individual patient characteristics. This is a very difficult decisional balance to evaluate in a
116
plan that does not have access to full clinical information. As the measure can be calculated
only by using prescription drug event (PDE) data, medications cannot be included on the
HRM List that have risks conditional on clinical factors that cannot be measured using PDE
data alone. As a result, some “Avoid” medications are included in the measure, while others
are not. This may create unintended consequences including the inappropriate
encouragement of certain non-HRM medications, which may not be the best choice for an
individual beneficiary’s clinical circumstance.
Based on feedback to the draft 2017 Call Letter (see Appendix 4 for summary of Star Ratings
comments and responses) and concerns that a change was being made after the measurement
period in which efforts by Part D sponsors were invested, the HRM measure will remain in
the Star Ratings for 2017 (based on 2015 data) and move to the display page for 2018 (based
on 2016 data). We will continue to provide HRM measure reports to Part D sponsors on a
monthly basis through the Patient Safety Analysis website, and we will continue to identify
outliers.
The PQA recently made two changes to the HRM measure specifications. First, any patient
with a hospice indicator at any point during the measurement year will be excluded from the
denominator calculation. We will implement this change immediately for the 2017 Star
Rating measure based on 2015 data. Second, the PQA revised the criteria to calculate the
average dose for doxepin, reserpine, and digoxin. We will implement this change for the
2018 measure based on 2016 data. Any additional updates endorsed by the PQA by the 2017
formulary and bid deadlines in May and June 2016 may be considered for adoption in the
2019 measures (using 2017 data).
Our initial analysis of HRM found that after controlling for contract effects and dual eligible
or low income subsidy status, there is a significant association between dual eligible/low
income status and HRM use. This association remains after further controlling for age, sex,
and race/ethnicity. However, because it is under direct provider control and should not be
affected by non-clinical beneficiary characteristics, the HRM measure was not one of the
measures adjusted for socio-economic status (SES) (discussed later in this Call Letter). We
recommend that the measure developers further review this measure to better understand the
associations.
Avoiding potentially inappropriate medications in older adults remains important for quality
of care for Medicare beneficiaries. HRM will be reconsidered for the Star Ratings again in
the future once analyses and specification changes, if any, are completed by the PQA. Any
changes will be proposed or implemented with sufficient lead time.

117
Data Integrity
It is essential that the data used for CMS’ Star Ratings are accurate and reliable. CMS’ policy is
to reduce a contract’s measure rating to 1 star if it is determined that biased or erroneous data
have been submitted. This would include cases where CMS finds mishandling of data,
inappropriate processing, or implementation of incorrect practices by the organization/sponsor
have resulted in biased or erroneous data. Examples would include, but are not limited to: a
contract’s failure to adhere to HEDIS, HOS, or CAHPS reporting requirements; a contract’s
failure to adhere to Plan Finder or PDE data requirements; a contract’s errors in processing
coverage determinations/exceptions or organization determinations found through program
audits or other reviews; compliance actions due to errors in operational areas that would directly
impact the data reported or processed for specific measures; or a contract’s failure to pass Part C
and D Reporting Requirements Data Validation related to organization/sponsor-reported data for
specific measures. Sponsors should refer to specific guidance and technical instructions related
to requirements in each of these areas. For example, information about HEDIS measures and
technical specifications are posted on
http://www.ncqa.org/HEDISQualityMeasurement/HEDISMeasures.aspx. Information about
Data Validation of Reporting Requirements data is posted on
https://www.cms.gov/Medicare/Prescription-Drug-
Coverage/PrescriptionDrugCovContra/PartCDDataValidation.html.
CMS has taken several steps in the past years to protect the integrity of the data; however, we
continue to identify new vulnerabilities where inaccurate or biased data could exist. We also
must safeguard against the Star Ratings Program creating perverse incentives for sponsors. CMS
is piloting program audit protocols in 2016, including Part D sponsors’ MTM programs
(discussed later in the Call Letter). Findings identified during pilots of these new MTM audit
protocols would not be applied to Star Ratings. Once the protocols are finalized, we would
review and apply any relevant MTM program audit findings that could demonstrate systemic
failures by sponsors that resulted in biased MTM data, outside of the Data Validation (DV)
results. CMS is concerned about sponsor activities that may not be detected by DV standards,
such as attempts to restrict eligibility from their approved MTM programs, encouraging
beneficiaries to opt-out of MTM programs within the first 60-days, or reporting CMRs that do
not meet CMS’ definition per guidance.
DV standards primarily focus on compliance with CMS’ reporting requirements, and CMS
considers failing to meet these standards to represent systemic issues that would result in biased
data. DV element-level failures can indicate that incomplete or inaccurate data were reported for
use in Star Ratings. It is possible for a sponsor to receive a passing score for a section, but have
specific element-level failures that directly impact the validity of their measure. For example, if
the DV found a sponsor’s errors in the numbers of beneficiaries enrolled in the MTM or
receiving a CMR, regardless of the overall MTM DV score, CMS would still have concerns
about the accuracy of the sponsor’s CMR numerator and denominator.

118
CMS may perform additional audits or reviews to ensure the validity of data for specific
contracts. Without rigorous validation of Star Ratings data, there is risk that CMS will reward
contracts with falsely high ratings.
Impact of Socio-economic and Disability Status on Star Ratings
A key goal of the MA and Part D programs is to achieve greater value and quality for all
beneficiaries; therefore, an important corollary is that we do not distort quality signals in our
measures or mask true differences in quality of care. CMS continuously reviews the Star Ratings
methodology to improve the process, incentivize plans, and provide information that is a true
reflection of the performance and experience of the enrollees. The policies implemented must
result in high quality of care and improved health outcomes for all of our beneficiaries, while
acknowledging the unique challenges of serving traditionally underserved subsets of the
population.
A number of MA organizations and PDP sponsors believe that enrollment of a high percentage
of dual eligible (DE) enrollees and/or enrollees who receive a low income subsidy (LIS) limits
their plans’ ability to achieve high MA or Part D Star Ratings. CMS has responded to the
concern from our stakeholders by comprehensively gathering information to determine if the Star
Ratings are sensitive to the LIS/DE and disability status of a contract’s enrollees. If adjustments
are to be made to address this issue, they must be data driven. For example, if a disparity is due
to challenges in serving disabled beneficiaries, rather than in serving LIS/DE beneficiaries, then
the adjustment should clearly focus on the disability status of beneficiaries. Similarly, unless our
methods are transparent and open to input from a breadth of sources, MA organizations and Part D
sponsors will not be able to easily translate our findings into actionable quality improvement steps.
With support from our contractors, CMS has undertaken research to provide scientific evidence
as to whether MA organizations or Part D sponsors that enroll a disproportionate number of
vulnerable beneficiaries are systematically disadvantaged by the current Star Ratings. In 2014,
we issued a Request for Information to gather information directly from organizations to
supplement the data that CMS collects, as we believe that plans and sponsors are uniquely
positioned to provide both qualitative and quantitative information that is not available from
other sources. In February and September 2015, we released details on the findings of our
research.
8
We have also reviewed reports about the impact of socio-economic status (SES) on
quality ratings, such as the report published by the National Quality Forum (NQF) posted at
www.qualityforum.org/risk_adjustment_ses.aspx and both the Medicare Payment Advisory
Commission’s (MedPAC) Report to the Congress: Medicare Payment Policy posted at
http://www.medpac.gov/documents/reports/mar2015_entirereport_revised.pdf and their recent
8
The February release can be found at https://www.cms.gov/medicare/prescription-drug-coverage/prescriptiondrugcovgenin/
performancedata.html.
The September release can be found at https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovGenIn/
Downloads/Research-on-the-Impact-of-Socioeconomic-Status-on-Star-Ratingsv1-09082015.pdf.

119
presentation released on September 10
th
entitled Factors Affecting Variation in Medicare
Advantage Plan Star Ratings posted at http://www.medpac.gov/documents/september-2015-
meeting-presentation-factors-affecting-variation-in-medicare-advantage-plan-star-ratings.pdf.
The Improving Medicare Post-Acute Care Transformation Act of 2014 (IMPACT Act, P.L. 113-
185) instructs the Office of the Assistant Secretary for Planning and Evaluation (ASPE) to
conduct a study that examines the effect of individuals’ SES on quality measures, resource use,
and other measures for individuals under the Medicare program and report its findings to
Congress by October 2016. In addition, ASPE will issue a report to Congress by October 2019
on the impact of SES on quality and resource use in Medicare using measures (e.g., education
and health literacy) from other data sources. Because ASPE’s research agenda aligns closely
with our goals, we will continue to work collaboratively with ASPE and other governmental
agencies to broaden and expand the focus of the issue.
CMS has also engaged NCQA and the PQA to examine their measure specifications used in the
Star Ratings Program to determine if re-specification is warranted. The majority of measures
used for the Star Ratings Program are consensus-based. Measure specifications can be changed
only by the measure steward (the owner and developer of the measure). Thus, measure scores
cannot be adjusted for differences in enrollee case-mix unless required by the measure
specification. Measure re-specification is a multi-year process. For example, NCQA has a
standard process for reviewing any measure and determining whether a measure requires re-
specification. NCQA’s re-evaluation process is designed to ensure any resulting measure
updates abide by desirable attributes of relevance, scientific soundness, and feasibility.
Relevance describes the extent to which the measure captures information important to different
groups, e.g., consumers, purchasers, policymakers. To determine relevance, NCQA assesses
issues such as health importance, financial importance, and potential for improvement among
entities being measured. Scientific soundness captures the extent to which the measure adheres
to clinical evidence and whether the measure is valid, reliable, and precise. Feasibility captures
the extent to which a measure can be collected at reasonable cost and without undue burden. To
determine feasibility, NCQA also assesses whether a measure is precisely specified and can be
audited. The overall process for assessing the value of re-specification emphasizes multi-
stakeholder input, use of evidence-based guidelines and data, and wide public input.
CMS Research
As stated in the 2016 final Call Letter, CMS believed additional research into the nature of the
differential performance on a subset of measures was necessary before any interim or permanent
changes in the Star Ratings measurements could be developed and implemented. Of the 32
measures included in Star Ratings for Part C and 15 measures for Part D, 8 measures for Part C
and 2 measures for Part D were already case-mix adjusted in some way. CMS further excluded
measures that should not be affected by the enrollee’s SES or disability status. These exclusions
for example include the HRM measures (for reasons described in an earlier section) and
complaints measures. That is, a measure was excluded from analysis if the measure was already
120
case-mix adjusted for SES (i.e., CAHPS and HOS measures), if the focus of the measurement
was not a beneficiary-level issue but rather a plan- or provider-level issue (e.g., appeals, call
center, Part D price accuracy, HRM), if the measure was scheduled to be retired or revised, or if
the measure was applicable to only Special Needs Plans (SNPs) (i.e., SNP Care Management,
Care for Older Adults measures). These exclusions resulted in a remainder of 16 measures.
The 16 clinical quality measures that comprised the subset of the Star Ratings measures
examined included: adult BMI assessment, rheumatoid arthritis management, breast cancer
screening, controlling blood pressure, diabetes care – blood sugar controlled, diabetes care – eye
exam, diabetes care – kidney disease monitoring, colorectal cancer screening, osteoporosis
management in women who had a fracture, plan all-cause readmissions, annual flu vaccine,
monitoring physical activity, reducing the risk of falling, medication adherence for diabetes
medications, medication adherence for hypertension, and medication adherence for cholesterol.
After the publication of the 2016 Final Call Letter, CMS further examined LIS/DE differences
(“effects”) and their magnitude. Due to the considerable overlap between LIS/DE beneficiaries
and disabled beneficiaries, the research was expanded to consider the possible role of disability
status. The research considered the association between the performance on Star Ratings
measures and enrollment of LIS/DE/disabled beneficiaries, and the variability across contracts of
differences in performance on each measure to gain a better understanding of LIS/DE differences
revealed in the preliminary research.
The methodology employed permitted the estimation of within-contract differences associated
with LIS/DE and/or disability. Within-contract differences are differences that may exist
between subgroups of enrollees in the same contract (e.g., if LIS/DE enrollees within a contract
have a different mean or average performance on a measure than non-LIS/DE enrollees in the
same contract). These differences may be favorable or unfavorable for LIS/DE and/or disabled
beneficiaries. Between-contract differences in performance associated with LIS/DE and/or
disability status (“between-contract LIS/DE and/or disability disparities”) are the possible
additional differences in performance between contracts associated with the contract’s proportion
of LIS/DE and disabled enrollees that remain after accounting for within-contract disparities by
LIS/DE and disability status. If LIS/DE and/or disabled beneficiaries are more or less likely than
other beneficiaries to be enrolled in lower-quality contracts, then between-contract disparities
may represent true differences between contracts in quality. Because of this possibility,
between-contract disparities may not be appropriate for adjustment due to the risk of masking
true differences in quality. Adjusting for within-contract disparities is an approach aligned with
the consensus reflected in the NQF report on sociodemographic adjustment, which states that,
“…only the within-unit effects are adjusted for in a risk adjustment procedure because these are
the ones that are related specifically to patient characteristics rather than differences across
units” (National Quality Forum, 2014). Our research focused on measuring within-contract
differences in performance for LIS/DE and/or disabled compared to non-LIS/DE and non-
disabled beneficiaries.

121
Our additional research findings were consistent with the preliminary results shared in the 2016
Final Call Letter. The research to date has provided scientific evidence that there exists a within-
contract LIS/DE and disability effect for a subset of the Star Ratings measures. The size of the
effect differs across measures and is not exclusively negative.
CMS is firmly committed to building the foundation for a long-term solution that appropriately
addresses the issue at hand and aligns with our policy goals. Any policy response must delineate
the two distinct aspects of the LIS/DE and/or disability issue - quality and payment. The Star
Ratings Program focuses on accurately measuring the quality of care provided, so any response
must focus on enhancing the ability to measure actual quality differences among contracts. To
address the LIS/DE and disability issue we must accurately address any sensitivity of the ratings
to the composition of the beneficiaries enrolled in a contract at the basic building block of the
rating system, the measure. CMS has encouraged the measure stewards to examine our findings
and undertake an independent evaluation of the measures’ specifications to determine if measure
re-specification is warranted. Additionally, the payment response focuses on payment accuracy
for beneficiaries with different dual statuses, differentiated by aged or disabled status, by
improving the predictive performance of the CMS-HCC risk-adjustment model to take into
account the unique cost patterns of each of these subgroups of beneficiaries. CMS proposed
revisions to the CMS-HCC risk adjustment models for Payment Year 2017 elsewhere in the
Advance Notice. Information about the payment methodology for 2017 can be found in the CY
2017 Medicare Advantage Capitation Rates and Medicare Advantage and Part D Payment
Policies.
Interim Analytical Adjustments
Background: While the measure stewards undertake a comprehensive review of their measures
used in the Star Ratings Program and ASPE continues its work under the IMPACT Act, CMS
explored interim analytical adjustments to address the LIS/DE and disability effect in the near
term. We recognize that the interim response needs to be both transparent and feasible to
implement pending any changes to measure specifications that may be made by the measure
stewards. In addition, the integrity of the Star Ratings and the core of its methodology must be
maintained. Further, the adjustment must not result in unnecessary complexity and burden to
plans and sponsors. CMS sought to develop methods to afford plans and sponsors the time
needed to validate their data and not impinge on the time allotted for the plan preview period.
Plans must feel confident in their ability to understand the methodology and reproduce their
overall and summary ratings.
As noted in the “Request for Comments: Enhancements to the Star Ratings for 2017 and
Beyond” released on November 12, 2015
9
, CMS in concert with ASPE developed two options
9
The Request for Comment can be found at: https://www.cms.gov/Medicare/Prescription-Drug-Coverage/
PrescriptionDrugCovGenIn/Downloads/2017-Star-Ratings-Request-for-Comments.pdf

122
for interim analytical adjustments to address the LIS/DE and disability effect: (1) a Categorical
Adjustment Index (CAI) and (2) Indirect Standardization (IS). The proposed methods were
explained more fully during the User Call on December 3, 2015.
10
The proposals align with the
goals of making adjustments that reflect the actual magnitude of the differences observed in the
data, providing valid quality ratings to facilitate consumer choice, and providing incentives for
MA and Part D quality improvement. The Categorical Adjustment Index (CAI) is a factor that
would be added to or subtracted from a contract’s overall and/or summary Star Rating to adjust
for the average within-contract disparity; the adjustment factor varies by a contract’s proportion
of LIS/DE and disabled status beneficiaries. The CAI approximates the effect of case-mix
adjustment of contract performance scores for DE/LIS and disabled status. MA contracts would
have up to three adjustments – one for the overall Star Rating and one for each of the summary
ratings (Part C and Part D). PDPs would have one adjustment for the Part D summary rating.
As described in the Request for Comments, Indirect Standardization (IS), the alternative proposal
for adjustment, would have been applied to the same subset of the individual measures that are
adjusted for the determination of the CAI. The focus of the adjustment is the within-contract
LIS/DE and/or disability status difference in the measure scores while allowing for the existence
of true differences in quality by contract. The standardization would employ the current year’s
measure scores.
The overall reaction to the proposed analytical adjustments presented in “The Request for
Comments” was mixed. There were a limited number of comments addressing the measure set
for adjustment. The comments related to the measure set ranged from a general agreement to the
subset of 7 measures selected, to expansion of the adjusted measure set, to the 16 measures
researched by CMS to the inclusion of all measure used in the Star Ratings Program regardless
of whether they were already adjusted or not. Many respondents did not express a preference for
either proposed interim analytical adjustment approach. Of those who did provide a preference,
the majority preferred CAI instead of IS, citing its similarity to CAHPS, greater transparency,
ease of understanding, the ability to have the CAI factors in advance of the plan preview, and
more flexibility and accuracy of the method. Many commenters expressed concern about the
large volume of data needing validation if the IS method were implemented and its impact on the
plan preview period. Many commenters urged CMS to provide simulations such that contracts
could have a better understanding of the impact on their ratings.
After careful review and consideration of the “Request for Comments,” CMS included the CAI
adjustment in the draft 2017 Call Letter for further consideration. In addition, using the 2016
Star Ratings data, CMS simulated the change in the distribution of ratings to the overall and Part
C and D summary Star Ratings for MA organizations and Part D summary Star Rating for PDP
contracts after the application of both proposed interim analytical adjustments and released
10
The User Call slides can be found at: https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovGenIn/
Downloads/Potential-Options-for-SES-and-Disability-Adjustments_120315.pdf.

123
summaries of the results of the simulations in the draft Call Letter.
11
The simulations results did
not include contracts that exclusively serve Puerto Rico. The simulation results for Puerto Rico
and a discussion of the LIS Indicator were presented in a separate section. Contracts were able
to review their simulation results under each of the proposed analytical adjustments in HPMS
beginning on February 22, 2016.
For the simulations, the measures selected for adjustment were determined by our research and
included the measures that had the greatest differences in outcomes between LIS/DE and/or
disability beneficiaries and non-LIS/DE and/or non-disabled beneficiaries within the same
contracts. The primary basis for the selection of the subset of measures for adjustment was the
research conducted using the 2012 measurement period that examined the variability of the
within-contract differences for measures that had a median absolute difference between LIS/DE
and non-LIS/DE beneficiaries of 5% or more and/or no contracts that had the LIS/DE subgroup
outperform the non-LIS/DE subgroup within a contract. For PDPs, the research showed that the
median absolute difference in performance between LIS/DE and non-LIS/DE enrollees was
greater than 5% for Medication Adherence for Hypertension. It was slightly smaller for MA-
PDs, but to apply consistent adjustments across MA-PDs and PDPs it is included for adjustment
for both delivery systems. Appendix 5 provides the summary statistics of the minimum, median,
and maximum for the within-contract variation for the LIS/DE differences revealed in our
research per measure for MA and PDP contracts. The measures selected for adjustment included
the following six Part C measures for MA (MA-only, MA-PD) and 1876 contracts: Breast
Cancer Screening, Colorectal Cancer Screening, Diabetes Care – Blood Sugar Controlled,
Osteoporosis Management in Women who had a Fracture, Rheumatoid Arthritis Management,
and Reducing the Risk of Falling. In addition, Medication Adherence for Hypertension (RAS
antagonists) was adjusted for MA-PDs and PDPs.
The simulations resulted in less movement, in the overall and summary Star Ratings, with the
application of the CAI compared to IS. The CAI values were modest negative adjustments for
contracts that had low percentages of dual/disabled enrollees and larger positive adjustments for
contracts with higher percentages of LIS/DE and disabled enrollees. By design, the values of the
CAI are monotonic and thus, contracts with a larger percentage of vulnerable beneficiaries would
realize more positive adjustments. The values of the CAI values thus align with the findings of
our research and reflect the actual magnitude of the differences observed in our research. The
changes in the Star Ratings that resulted due to the application of IS were not as consistent with
the research findings. The application of IS affected some contracts in an unexpected direction,
such that some contracts with high LIS/DE and disabled proportions received a negative
adjustment, while some contracts with low enrollments of vulnerable beneficiaries experienced
gains to their Star Ratings. The simulations confirmed that, based on the 2016 Star Ratings, the
analytical adjustment using CAI tends to increase the ratings for contracts with higher
11
The draft Call Letter which includes the simulations is posted at https://www.cms.gov/Medicare/Health-Plans/
MedicareAdvtgSpecRateStats/Announcements-and-Documents-Items/2017Advance.html.

124
proportions of LIS/DE and disabled beneficiaries, while the IS analytical adjustment did not
seem to do so as specifically and to the same degree as did the CAI.
CMS appreciates the views and opinions contained within the responses to the draft Call Letter.
We have listened carefully to the concerns of our multiple stakeholders in both the development
and decision for the response to these concerns for the final Call Letter. We hold steadfast to our
goal of providing the highest quality of care to our beneficiaries and incentivizing plans to do so.
We are grateful for the positive feedback that commended our examination of the issue at-hand.
Many commenters applauded CMS for the transparency in our processes and the multi-pronged
approach to developing a response that both aligned with our goals and reflected the magnitude
of the issue revealed in our research.
There was overwhelming support in response to the draft Call Letter for moving forward with
implementing the CAI analytical adjustment for the 2017 Star Ratings. While some commenters
expressed hesitation to implementing an interim solution, CMS believes that it is a necessary
first step for building the foundation for a long-term solution. CMS will implement the CAI
beginning with the 2017 Star Ratings. We will continue to work closely with our HHS partners
and look forward to our continued collaboration with ASPE as they too are examining the same
issue on a broader scale. The Star Ratings measure stewards will continue to examine their
measures for possible re-specification and CMS will continue to support and encourage them to
do so.
While the measure stewards continue their examination of the measure specification and ASPE
completes their studies and formulates recommendations, the CAI will be considered annually as
an interim adjustment.
12
The CAI methodology is such that it does not impact the core of the
Star Ratings methodology and thus, it affords CMS the ability to be nimble and reactive to
changes in the landscape in a timely fashion. The CAI methodology is flexible and allows
modification. Annually, CMS will request comments as to the subset of measures to be included
for adjustment. We welcome comments throughout the year on all aspects of the Star Ratings
Program and encourage our multiple stakeholders to provide suggestions for enhancement to the
Star Ratings Program. As stated in the draft 2017 Call Letter, the rating year’s CAI values will
be published in the final Call Letter each year during the period while the interim solution is
applied. The CAI values will be determined using the previous rating year’s measurement
period which allows the release of the values well in advance of the first preview period. In
addition, the Medicare Part C & D Star Rating Technical Notes
13
(Technical Notes) will provide
the CAI values along with the details of the methodology. Since 2017 is the initial year of
implementation, the details of the methodology are included in this 2017 final Call Letter.
12
If ASPE makes recommendations that modify the Star Ratings methodology, CMS will provide contracts with simulations for
review and comment.
13
The Technical Notes are posted at http://go.cms.gov/partcanddstarratings.
125
Categorical Adjustment Index Methodology
This section provides the details of the methodology that was employed to determine the 2017
CAI values for the overall and summary Star Ratings.
As discussed previously, the CAI is a factor that would be added to or subtracted from a
contract’s overall and/or summary Star Rating to adjust for the average within-contract disparity.
Contracts are categorized based on their percentages of LIS/DE and disabled beneficiaries, and
the CAI value will be the same for all contracts within each final adjustment category. The CAI
values will be determined using the prior year’s Star Rating data. For the 2017 Star Ratings, the
CAI values were based on the reportable values for the 2016 Star Ratings year using data from
all contracts that meet reporting requirements. The CAI calculation for the PDPs is performed
separately and employs the PDP specific cut points. The percentages of LIS/DE and disabled per
contract will be determined using Medicare enrollment data from CY 2015. If a beneficiary was
designated as a full or partial dual (Medicare and Medicaid) at any time during 2015 and/or if
during the application process, the beneficiary was deemed LIS eligible, the individual will be
categorized as LIS/DE. Disability status will be based on the original reason for entitlement for
Medicare. The percentages for LIS/DE and disability percentages will be provided to contracts
during plan preview. (This year, LIS/DE and disability percentages were provided with the
simulation results.)
The CAI values will be available and released in the final Call Letter each year while the interim
solution is applied. The values for the index will be presented and applied using 6 decimal
places. The CAI methodology, the list of the measures adjusted for the determination of the CAI
values, and all applicable rounding rules will be detailed and available in the Technical Notes for
the applicable year.
MA plans will have up to three mutually exclusive and independent adjustments – one for the
overall Star Rating and one for each of the summary ratings (Part C and Part D). PDPs will have
one adjustment for the Part D summary rating.
For 2017, the measures selected for adjustment are: Breast Cancer Screening, Colorectal Cancer
Screening, Diabetes Care – Blood Sugar Controlled, Osteoporosis Management in Women who
had a Fracture, Rheumatoid Arthritis Management, and Reducing the Risk of Falling. In
addition, Medication Adherence for Hypertension (RAS antagonists) would be adjusted for MA-
PDs and PDPs.
The adjusted measure scores used in the calculation of the CAI values will be determined from
regression models of beneficiary-level measure scores that adjust for the average within-contract
difference in measure scores by LIS/DE and disability status for MA or PDP contracts, without
masking potential differences in quality across contracts. The regression models used for
adjustment quantify the relationship between the measure score of interest and LIS/DE and
disability status, controlling for between-contract differences using contract fixed effects.
126
The approach employed to determine the adjusted measure scores approximates case-mix
adjustment in a patient-level, logistic regression model with contract fixed effects and
beneficiary-level indicators of LIS/DE and disability status, similar to the approach currently
used to adjust CAHPS patient experience measures. However, unlike CAHPS case-mix
adjustment, the only adjusters are LIS/DE and disability status. Measure scores are adjusted
first, and then the adjusted measure score is converted to a measure-level Star Rating using the
measure thresholds for the given Star Ratings year. The purpose of the adjusted measure scores
is to calculate the values of the CAI and not for contract-level information. Therefore, the
adjusted measures scores will not be displayed nor shared with contracts; only measure scores
that are calculated following the measure specification are displayed for public use. (As noted
previously, only the measure steward has the authority to change a measure specification.) The
unadjusted measure score cut points are employed in the conversion from a score to a star and
are done in order to compare changes in measure stars using adjusted measure scores relative to
unadjusted measure scores. The use of the unadjusted measure thresholds for the conversion is
justified given the CAI is applied to the unadjusted overall and summary Star Ratings. Since the
CAI will be added to or subtracted from the unadjusted overall Star Rating, the reward factor
(formerly known as the I-factor) would be based on unadjusted scores. The Part C and D
Improvement measures will use unadjusted measure scores for both years being compared.
Once all measures selected for adjustment have been converted to measure-level star ratings, the
CAI values are determined using the following methodology:
(1) Contracts are divided into an initial set of categories based on some combination of a
contract’s percentages of enrolled LIS/DE and disabled beneficiaries. As done in the simulations,
for the overall Star Rating and the Part C summary Star Rating, 50 initial categories are formed
corresponding to the 10 deciles of LIS/DE and the 5 quintiles for disability. For the Part D
summary Star Rating adjustment for PDPs, the initial categories consist of the 16 combinations
of LIS/DE quartile and disability quartile.
The number of initial categories employed in this first step of the methodology will be
determined based on the distribution of the composition of the contracts’ enrollees. Each initial
category does not need to contain the same number of contracts. It is possible that some initial
categories will have only a small number of contracts or perhaps no contracts based on the
distribution of the contracts’ percentages for LIS/DE and disabled beneficiaries. Alternative
initial groupings may be considered if numerous cells are underpopulated.
(2A) The adjusted overall and summary Star Ratings per contract are calculated using the
adjusted measure-level stars of the measures selected for adjustment instead of the unadjusted
measure-level stars.
(2B) The unadjusted overall and summary Star Ratings per contract are calculated using the
unadjusted measure-level stars of the measures.

127
For the 7 measures that were selected for adjustment, the aggregated summary measure-level
scores were derived from the patient-level data. The summary measure-level scores for the 7
selected measures may differ slightly from the summary scores submitted by the contract. The
unit of analysis for the calculation of the CAI values for the subset of measures selected for
adjustment must be consistent and is necessary for apple-to-apple comparisons.
(3) For each contract and each rating type, the difference between the adjusted overall or
summary Star Rating and the corresponding unadjusted Star Rating is computed.
(4) Within each of the initial categories, the mean difference between the adjusted overall or
summary Star Rating and the corresponding unadjusted Star Rating is determined.
(5) The mean differences for the initial categories in step (4) are examined and categories are
then combined into final adjustment groups to ensure at least 20 MA contracts or 10 PDPs in
each category and attain monotonicity with increasing percentages of LIS/DE and disability.
The initial categories will be collapsed to form the final adjustment categories in a manner that
enforces monotonicity. In other words, initial categories are combined such that, as the
percentages of LIS/DE or disabled beneficiaries within a category increases and the other
dimension does not decrease, the adjustment (value of the CAI) increases. The final adjustment
categories will be created with a minimum number of 20 contracts per each final MA adjustment
group and 10 contracts per each final PDP adjustment group. The guideline for the number of
contracts per final adjustment group is designed to maintain the stability of the estimates. If
possible, final adjustment categories will be collapsed such that CAI values differ by at least
0.01 units in at least one of the two dimensions (LIS/DE and disability). (It may not always be
possible to have final CAI category values differing by at least 0.01 units in at least one
dimension given the goal of imposing monotonicity across both the DE/LIS and disability
dimensions.)
(6) Using the contracts that fall within each of the final adjustment groups, the mean difference
between the adjusted overall or summary Star Rating and the corresponding unadjusted Star
Rating is computed per group.
(7) The set of mean differences for each Star-Rating-specific final adjustment group found in
Step (6) is the CAI value set.
(8) For each contract, the final adjusted overall and/or summary Star Ratings are computed by
adding the corresponding CAI value for the final adjustment category that the contract falls
within based on the contract’s percentages of LIS/DE and disabled beneficiaries to a contract’s
unadjusted overall and/or summary Star Rating
14
. (There are separate CAI values for the overall,
14
The CAI value can be either positive or negative. A positive CAI value will result in an increase of the HPMS posted score
after the application of the CAI value. A negative CAI value will result in a decrease of the HPMS posted rating after the
application of the CAI value.
128
Part C, and Part D summary Star Ratings.) The adjusted overall and summary Star Ratings will
be posted on Plan Finder and HPMS.
The CAI is applied outside of the specification and is applied to each contract’s current year
overall and/or summary Star Ratings. The measure specification for every measure used in the
Star Ratings Program remains unchanged by the CAI adjustment. Each contract within a given
final adjustment group receives the same adjustment to its overall and/or summary Star Rating.
The application of the CAI value for a contract will be carried out rounded to 6 decimal places
for both the unadjusted and adjusted Star Ratings. Rounding will take place after the
application of the CAI value and the rounding rules for the HPMS posted values as detailed in
the Technical Notes will be employed. All Star Ratings are displayed to the nearest half-star.
For the 2017 Star Rating year, the CAI will be applied to the overall and summary scores that
will be calculated as they have been in past using summary scores. In 2017, the rating-specific
adjustment factor that will be applied to contracts’ overall and summary Star Ratings will be
determined using the plan proportion of LIS/DE and disabled beneficiaries from the 2015
enrollment data.
2017 Categorical Adjustment Index Values
The values of the 2017 CAI values are below. The upper limit for each category is not included
in that category, but rather the next higher category. For example, if a contract’s percentage of
LIS/DE beneficiaries is 8.94%, the contract’s LIS/DE decile will be 2. The exceptions for the
upper limit exclusion for a class are the tenth decile for LIS/DE and the fifth quintile for
disabled.
Tables 1 and 2 provide the range of the percentages that correspond to the LIS/DE deciles and
disability quintiles for the categorization of MA contracts for the CAI for the overall Star Rating.
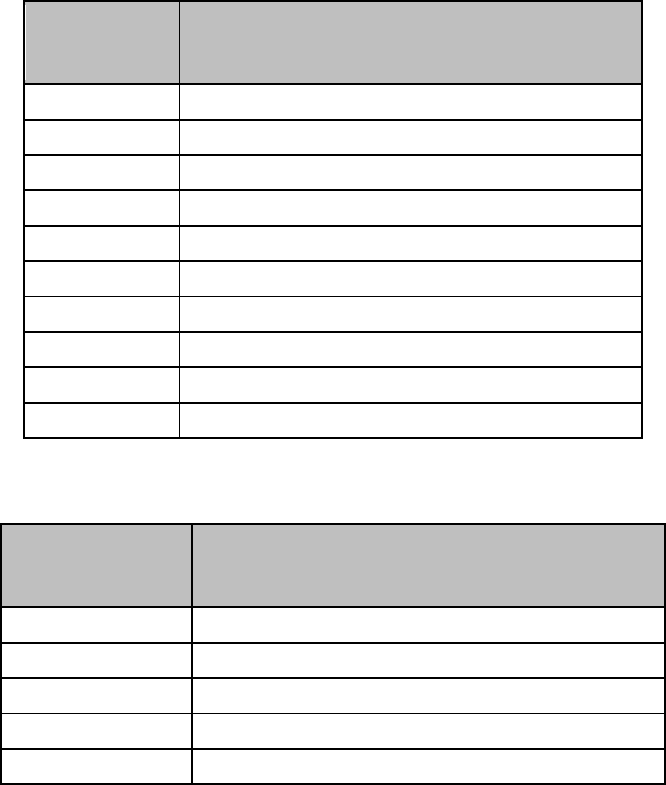
129
Table 1: Categorization of MA Contracts into LIS/DE Deciles for the Overall Rating
LIS/DE Decile
Percentage of Contract’s LIS/DE Beneficiaries
1
0.00% to less than 8.94%
2
8.94% to less than 12.60%
3
12.60% to less than 15.70%
4
15.70% to less than 19.00%
5
19.00% to less than 23.90%
6
23.90% to less than 30.37%
7
30.37% to less than 46.30%
8
46.30% to less than 73.90%
9
73.90% to less than 99.00%
10
99.00% to 100.00%
Table 2: Categorization of MA Contracts into Disability Quintiles for the Overall Rating
Disability Quintile
Percentage of Contract’s Disabled Beneficiaries
1
0.00% to less than 9.00%
2
9.00% to less than 13.10%
3
13.10% to less than 18.86%
4
18.86% to less than 26.50%
5
26.50% to 100.00%

130
Table 3 provides the description of each of the final adjustment categories for the overall Star
Rating for MA contracts and the associated values of the CAI for each final adjustment category.
Table 3: Final Adjustment Categories and CAI Values for the Overall Rating
Final Adjustment
Category
%LIS/DE
Decile
%Disability
Quintile
CAI Value
1
1
1
−0.015566
2
2-9
1
−0.006181
1-6
2
3
1-5
3-5
0.002408
6
3
4
7-8
2-3
0.013514
5
10
1-4
0.024680
9
2-4
6-8
4
6
6-8
5
0.028531
7
9
5
0.054610
8
10
5
0.081245
Tables 4 and 5 provide the range of the percentages that correspond to the LIS/DE deciles and
disability quintiles for the initial categories for the determination of the CAI values for the Part C
Summary.

131
Table 4: Categorization of MA Contracts into LIS/DE Deciles for the Part C Summary
Rating
LIS/DE Decile
Percentage of Contract’s LIS/DE Beneficiaries
1
0.00% to less than 8.72%
2
8.72% to less than 12.38%
3
12.38% to less than 15.56%
4
15.56% to less than 18.81%
5
18.81% to less than 23.56%
6
23.56% to less than 29.84%
7
29.84% to less than 45.43%
8
45.43% to less than 71.92%
9
71.92% to less than 99.01%
10
99.01% to 100.00%
Table 5: Categorization of MA Contracts into Disability Quintiles for the Part C Summary
Rating
Disability Quintile
Percentage of Contract’s Disabled Beneficiaries
1
0.00% to less than 8.81%
2
8.81% to less than 12.69%
3
12.69% to less than 18.69%
4
18.69% to less than 26.30%
5
26.30% to 100.00%
Table 6 provides the description of each of the final adjustment categories for the Part C
summary rating and the associated value of the CAI for each final adjustment category.

132
Table 6: Final Adjustment Categories and CAI Values for the Part C Summary Rating
Final Adjustment
Category
%LIS/DE
Decile
%Disability
Quintile
CAI Value
1
1
1
−0.017914
2
2-8
1
−0.002435
1-6
2
3
1-5
3-5
0.005340
6
3
4
7-8
2-3
0.010543
5
9-10
1-3
0.014127
6-10
4
6
6-8
5
0.020904
7
9
5
0.032875
8
10
5
0.046083
Tables 7 and 8 below provide the range of the percentages that correspond to the LIS/DE deciles
and the disability quintiles for the initial categories for the determination of the CAI values for
the Part D summary rating for MA-PDs.
Table 7: Categorization of MA-PD Contracts into LIS/DE Deciles for the Part D Summary
Rating
LIS/DE Decile
Percentage of Contract’s LIS/DE Beneficiaries
1
0.00% to less than 8.94%
2
8.94% to less than 13.01%
3
13.01% to less than 16.11%
4
16.11% to less than 20.43%
5
20.43% to less than 26.25%
6
26.25% to less than 32.62%
7
32.62% to less than 47.87%
8
47.87% to less than 78.88%
9
78.88% to less than 99.60%
10
99.60% to 100.00%

133
Table 8: Categorization of MA-PD Contracts into Disability Quintiles for the Part D
Summary Rating
Disability Quintile
Percentage of Contract’s Disabled Beneficiaries
1
0.00% to less than 9.39%
2
9.39% to less than 13.58%
3
13.58% to less than 19.95%
4
19.95% to less than 29.71%
5
29.71% to 100.00%
Table 9 provides the description of each of the final adjustment categories for the Part D
summary rating for MA-PDs and the associated values of the CAI for each final adjustment
category.
Table 9: Final Adjustment Categories and CAI Values for the Part D Summary Rating for
MA-PDs
Final Adjustment Category
%LIS/DE Deciles
%Disability Quintiles
CAI Value
1
1-5
1-2
−0.007435
2
1-5
3-5
−0.002020
3
6-10
1-3
0.000944
4
6-10
4
0.027383
5
6-8
5
0.052087
6
9
5
0.088059
7
10
5
0.091937
Tables 10 and 11 provide the range of the percentages that correspond to the LIS/DE and
disability quartiles for the initial categories for the determination of the CAI values for the Part D
summary rating for PDPs. Quartiles are used for both dimensions (LIS/DE and disability) due to
the limited number of PDPs as compared to MA contracts.
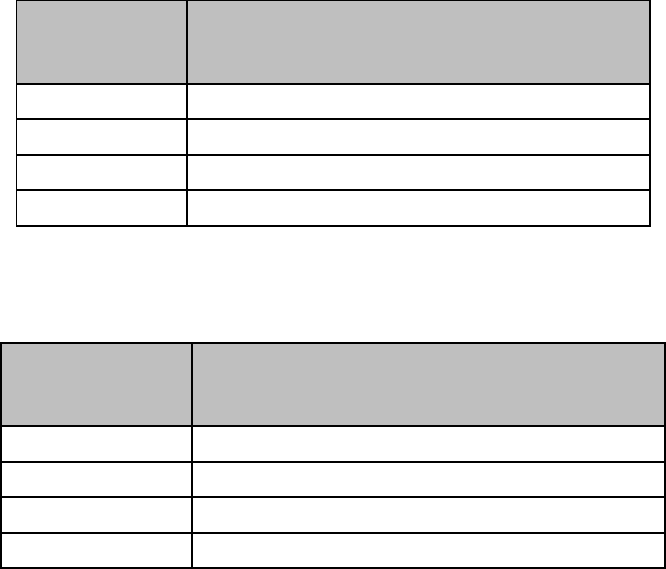
134
Table 10: Categorization of PDP Contracts into LIS/DE Quartiles for the Part D Summary
Rating
LIS/DE Quartile
Percentage of Contract’s LIS/DE Beneficiaries
1
0.00% to less than 3.79%
2
3.79% to less than 11.41%
3
11.41% to less than 49.43%
4
49.43% to 100.00%
Table 11: Categorization of PDP Contracts into Disability Quartiles for the Part D
Summary Rating
Disability Quartile
Percentage of Contract’s Disabled Beneficiaries
1
0.00% to less than 5.37%
2
5.37% to less than 9.98%
3
9.98% to less than 28.32%
4
28.32% to 100.00%

135
Table 12 provides the description of each of the final adjustment categories for the Part D
summary rating for PDPs and the associated value of the CAI per final adjustment category.
Please note that the CAI values for the Part D summary rating for PDPs are different from the
CAI values for the Part D summary rating for MA contracts.
Categories were chosen to enforce monotonicity and to yield a minimum of 10 contracts per final
adjustment category. There are three final adjustment categories for PDPs for the Part D
summary rating.
Table 12: Final Adjustment Categories and CAI Values for the Part D Summary Rating
for PDPs
Final Adjustment Category
%LIS/DE Quartiles
%Disability Quartiles
CAI Value
1
1-2
1-4
−0.108739
3-4
1-2
2
3
3-4
−0.022527
4
3
3
4
4
0.127092
Additional response to address lack of an LIS indicator for enrollees in Puerto Rico
Under statute, aspects of the Medicare and Medicaid programs are implemented differently in
Puerto Rico. We are cognizant of the particular challenges in not only Puerto Rico, but in all
territories without LIS and propose an additional analytical adjustment for contracts serving
these areas exclusively to address the fact that the Part D LIS is not available there.
Notably, Puerto Rican beneficiaries are not eligible for LIS, which is an important element of the
methodology for the analytical adjustment. (Beneficiaries in the 50 states and DC are eligible for
LIS if their income is less than 150% of the Federal Poverty Level (FPL) and they meet the
applicable resource requirement.) In the draft Call Letter, CMS proposed implementing an
additional adjustment to make the proposed CAI analytical adjustment equitable for contracts in
Puerto Rico. The additional adjustment would be used to identify beneficiaries in Puerto Rico’s
contracts whose incomes would result in an LIS designation in the 50 states and DC. Although
LIS in the states depends on both income and resources, a data source for resource information
for PR enrollees is not available.
Representatives of and advocates for Puerto Rico and MA organizations have expressed
additional concerns about the sensitivity of the Star Ratings in responses to the 2016 draft Call
Letter and the Request for Comments released in 2015. CMS responded in the 2017 draft Call
Letter by proposing two additional provisions in the 2017 Star Ratings to specifically address

136
these concerns. CMS proposed for contracts that are solely serving beneficiaries in Puerto Rico:
(1) the use of an LIS indicator that would be used in conjunction with the CAI analytical
adjustment, and (2) a differentiated weighting scheme for the Part D medication adherence
measures in the calculation of the overall and summary Star Ratings.
In order to determine the LIS indicator for contracts in Puerto Rico, CMS must use a data source
that is readily available at this time. For the 2017 Star Ratings, CMS proposed employing the
contract-specific proportion of DE beneficiaries in Puerto Rico calculated using the rating year
enrollment data and the overall mean proportion of beneficiaries at or below 150% of the FPL in
Puerto Rico based on the American Community Survey (ACS). The data source for the LIS
indicator must provide valid, reliable estimates for use in the Star Ratings. We are cognizant of
the statutory differences in the implementation of the Medicaid Program in Puerto Rico
including the eligibility for DE status that is limited to a lower percentage of the FPL than in the
states due to the cap on the Federal Medical Assistance Percentage (FMAP) in the territories.
The contract-level modified LIS/DE proportion for Puerto Rico was proposed to be developed
from two sources of information: (1) the overall proportion of beneficiaries in Puerto Rico with
incomes less than 150% of the FPL and (2) each contract’s proportion of DE beneficiaries using
the most current data available. A linear regression model using the most recent data would be
developed to predict the percentage of LIS/DE in a contract using the percentage of DE using
MA contracts in the 10 states with the highest poverty.
15
The parameters from the model would
then be used to estimate the percentage LIS/DE for each Puerto Rican contract (i.e., contracts
with a service area only in Puerto Rico) from the contract-specific proportion DE. These
estimates then would be adjusted to reflect the higher overall level of poverty in Puerto Rico by
using data from the ACS. Using the model developed, each contract’s proportion of DE
beneficiaries in Puerto Rico would have a corresponding proportion of LIS to create a contract-
level measure of LIS/DE percentage to be used in the CAI.
CMS also recognizes the additional challenge unique to Puerto Rico related to the medication
adherence measures in the Star Ratings Program. It has been shown that beneficiaries’ out-of-
pocket costs may adversely affect medication adherence, which presents an additional barrier for
Puerto Rican contracts serving beneficiaries whose incomes would result in an LIS designation
in the states. In the past, CMS has considered reducing the weights for the Medication
Adherence measures, but in general such changes were not supported, and ultimately CMS
decided not to move forward with these proposals.
15
The preliminary modelling suggested employing the 50 states and the District of Columbia results in very high accuracy in
predicting contract-level LIS from contract-level DE. There is an insignificant impact on the model coefficients when restricting
the data source to the lower-income subsets of states. CMS is moving forward using the percentage of DE using MA contracts in
the 10 states with the highest poverty to create a contract-level measure of LIS/DE percentage to be used in the CAI. The states
used for the development of the model are: Mississippi, New Mexico, Louisiana, Arkansas, Georgia, DC, Kentucky, Alabama,
Arizona, and South Carolina. The list of states would be updated each year in the Technical Notes.

137
We commend the Puerto Rican contracts on their improved performance overall across the 2016
Star Ratings and in particular the Part D Medication Adherence measures. This year, CMS
proposed an additional option to the LIS/DE adjustment noted above, one that is similar to a
previous proposal, but limited to MAO and PDP contracts that operate solely in Puerto Rico or
other non-continental territories in order to address the unique challenges of improving
medication adherence in those areas. For the 2017 Star Ratings, CMS proposed to reduce the
weights of the three Part D Medication Adherence measures to zero for the calculation of the
overall and summary ratings, and retain the values and the associated weight of the three
adherence measures for the calculation of the improvement factor.
The summary of the simulations provided in February 2016 in the CY 2017 draft Call Letter and
the individual contract simulations provided through HPMS used only income, not resource,
information to simulate the LIS indicator as described above. The value for the LIS indicator in
Puerto Rico (determined through modeling) was used in the application of the CAI analytical
adjustment for the overall and summary Star Ratings.
16
Using both the LIS indicator and CAI
for contracts in Puerto Rico resulted in one contract realizing an increase in its overall Star
Rating by half a star. (With IS, one contract would have experienced a decline in its overall
Rating by half a star). There were no changes in the Part C or Part D summary ratings for Puerto
Rican contracts for the CAI simulation. (For the IS simulation, one MA Puerto Rican contract
would experience a decline by half a star in its Part C summary rating and another MA contract
would experience a decline by half a star in its Part D summary rating. )
The simulations of the down weighting of the adherence measures for Puerto Rico resulted in
four MA-PDs increasing by a half-star in its overall rating, independent of making an SES
adjustment. With the down weighting of the adherence measures, one PDP increased one star in
its Part D summary rating.
Overall, the draft Call Letter commenters expressed appreciation for acknowledging the unique
challenges of Puerto Rico contacts and widespread support for the estimated LIS indicator and,
the reduction in the weights for the three Part D adherence measures. Based on these comments,
CMS will implement the interim estimates for the LIS indicator using modelling based on the 10
states with the highest level of poverty for the 2017 Star Ratings. In addition, for the 2017
ratings year, CMS will employ the data source as outlined in the draft Call Letter (i.e., the ACS)
instead of waiting for the availability of a different data source. CMS has explored other sources
of data for use in determining the LIS indicator for the upcoming rating year, but at this time no
other source has been identified. We continue to encourage stakeholders in Puerto Rico to
provide data appropriate for determining the LIS indicator.
16
Currently, none of the territories, except Puerto Rico, have contracts that serve exclusively beneficiaries within the territory.
The proposed changes discussed in this section will also apply to other territories without the LIS if those contracts serve
exclusively beneficiaries in the territory.
138
CMS will also move forward to reduce the weights of the three Part D Medication Adherence
measures to zero for the calculation of the overall and summary ratings for contacts operating
solely in Puerto Rico. Further, to continue to create incentives to improve medication
adherences in Puerto Rico, CMS will retain the adherence measures in the determination of the
improvement measure.
2017 CMS Display Measures
Display measures on CMS.gov are not part of the Star Ratings. These may include measures that
have been transitioned from the Star Ratings, new measures that are being tested before inclusion
into the Star Ratings, or measures displayed for informational purposes. Similar to the process
used in 2016, organizations and sponsors will have the opportunity to preview their data for the
display measures prior to release on CMS’ website. Data for measures moved to the display
page will continue to be collected and monitored; poor scores on display measures may reveal
underlying compliance and performance issues that are subject to enforcement actions by CMS.
It is expected that all 2016 display measures will continue to be shown on CMS.gov in 2017.
CMS will continue to provide advance notice regarding measures considered for implementation
as future Star Ratings measures. Other display measures may be provided as information only.
Below are a number of revised or new measures for the 2017 display page.
1. Timely Receipt of Case Files for Appeals (Part D) & Timely Effectuation of Appeals
(Part D). For the 2016 display measures, the data time frame for both measures was January
1, 2015 – June 30, 2015. CMS will change the data time frame from the first six months of
the current year to January 1 – December 31 of the previous year. For example, the 2017
display measures will be based on IRE data from January 1, 2015-December 31, 2015. This
change will allow the appeal display measures to match the same timeframe used for the Part
D Appeal Star Ratings measures.
2. Medication Reconciliation Post Discharge (Part C). The Medication Reconciliation Post-
Discharge (MRP) measure assesses the percentage of discharges from acute or non-acute
inpatient facilities for members 66 years of age and older for whom medications were
reconciled within 30 days of discharge. This measure has been collected in SNP HEDIS
since 2008. NCQA made two changes: 1) expanded the coverage on this measure from
Medicare SNPs only to all MA plans; and 2) expanded the age range to members 18 years
and older. Both of these changes for HEDIS 2016 are seen as important steps to measure the
quality of care coordination post-discharge for MA beneficiaries as well as ensuring patient
safety. CMS will include this measure on the 2017 display page and in the 2018 Star
Ratings. Please refer to the NCQA HEDIS 2016 Technical Specifications for Health Plans
Volume 2 for measure construction and technical specifications.
3. Hospitalizations for Potentially Preventable Complications (Part C). NCQA added to
HEDIS 2016 a risk-adjusted measure of hospitalization for ambulatory care sensitive
139
conditions based on the NQF-endorsed Prevention Quality Indicators (PQI), developed by
AHRQ. This measure assesses the rate of hospitalization for complications of chronic and
acute ambulatory care-sensitive conditions. The measure is therefore an important indicator
of care coordination. CMS will include this measure on the 2017 display page and in the
2018 Star Ratings unless there are data issues with the initial data collection. Please refer to
the NCQA HEDIS 2016 Technical Specifications for Health Plans Volume 2 for measure
construction and technical specifications.
4. Statin Therapy for Patients with Cardiovascular Disease (Part C). NCQA has added two
sets of statin therapy measures to HEDIS aligned with the 2013 ACC/AHA blood cholesterol
guidelines. These measures are focused on two of the major statin benefit groups described
in the guidelines: patients with clinical atherosclerotic cardiovascular disease and patients
with diabetes. Since some of these HEDIS measures overlap with the measures developed
by the PQA, CMS will include only one of the HEDIS measures on the 2017 display page
where it will remain for two years. After gaining experience with the new treatment
guidelines and metric, we plan to include this measure in the 2019 Star Ratings. This
measure focuses on statin therapy for patients with cardiovascular disease. It is the
percentage of males 21 to 75 years of age and females 40 to 75 years of age who were
identified as having clinical atherosclerotic cardiovascular disease and were dispensed at
least one high or moderate-intensity statin medication during the measurement year.
5. Asthma Measures (Part C). NCQA has expanded its asthma measures to include older
adults. HEDIS 2016 includes two measures for older adults. Medication Management for
People with Asthma is the percentage of members 5 to 85 years of age who were identified
as having persistent asthma and were dispensed appropriate medications that they remained
on during the treatment period (i.e., first prescription date through end of measurement year).
The Asthma Medication Ratio is the percentage of members who were identified as having
persistent asthma and had a ratio of controller medications to total asthma medications of
0.50 or greater during the measurement year. CMS has shared all comments received with
NCQA and will continue to monitor the development of these measures. CMS will include
these on the 2017 and 2018 display page and will consider these for inclusion in Star Ratings
for future years.
6. Statin Use in Persons with Diabetes (SUPD) (Part D). This new PQA-endorsed measure,
Statin Use in Persons with Diabetes (SUPD), calculates the percentage of patients between
40 and 75 years old who received at least two diabetes medication fills and also received a
statin medication during the measurement period. Beneficiaries in hospice according to the
Enrollment Database (EDB) will be excluded from the denominator of the SUPD measure
for the entire year. Part D sponsors have received year of service 2015 SUPD measure
reports on a monthly basis through the Patient Safety Analysis website, and we will add the
SUPD measure to the 2017 display page (using 2015 data) where it will remain for two

140
years. After gaining experience with the new treatment guidelines and metric, we plan to add
the SUPD measure to the 2019 Star Ratings (using 2017 data).
Lastly, in January 2015, the PQA’s Quality Metrics Expert Panel (QMEP) considered
whether beneficiaries taking proprotein convertase subtilisin/kexin type 9 (PCSK-9)
inhibitors should be excluded from the measure denominator. At this time, the QMEP
decided not to exclude beneficiaries taking PCSK-9 inhibitors from SUPD measure
denominator. It is our understanding that the PQA will review the measure specifications
again when more information is available about this new therapeutic class.
Forecasting to 2018 and Beyond
The following describes changes to existing measures and potential new measures. CMS will
also monitor any additional measures developed by NCQA or PQA for potential incorporation
into the Star Ratings for 2018 or later.
New Measures
The section above describes a number of new measures under consideration for the 2018 Star
Ratings that will be reported as 2017 display measures. The following are additional measures
under consideration for the Star Ratings or display measures for 2018 and beyond.
1. Care Coordination Measures (Part C). Effective care coordination contributes to improved
health outcomes. CMS believes that 5-star contracts perform well on our Star Ratings
measures because they understand how to effectively coordinate care for their enrollees. Our
assumption about plan care coordination activities, however, is based largely on anecdote and
discussions with high performing plans, as well as on data we collect from CAHPS surveys,
which reflect enrollees’ experiences with the care they receive.
CMS is working to expand efforts in this area. To identify potential new care coordination
measures, CMS has awarded two contracts to conduct targeted research, extensive literature
reviews, and data analysis, and to engage in discussions with expert panels and high
performing plans. As part of this effort, the contractors are using various data sources such
as administrative data, encounter data, Part D data and medical record reviews. We are
considering whether the measures should be focused on subgroups of MA enrollees or all
MA enrollees. We are also considering the activities that best represent care coordination,
such as ensuring seamless transitions across settings, appropriate follow up after inpatient
and emergency department visits, communication across providers, and comprehensive
assessments, as well as the relationship between the plan and provider in care coordination
activities. CMS continues to welcome comments on measures that could be developed using
MA encounter data. We will provide updates to the industry as this work progresses.

141
2. Depression Measures (Part C). NCQA has adapted a provider-level depression outcome
measure developed by Minnesota Community Measurement for use in HEDIS. Depression
Remission or Response in Adolescents and Adults (DRR) uses a patient-reported outcome
measure, the PHQ-9 tool, to assess whether patients with depression have achieved remission
or have an improvement in their symptoms. The measure assesses the percentage of
individuals age 12 and older with depression and an elevated PHQ-9 score (greater than 9)
who achieve a PHQ-9 score of less than 5 at six months or have a 50% reduction in their
PHQ-9 score. This measure also uses a new data collection methodology for HEDIS, relying
on data coming from electronic clinical data systems (e.g., EHRs, clinical registries, case
management records). If approved, the new measure would be published in HEDIS 2017.
CMS shared with NCQA comments received as part of our Request for Comments and draft
Call Letter on this topic and will continue to monitor the development of this measure.
3. Appropriate Pain Management (Part C). NCQA is exploring opportunities to develop a
new measure(s) focusing on appropriate pain management. The intent is to assess the quality
of pain management and treatment. There is no definite timeline established for the
development of this measure.
4. Use of Opioids from Multiple Providers or at High Dosage in Persons without Cancer
(Part D). In the 2016 Call Letter, we noted that three opioid overutilization measures were
in development by the PQA. We further stated that if these measures were endorsed by the
PQA prior to the 2017 bid deadline in June 2016 that we may adopt them as future display
measures or alternatively use them in the Overutilization Monitoring System (OMS). The
measures were endorsed by the PQA in May 2015.
PQA’s three opioid measures examine multi-provider, high dosage opioid use among
individuals 18 years and older without cancer and not in hospice care.
Measure 1 (Opioid High Dosage): The proportion (XX out of 1,000) of individuals without
cancer or hospice receiving prescriptions for opioids with a daily dosage greater than 120 mg
morphine equivalent dose (MED) for 90 consecutive days or longer.
Measure 2 (Multiple Prescribers and Multiple Pharmacies): The proportion (XX out of
1,000) of individuals without cancer or hospice receiving prescriptions for opioids from four
(4) or more prescribers AND four (4) or more pharmacies.
Measure 3 (Multi-Provider, High Dosage): The proportion (XX out of 1,000) of individuals
without cancer or hospice receiving prescriptions for opioids with a daily dosage greater than
120 mg morphine equivalent dose (MED) for 90 consecutive days or longer, AND who
received opioid prescriptions from four (4) or more prescribers AND four (4) or more
pharmacies.

142
We tested the measures using the PQA specifications. We will develop new patient safety
reports for the three opioid overutilization measures to provide to Part D sponsors on a
monthly basis through the Patient Safety Analysis website, similar to the other patient safety
measures. The website also includes the OMS. The reports will allow sponsors to track their
performance over time and allow for contract level trending and outlier analyses. Reports
will be distributed beginning with 2016 dates of service. After at least one year to gain
experience with the measures we will add these three measures to the 2019 Part D display
page (using 2017 data). We are not adding these measures to the Star Ratings at this time
due to concerns (1) about the current lack of consensus clinical guidelines for the use of
opioids to treat chronic, non-cancer pain and potential exceptions due to medical necessity
and (2) pending additional analysis on diagnosis data sources, such as newly available
encounter data for Medicare Part C and resolving timing issues of RAPS file updates, which
are used to identify exclusions for certain cancer conditions.
These measures were developed and endorsed by the PQA prior to publication of the CDC
Guideline for Prescribing Opioids for Chronic Pain. We encourage the PQA to review the
CDC Guideline and consider potential updates to the measure specifications as applicable.
Additionally, NCQA is adapting the three opioid overuse measures developed by the PQA
for potential use in HEDIS.
5. Antipsychotic Use in Persons with Dementia (APD) (Part D). CMS has been particularly
concerned with the unnecessary use of antipsychotic drugs in nursing homes and, as a result,
has pursued strategies to increase awareness of antipsychotic use in long term care settings.
In 2013, we began to calculate a general atypical antipsychotic utilization rate, called Rate of
Chronic Use of Atypical Antipsychotics by Elderly Beneficiaries in Nursing Homes, for
inclusion in the Part D display measures. The average rates decreased from approximately
24.0% in 2011 to 21.4% in 2013.
There continues to be increased attention on this important issue. The United States
Government Accountability Office (GAO) released a report
17
in January 2015 describing the
inappropriate use of antipsychotics in Part D beneficiaries with dementia, in both community
(i.e., outside of nursing homes) and long-stay nursing home residents during 2012, with
recommendations for CMS to address this problem. The GAO conducted this study due to
concerns raised regarding the use of antipsychotic drugs to address the behavioral symptoms
associated with dementia, the FDA’s boxed warning that these drugs may cause an increased
risk of death when used by older adults with dementia, and because the drugs are not
approved for this use.
17
Antipsychotic Drug Use: HHS Has Initiatives to Reduce Use among Older Adults in Nursing Homes, but Should Expand
Efforts to Other Settings. http://www.gao.gov/products/GAO-15-211. GAO-15-211: Published: Jan 30, 2015. Publicly Released:
March 2, 2015.

143
In addition, the PQA endorsed the measure, Antipsychotic Use in Persons with Dementia
(APD). This provides CMS with a new measure developed through a consensus process to
monitor the inappropriate use of antipsychotics in both the nursing home and community
settings across Medicare Part D plans.
We tested this measure based on the PQA specifications. We calculated the APD measure
rate in aggregate for all contracts, MA-PDs, and PDPs, and at the individual contract level,
for all beneficiaries, community-only residents (never a nursing home resident), and both
short-term and long-term nursing home residents that met the inclusion and exclusion
criteria. Beneficiaries were identified as long-stay nursing home residents if they had stays
greater than 100 cumulative days in a nursing home during the year based data in the Long
Term Care Minimum Data Set (MDS). Each beneficiary was counted in only one category
for the entire measurement period within a contract and not considered separately for time
spent in different settings (e.g., a beneficiary who experienced both short-term and long-term
nursing home stays was included only in the long-term category).
To identify the numerator and denominator populations, we used diagnosis data obtained
from inpatient (IP), outpatient (OP), and carrier claims from the Common Working File
(CWF) and RxHCCs from the RAPS. OP and Carrier claims are available for PDP contracts
only. We also adjusted rates based on the number of months beneficiaries are enrolled in
each Part D contract (i.e., member-years adjustment).
We conducted reliability testing using mixed effect logistic regression with varying intercept.
The testing results indicate that the rate variations at the contract level are statistically
significant, providing evidence that the measure is reliable.
A report, Antipsychotic Use in Part D Enrollees with Dementia, which summarizes the
testing results, is posted on CMS.gov at: https://www.cms.gov/Medicare/Prescription-Drug-
Coverage/PrescriptionDrugCovGenIn/Downloads/Antipsychotic-Use-in-Part-D-Enrollees-
with-Dementia-v12092015.pdf.
We will develop new patient safety APD measure reports to provide to Part D sponsors on a
monthly basis through the Patient Safety Analysis website beginning with year of service
2016. We will add the overall APD measure plus breakout rates for community-only
residents, short-term nursing home residents, and long-term nursing home residents to the
2018 Part D display measure set (using 2016 data) to continue to draw attention to the
inappropriate use of antipsychotics in persons with dementia without an appropriate mental
health diagnosis in both the community and nursing home settings. The APD measure will
replace the Rate of Chronic Use of Atypical Antipsychotics by Elderly Beneficiaries in
Nursing Homes display measure. However, we do not propose adding this measure to the
Star Ratings pending additional research on diagnosis data sources, such as newly available
encounter data for Medicare Part C and resolving timing issues of RAPS file updates.

144
Changes to Existing Star Ratings and Display Measures and Potential Future
Changes
1.
Colorectal Cancer Screening (Part C Star Rating)
. The Colorectal Cancer Screening
(COL) measure assesses the percentage of adults 50-75 years of age who had appropriate
screening for colorectal cancer. This measure is based on the U.S. Preventive Services Task
Force (USPSTF) guideline on colorectal cancer screening in adults age 50-75. NCQA is
monitoring updates to the guideline as the USPSTF has recently released a draft
recommendation statement. NCQA will consider revisions to the COL measure once the
USPSTF final recommendation statement is published. It is anticipated that the final release
of recommendations will not occur until late 2016.
2.
Fall Risk Management (Part C Star Rating).
The Fall Risk Management (FRM) measure,
collected through the Health Outcomes Survey, consists of the following two indicators: 1)
Discussing Fall Risk assesses the percentage of Medicare members 75 years of age and older
or 65-74 years of age with a balance or walking problem or fall in the past 12 months who
discussed falls or problems with balance or walking with their current practitioner; and 2)
Managing Fall Risk assesses the percentage of Medicare members 65 years of age and older
who had a fall or had problems with balance or walking in the past 12 months and received
fall risk intervention from their current practitioner (defined as suggesting use of a cane or
walker, a vision or hearing test, physical therapy or exercise, or taking of a postural blood
pressure). NCQA is currently re-evaluating this measure to align with the most current U.S.
Preventive Services Task Force (USPSTF) guidelines. NCQA is proposing to 1) revise the
denominator in the Discussing Fall Risk indicator to include all Medicare members age 65
and older and 2) revise the numerator for the Managing Fall Risk indicator to include plan
members who report having had an intervention. The survey question will list examples of
interventions to prompt survey respondents to recall if they received any fall risk
management intervention from their provider. These proposed changes, if approved, would
be published in HEDIS 2017 or HEDIS 2018.
3.
Pneumococcal Vaccination Status for Older Adults (Part C Display).
The Pneumococcal
Vaccination Status for Older Adults (PNU) measure, collected through the Medicare CAHPS
survey, assesses the percentage of Medicare members 65 years of age and older who have
ever received a pneumococcal vaccination. In 2014, The Advisory Committee on
Immunization Practices (ACIP) released new recommendations that all adults 65 years of age
and older should receive sequential administration of both PCV13 and PPSV23. NCQA is
considering changes to the measure to align with the most current guidelines. Specifically,
they are evaluating the feasibility of developing a new measure of pneumococcal vaccination
based on alternative data sources, such as administrative claims, state immunization registries
and electronic health records. In the meantime they recommend the following wording
changes to the existing CAHPS measure: “Have you ever had one or more pneumonia shots?
Two shots are usually given in a person’s lifetime and these are different from a flu shot. It is
145
also called the pneumococcal vaccine.” Pending OMB approval the new wording will be
utilized for 2017 CAHPS implementation. This measure is on the CMS display page.
4.
CAHPS measures (Part C & D).
Patient experience surveys such as CAHPS focus on how
patients experienced or perceived key aspects of their care, not how satisfied they were with
their care. CAHPS surveys follow scientific principles in survey design and development.
The surveys are designed to reliably assess the experiences of a large sample of
patients. They use standardized questions and data collection protocols to ensure that
information can be compared across health care settings. CAHPS surveys are developed
with broad stakeholder input, including a public solicitation of measures and a technical
expert panel, and the opportunity for anyone to comment on the surveys through multiple
public comment periods through the Federal Register.
The current MA & PDP CAHPS Survey includes the core CAHPS 4.0 Health Plan Survey.
CMS conducted an experiment in 2015 to understand how CAHPS measures differ between
4.0 and 5.0, and based on the results we will update the survey for future years to reflect
AHRQ’s CAHPS 5.0 Health Plan Survey. The findings from the experiment suggest that
these changes are associated with a small increase in scores for several evaluative MA
measures. These small increases did not significantly differ across contracts. Since there are
no longer fixed thresholds for Star Ratings and they are based on the actual distribution of
scores, there should be no shifts in Star Ratings due to transition to the version 5.0 instrument
compared to what would have been the case with 4.0. Every contract would have the same
expected Star Rating whether version 4.0 or 5.0 is used, and the correlation between this
year’s Star Ratings and next year’s Star Ratings should be the same regardless of whether 4.0
or 5.0 is used next year.
The 5.0 update applies recent improvements in survey design that resulted from development
and testing of the Clinician & Group Surveys. The 5.0 version of the CAHPS Health Plan
Survey incorporates some minor changes into the wording of core items, and a change in the
placement of one core item that also resulted in the deletion of a screener item.
The following are the changes in the 5.0 version of the Health Plan Survey:
The items about access to urgent and non-urgent appointment items were
modified to ask respondents if they were able to get an appointment as soon as
they needed, as opposed to as soon as they thought they needed. Non-urgent
appointments are described as a check-up or routine care rather than health care.
In addition, the phrase, “…not counting the times you needed care right away”
was deleted from these questions. These revisions simplify the items and make
them consistent with questions in other CAHPS surveys.
The item about how often it was easy to get appointments with specialists was
revised to ask respondents if they got an appointment to see a specialist as soon as

146
they needed. This revision makes the item consistent with other CAHPS items
that ask about access to care.
The item about how often it was easy to get care, tests, or treatment was
moved from the Your Health Plan section to the Your Health Care in the Last 6
Months section, because respondents had difficulty attributing this item to the
health plan.
The screener item about getting care, tests, or treatment through the health
plan was deleted because the subsequent question was moved to an earlier section
of the survey and no longer required a screener.
These changes would take effect for the 2017 CAHPS survey administration (used for 2018
Star Ratings) based on OMB approval. We will use the following standard for deciding that
a specification change has occurred for a CAHPS measure in connection with the
modification of the wording to decide whether to exclude the measure from the improvement
measure calculation: (1) at least one item within the measure changed in wording, had a
wording change in its screener, or had a wording change in the immediately preceding item,
and (2) the measure score in version 5.0 was significantly different from the measure score in
version 4.0 in the 5.0 experiment. Three MA measures meet this standard: Getting Care
Quickly, Customer Service, and Care Coordination. Thus, these three measures will be
excluded from the Part C improvement measure for the 2018 Star Ratings.
We are also considering changing the sampling for CAHPS in future years when a contract is
listed in HPMS as a consolidation between July of the prior year and January of the current
year when the CAHPS sample is drawn. The sampling frame for the surviving contract
would include the enrollees for all members of all contracts involved if two or more contracts
consolidate under the same parent organization. We will continue to study this and will give
advance notice before making any changes to the methodology.
CMS provides translations of the MA & PDP CAHPS Survey in Spanish and Chinese. All
translations are the product of translation and review by native speakers of the target
languages and have had multiple rounds of qualitative testing with Medicare beneficiaries
with characteristics similar to the MA & PDP CAHPS population. By providing survey
translations, CMS promotes standardization by assuring that questions are presented
similarly to beneficiaries across and within languages, which also promotes comparability of
the results across vendors and contracts. The survey administration protocol for MA & PDP
CAHPS does not permit “live,” “individual,” or “real-time” translation of the survey by an
interpreter as such an approach does not promote comparability of data, and there is no
mechanism for assuring the accuracy and consistency of the translation. The MA & PDP
CAHPS protocol does allow for the use of proxy respondents in cases where a respondent is
unable to complete the survey.

147
We note that CMS applies standards of reliability to CAHPS results, directly and through
significance testing. Contract measures with interunit reliability (IUR) less than 0.60 are
flagged as Very Low Reliability and are excluded from use in public reports or incentive
payments. Those with IUR less than 0.72 are flagged as low reliability (up to 12% of the
entire number of participating contracts) and limited use is made of those data, requiring
stronger supporting evidence to classify a contract as different from average. The number of
contracts falling below this criterion varies by measure from a few percent of contracts to
about half. Tests of significance also play a role in CAHPS analyses, and these automatically
adjust for the precision of available data. Finally, CMS offers contracts the option of
augmenting their CAHPS sample sizes if they wish to obtain more precise overall results
and/or perform subgroup analyses with larger samples. CMS reminds sponsors that the case-
mix coefficients for the CAHPS Star Ratings measures are available in the Star Ratings
Technical Notes each year.
We received several comments requesting that CMS shorten the MA CAHPS survey. CMS
is committed to shortening the 2017 MA CAHPS survey by removing some questions that
are not used in current Star Ratings measures.
5. MPF Price Accuracy (Part D Star Rating). CMS plans to make a few updates to this
measure for the 2018 Star Ratings. The first change is related to the method by which claims
are excluded from the measure. Currently, the measure is limited to claims filled for a 30-
day supply at pharmacies reported by sponsors as retail only or retail and limited access only
in their MPF Pharmacy Cost files. That is, claims that are not filled for exactly a 30-day
supply, or claims filled for 60 and 90 days’ supply are excluded. Additionally, claims filled
by retail pharmacies that are also long term care, mail order, or home infusion pharmacies are
excluded. These restrictions result in the exclusion of many PDEs, thus potentially biasing
the reliability of the measure.
We plan to include claims with 28-34 day supply, as we believe it would be appropriate to
compare their PDE costs to MPF’s fixed display of 1 month pricing. We also plan to include
60-62 and 90-93 day supply claims for a more comprehensive evaluation of PDE claims.
Beginning with CY 2015 MPF submissions, plans must provide brand and generic
dispensing fees for 60 and 90 day supply claims in the Pharmacy Cost file. CMS can use
these data, along with 60 and 90 day supply Pricing File data, to compare MPF and PDE
costs.
Additionally, we plan to use the PDE-reported Pharmacy Service Type code in conjunction
with the MPF Pharmacy Cost data to identify retail claims. CMS began requiring
pharmacies to populate the Pharmacy Service Type field on all PDEs at the end of February
2013. We recommend expanding the retail claims identification process to include all PDEs
that are from retail pharmacies according to the Pharmacy Cost data and have a Pharmacy
Service Type of either Community/Retail or Managed Care Organization (MCO). Although
148
some sponsors cited concern about the accuracy of these data as reported by pharmacists,
Part D sponsors are ultimately responsible for the accuracy of their submitted PDE to CMS.
According to PDE requirements, CMS expects “…sponsors and their network pharmacies to
develop and implement controls to improve the accuracy of this information during 2013…”
This methodology change would increase the number of PDEs eligible for inclusion in the
Price Accuracy Scores while continuing to identify only retail claims.
We plan to make changes to the methodology by which price accuracy is calculated. The
current methodology measures the magnitude, but not the frequency, of a contract’s PDE
prices being higher than the MPF prices. A contract’s accuracy score can be significantly
impacted by high price PDEs. As a result, contracts with divergent accurate price reporting
and/or consistency can receive the same Price Accuracy Score. CMS is interested in
modifying the methodology to factor in both how much and how often PDE prices exceeded
the prices reflected on the MPF. The frequency of inaccuracy by a contract would be the
percent of claims where the PDE price is greater than the MPF price. The numerator is the
number of claims where the PDE price is greater than MPF price, and the denominator is the
total number of claims. This ratio is then subtracted from 1 and multiplied by 100 to
calculate the Claim Percentage Score, with 100 as the best possible score and 0 as the worst
possible score. The contract’s accuracy score would be a composite of the Price Accuracy
Score and the Claim Percentage Score.
By capturing the frequency of inaccuracy as well as the magnitude, the measure would better
depict the reliability of a contract’s MPF advertised prices. CMS is aware that while the
MPF display is updated every two weeks, real time pricing, at the point of sale, can change as
often as every day. Some sponsors have expressed concern that in order to perform well in
the Price Accuracy measure, they cannot offer lower prices at point of sale in real time than
the prices are displayed on MPF. We note that PDEs priced lower than MPF displayed
pricing do not lower a contract’s score in this measure.
CMS’ simulation of this proposal found little change in the range of contracts’ accuracy
scores. Other options we explored include measuring the magnitude of inaccuracy as a
percentage cost difference, instead of the current measure’s use of absolute cost difference.
Testing however found this method may overstate small differences between PDE and MPF
costs for low-cost claims. For example, when using percentage cost differences, a claim with
a $2.00 PDE price and a $1.00 MPF price would be considered equally overpriced as a claim
with a $200.00 PDE price and a $100.00 MPF price.
We plan to implement these changes for the 2018 Star Ratings (using 2016 PDE and MPF
data). We believe the changes will greatly improve the Price Accuracy Scores, making them
a more comprehensive assessment of contracts’ price reporting for Part D beneficiaries. For
consistency, we will also implement these changes for the 2018 display measure, Plan
Submitted Higher Prices for Display on MPF.
149
6. Drug-Drug Interactions (DDI) (Part D Display). The PQA-endorsed DDI measure is
currently a Part D display measure. This measure is defined as the percent of Medicare Part
D beneficiaries who received a prescription for a target medication during the measurement
period and who were dispensed a prescription for a contraindicated medication with or
subsequent to the initial prescription.
The PQA has conducted an extensive review of the drug-drug pairs included in the DDI
measure. They engaged a DDI expert panel convened by the University of Arizona on
PQA's behalf, which completed the review, including a comparison to the DDI list developed
for the Office of the National Coordinator for Health Information Technology (ONC). The
Expert Panel's recommendations were reviewed by the PQA’s Measure Update Panel for
consideration by the PQA’s Quality Metrics Expert Panel (QMEP). Next, the PQA will test
the DDI measure specifications because there will be extensive changes. We will closely
monitor any updates to this measure, test updated specifications when available, and propose
changes in the future for the Part D display measure and patient safety reporting.
7. Center for Medicare and Medicaid Innovation Model Tests. We note that some
stakeholders (and commenters to the Request for Comments and draft Call Letter) have
expressed concern regarding the potential for the improvements in quality resulting from the
Medicare Advantage Value-Based Insurance Design (MA-VBID) and the Part D Enhanced
MTM Model test to adversely influence the Star Ratings of contracts ineligible to participate
(or that include some PBPs ineligible to participate). CMS’ goal is to not penalize
participants or non-participants in either model.
As the model tests are implemented, we will closely monitor performance trends of
participating plans across individual measures and determine if any changes are warranted.
For the MA-VBID Model test, CMS is considering the exclusion of some of the model-
participants’ data when calculating measure-level cut points.
The Part D plans participating in the Part D Enhanced MTM Model test will be waived from
the MTM requirements under Section 1860D–4(c)(2) and 42 CFR 423.153(d) and the Part D
Reporting Requirements for MTM. However, Part D sponsors will not be waived from
establishing MTM programs in compliance with current requirements and reporting data for
the remaining plans under each Part D contract. Therefore, the MTM Program CMR
Completion Rates will be calculated using available plan-reported data from the remaining
plans under the Part D contract.
Some stakeholders in response to the Request for Comments and draft Call Letter expressed
concern that Enhanced MTM Model participants will sometimes be significantly advantaged
or disadvantaged by the removal of the participating PBPs from the calculation of the CMR
completion rate measure at the contract level, and have suggested the elimination of this
measure for PDP contracts with model-participating plans. Some alternative possible options

150
are to establish different cut points for model participants or to case-mix adjust scores for the
purpose of determining cut points. We are aware that the national scope of many PDP
contracts must be taken into consideration in evaluating options for addressing potential
differences in performance between participating and non-participating plans. Commenters
requested that CMS engage stakeholders and provide information as these potential
adjustments are developed. CMS will continue to consider how to address any potential
differences in performance between participating and non-participating plans, taking these
comments into consideration.
Measurement and Methodological Enhancements
CMS is committed to continuing to improve the Part C and D Star Ratings by identifying new
measures and methodological enhancements. Feedback or recommendations can help CMS’
continuing analyses, as well as our collaboration with measurement development entities such as
NCQA and PQA.
As announced in the March 8, 2016 HPMS memo, CMS is suspending the reduction in the
overall and summary Star Ratings of contracts that are under sanction, while CMS re-evaluates
the impact of sanctions, audits, and CMPs on the Star Ratings
18
. CMS plans to describe our
proposals in the Request for Comments in fall 2016.
Based on feedback received from the Star Ratings Request for Comments in fall 2015 and the
CY 2017 draft Call Letter concerning our methodology for the Call Center Monitoring measure,
beginning in 2017 CMS will allow the interpreter an extra 60 seconds to address an introductory
question that is asked prior to three specific plan benefit questions. This will affect the 2018 Star
Ratings.
CMS would like to clarify that the Call Center Monitoring tasks are described in the annual
memos issued via HPMS each year, which ask plans to update all phone numbers in
HPMS. Specifically, CMS informs health plans that “[t]he Timeliness Study measures
Medicare Part C and Part D current enrollee beneficiary call center phone lines and pharmacy
technical help desk lines to determine average hold times and disconnect rates” and “The
Accuracy and Accessibility Study measures plan sponsors’ Medicare Part C and Medicare
Part D prospective enrollee beneficiary call center phone lines to determine (1) the availability
of interpreters for individuals, (2) TTY functionality, and (3) the accuracy of plan information
provided by customer service representatives (CSRs) in all languages.” The same description is
used in any compliance action issued. The pharmacy technical assistance line, or what is labeled
as “pharmacy” in the monitoring results or compliance actions, refers to the requirement found at
42 C.F.R. § 423.128(d)(1). The Medicare Marketing Guidelines, at Appendix 3, clarifies the
18
Prior to the suspension of this policy, contracts under an enrollment sanction were automatically assigned 2.5 stars for their
highest rating. If a contract under sanction already had 2.5 stars or lower for their high rating, it received a 1-star reduction.
Contracts were evaluated and adjusted for enrollment sanctions at two periods each year.

151
requirement as, “Part D Sponsors must operate a toll-free pharmacy technical help call center or
make available call support to respond to inquiries from pharmacies and providers regarding the
beneficiary’s Medicare prescription drug benefit; inquiries may pertain to operational areas
such as claims processing, benefit coverage, claims submission, and claims payment.” The
pharmacy technical assistance line listed in HPMS must be the toll-free number that pharmacies
and providers would use to inquire about issues like claims submission or claims processing, and
it is not intended to be the number a beneficiary would call. The Part D current enrollee or
prospective member lines are the numbers intended for use by a current or prospective
beneficiary.
Finally, we note that CMS has a rigorous Quality Assurance and Audit process over the test call
process that involves multiple layers of review before, during and after each monitoring
period. We encourage plans/sponsors to request and review their raw call data to validate the
results. CMS believes that validation of the information by plans/sponsors is an important tool in
our overall review of the monitoring contractor’s performance, and we encourage plans/sponsors
to contact CMS via [email protected] if they believe an error occurred.
Medicare Parts C & D Program Audits
Proposed Release Date for the 2017 Part C and Part D Program Audit Protocols
Each year, the Medicare Parts C & D Oversight & Enforcement Group (MOEG) releases the Part
C and Part D audit protocols to the industry in an effort to be as transparent as possible about our
audit approach. We remain committed to continuous improvement in the development of our
audit processes and protocols, and value the input and feedback of all sponsors and stakeholders.
We have received feedback previously that sponsors would appreciate our audit protocols being
released well in advance of the audit year, to allow more time to implement the new protocols
and prepare for audits.
In the draft Call Letter, we indicated that beginning with the 2017 audit protocols, we would
release the following year’s protocols by the end of July, instead of mid-to-late fall. In other
words, the 2017 protocols will be released in July of 2016. This release date should allow
sponsors sufficient time to program their systems to pull accurate audit universes, conduct self-
assessments, and prepare for an audit.
We noted, however, that this approach would delay our ability to incorporate sponsor’s feedback
on protocols until the following year’s versions were released; so, feedback gathered on 2016
protocols would be incorporated into the 2018 protocols. We received multiple comments from
sponsors, and all were very supportive of publishing audit protocols earlier. However, many
sponsors raised concerns with the lag time that would occur with respect to incorporating
feedback from the industry. We received many suggestions, including issuing interim updates to
protocols in between annual releases, but most sponsors suggested we post protocols in draft,
allow time for comment and then publish them in final. However, our earlier proposal failed to
152
consider the time to get changes to protocols approved by the Office of Management and Budget
(OMB) under the Paperwork Reduction Act (PRA). When protocols are going through the PRA
approval process, they are published in the Federal Register for a 60 day and then subsequent 30
day comment periods. We will solicit sponsor feedback on our protocols during this more
formal process. Audit protocols will be submitted to OMB annually, allowing sponsors an
opportunity to provide feedback and have that feedback considered for incorporation each year.
We will continue to work to issue audit protocols early in the year.
This new release cycle will have a particular impact on the two audit protocols that are being
piloted in 2016, the Medication Therapy Management (MTM) and Provider Network Adequacy
(PNA) protocols.
As stated in the draft Call Letter, we gather feedback from sponsors who take part in an audit
with pilot protocols and use their feedback and experience to evaluate if updates and changes are
needed to our pilot protocols prior to finalizing them. Since we will begin the process of
finalizing the 2017 protocols only a few months into the 2016 pilot audit period, we do not
believe that we will have gathered enough feedback on the pilot protocols prior to the July
release date. Therefore, we are extending the pilot of these protocols into 2017 in order to allow
time to gather feedback and determine if revisions are needed to the pilot audit protocols.
Therefore, these protocols will be subject to a separate release cycle for 2016 and 2017.
As a reminder, sponsors subject to pilot protocols do not receive a score for the pilot, nor does it
factor into their overall audit score. Finally, the results from the pilot audit protocol do not
appear in the final audit report.
We would also like to acknowledge that the Provider Network Adequacy protocol will not be
administered as a normal audit protocol and will not happen in conjunction with the remainder of
our program audits. As mentioned in Section II of this document, wide scale monitoring efforts
are underway with respect to network adequacy and provider directory. MOEG, in coordination
with the Medicare Parts C & D Contract Administration Group (MCAG) are taking a
comprehensive approach to monitor, audit and validate compliance with these requirements.
Therefore, MOEG will be using the results of MCAG’s provider directory monitoring each year
to audit and validate correction of any deficiencies identified throughout the year. Those
organizations that fail to correct and come into compliance with these requirements may be
subject to possible enforcement action, including civil money penalties or enrollment sanctions.
Medicare Parts C & D Enforcement Actions
Civil Money Penalty (CMP) Calculation Methodology
When CMS makes a determination that a plan sponsor’s operational deficiencies adversely
affected or had the substantial likelihood of adversely affecting enrollees, the agency imposes
Civil Money Penalties (CMPs) in accordance with Subpart O of 42 C.F.R. §§ 422 and 423. As
153
noted in the draft Call Letter and reflected again in comments to the draft Call Letter, a number
of plan sponsors and industry groups have requested more information on the approach CMS
uses to determine CMP amounts and how the impact of certain deficiencies are factored into a
given CMP. In response to this interest, CMS plans to release a memo describing our
interpretation of the applicable rules in a CMP Methodology by 2017, but will provide an
opportunity for industry to comment before finalizing. This CMP methodology may be modified
and republished on an as needed basis.
Compliance and Enforcement Actions Related to Part D Auto-Forwards
Part D plan sponsors are required to have procedures for making timely coverage determinations
and redeterminations and for notifying enrollees of those decisions within the required
adjudication timeframes. If notice of the decision is not provided within the required timeframe,
the case must be automatically forwarded to the Part D Independent Review Entity (IRE). While
all auto-forwarded cases represent non-compliance with CMS requirements for timely
processing, of particular concern to CMS are plan sponsors with inordinately high levels of cases
that are auto-forwarded throughout the plan year due to the plan sponsor’s failure to meet the
required adjudication timeframes. The requirements related to auto-forwarding untimely cases
from the sponsor to the Part D IRE are set forth at 42 CFR Part 423, Subpart M and in Chapter
18 of the Medicare Prescription Drug Benefit Manual.
As stated in the draft Call Letter, the volume of cases auto-forwarded to the IRE has been
significant and sustained over the past several years. CMS has been monitoring auto-forward
rates with the expectation that there would be a meaningful reduction of this volume over time as
Part D plan sponsors gained program experience. In 2017, CMS will continue to increase the level
and severity of the compliance and enforcement actions imposed on plans that substantially fail
to comply with adjudication requirements for coverage determinations and redeterminations.
We received a number of comments asking CMS to clarify what thresholds will be used in
determining whether a sponsor is considered an outlier. CMS will use data to determine which
plan sponsors are outliers with respect to untimely decisions and the corresponding rate at which
cases are auto-forwarded to the Part D IRE per 10,000 enrollees. This outlier threshold will be
established each year and will be based on a quarterly auto-forward rate per 10,000
enrollees. This outlier threshold will be in alignment with the Star Ratings auto-forward measure
2-star cut-point (for the 2016 Star Ratings this annual cut-point was 38.5 - 66.8).
Pursuant to § 423.752(c)(1)(i), CMS has the authority to impose CMPs on sponsors that
substantially fail to comply with the requirements related to coverage determinations, appeals
and grievances in accordance with § 423.509(a)(4)(ii). A plan sponsor’s inordinately high auto-
forward rate is evidence of substantial failure to comply with the requirements to notify enrollees
of coverage determination and redetermination decisions within the required timeframes. These
failures adversely affect (or have the substantial likelihood of adversely affecting) beneficiaries
154
by causing inappropriate delays in accessing needed prescription drugs and/or financial hardship
to beneficiaries.
Enforcement Actions Related to One Third Financial Audit Findings
Sections 1857(d)(1) and 1860D-12(b)(c) of the Social Security Act require the HHS Secretary to
provide for the annual audit of the financial records of at least one-third of the Medicare
Advantage Organizations (MAOs) and Prescription Drug Plans (PDPs). The one-third financial
audit program is designed to examine the health plans’ financial records, internal controls over
payment disbursements, Medicare utilization and costs, and the computation of Part C & D
bids. As stated in the draft Call Letter, instances of noncompliance from these audits have
identified significant financial errors, disallowed costs, and internal control weaknesses. While
sponsors are required to put a corrective action in place and rectify their deficiencies, certain
findings with adverse beneficiary impact, such as incorrect or increased cost-sharing or
copayments for beneficiaries, warrant further enforcement actions. As a result, for audits
conducted in 2017 (based on CY 2015) CMS will begin to consider findings and observations of
noncompliance from the one-third financial audits for potential enforcement actions, in
accordance with 42 CFR §§422.752(c)(i) and 423.752(c)(i). We received comments requesting
further information about what criteria will be used in determining potential enforcement actions.
Therefore, information related to these actions will be shared in advance with the industry.
Innovations in Health Plan Design
The CMS Innovation Center is responsible for developing and testing new payment and service
delivery models that will lower costs and improve quality for Medicare, Medicaid, and CHIP
beneficiaries. In the CY 2016 Call Letter, CMS indicated its intention to partner with private
payers to test innovations in health plan design for CMS beneficiaries.
Since the CY 2016 Call Letter, CMS has announced the Medicare Advantage Value-Based
Insurance Design (MA-VBID) and the Part D Enhanced Medication Therapy Management
(MTM) Model tests, both scheduled to begin on January 1, 2017. These model tests are
described below.
We received suggestions for potential model tests for CMS to conduct under Innovation Center
authority, and a request that CMS include both participants and non-participants in model test
learning. CMS appreciates these suggestions, and looks forward to continuing to engage
stakeholders in the model test development and learning processes.
Medicare Advantage Value-Based Insurance Design Model Test
The MA-VBID Model test is an opportunity for MAOs to offer mandatory supplemental benefits
or reduced cost sharing to enrollees with CMS-specified chronic conditions, focused on the
services that are of highest clinical value to them. Only those MAOs approved by CMS to

155
participate in the model may do so, and only within PBPs accepted into the model test. The
model will test whether these interventions can improve health outcomes and lower expenditures
for Medicare Advantage enrollees and for the Medicare program. CMS is conducting the model
test in seven states, and the application period for joining the model in CY 2017 closed in
January 2016.
We received comments supportive of the MA-VBID model test, with suggestions for
improvement in future model years, and will take these suggestions into account. Two
commenters requested that CMS allow participating MAOs to offer supplemental non-covered
benefits contingent on participation in disease management or related programs for the clinically-
targeted enrollee population. CMS views this type of intervention as being within the flexibility
offered by the model test’s Request for Applications, and MAOs wishing to offer innovative
approaches to VBID should make appropriate proposals to CMS for our consideration in future
application cycles.
Part D Enhanced MTM Model
The Part D Enhanced MTM Model will test whether providing Part D sponsors with additional
payment incentives and regulatory flexibilities will engender enhancements in the MTM
program, leading to improved therapeutic outcomes, while reducing net Medicare expenditures.
The model is an opportunity for stand-alone basic Part D plans to right-size their investments in
MTM services, identify and implement innovative strategies to optimize medication use,
improve coordination of care between plans and providers, and strengthen system linkages.
Standalone PDP basic plans that have applied and been approved to participate in the CMS
Innovation Center’s Enhanced MTM Model will offer MTM programs subject to the terms and
conditions of the model test in the five selected Part D regions. All other Part D plans, including
any ineligible plans offered by the PDP sponsors of participating plans, will remain subject to the
current regulatory requirements for MTM programs and must include those costs in their 2017
Part D bids. None of the waivers or funding available to model-participating plans is applicable
to the other ineligible plans offered by those PDP sponsors. A participating plan sponsor may
use lessons learned from model beneficiary and provider engagement and intervention strategies
to increase participation within its mandatory MTM programs in other plans, to the extent
allowable outside of the model. For more information, please visit: https://innovation.cms.gov/
initiatives/enhancedmtm/.
We received comments generally supportive of the Enhanced MTM model test, with several
comments requesting continued robust stakeholder engagement on the model. CMS will take
these comments into consideration as the model progresses. Three commenters suggested that
CMS modify the Enhanced MTM model to allow drug manufacturers to participate in the
development of new MTM strategies. The Enhanced MTM model is designed to test PDP
Sponsor-driven approaches to improving medication usage among at-risk enrollees. The model
156
test does not permit collaboration with drug manufacturers. However CMS will continue to
evaluate all avenues to improve medication usage and health outcomes in considering future
model tests.
Section II – Part C
Guidance on the Future of Provider Directory Requirements and Best Practices
CMS wants to further emphasize the importance of providing accurate provider directories to
MA enrollees. Inaccurate provider directories can impede access to care and bring into question
the adequacy and validity of the MAO’s network as a whole. In concert with previously released
guidance, our focus remains making sure provider directories are accurate for Medicare
beneficiaries and their caregivers who rely on them to make informed decisions regarding their
health care choices.
CMS is aware of pilot programs being tested by some MAOs to use new technology to simplify
the process of updating provider directories for physicians and other network participants. We
are supportive of industry efforts to improve provider directories and encourage MAOs and
providers to continue to work collaboratively to develop more effective and efficient methods of
maintaining accurate provide directories. We see great potential with the use of technologies
that capitalize on machine readable information. To foster the development of such
technologies, we urge both industry and provider community to strive to provide data, including
provider information on network participation, in a machine readable format. CMS has
purposefully not prescribed the means by which MAOs must update their provider directories in
order to allow innovation in this area such as updating provider directories by gathering a digital
representation of provider participation and contact information directly from a provider’s web
page.
We received comments on the critical role that providers play in ensuring provider directory
accuracy. CMS agrees that a component of accuracy relies on providers keeping plans abreast of
changes. CMS has taken this into account in our Medicare Marketing Guidelines (MMG)
regarding quarterly provider outreach and updating any identified errors within 30 days of
receipt. We continue to encourage the industry and the provider community to work
collaboratively to address this important matter.
Preliminary data gathered by CMS, as well as continued stakeholder concerns, has intensified
our concerns with provider directory accuracy. We will continue to aggressively identify and
pursue instances of non-compliance by using a host of oversight methods. For example, with
contractor support, we have developed a comprehensive process for monitoring provider
directory accuracy, which is currently underway. The data collected through our monitoring
activities could drive additional reviews of network adequacy, as well as future monitoring

157
and/or audit-based activities. Moreover, identified areas of non-compliance may be subject to
compliance and/or enforcement actions, including civil money penalties or enrollment sanctions.
We received a number of comments regarding the provider directory monitoring activities
currently underway. Commenters urged CMS to share our methodology for the reviews as well
as to provide preliminary data to MAOs prior to taking any compliance and/or enforcement
action. We will share the methodology in an upcoming HPMS memo. We will also provide
preliminary data related to the monitoring to MAOs prior to taking any action. Additionally,
some commenters requested leniency from CMS as MAOs work to improve accuracy of
provider directories. While we acknowledge the industry’s efforts thus far, our focus remains on
overall directory accuracy, which is a long-standing Medicare Advantage requirement. We will
continue along the path of issuing compliance and enforcement actions when necessary.
CMS also remains committed to making provider directory requirements across CMS programs
consistent. As such, the MA program is taking steps to harmonize the requirements and provide
organizations that operate across multiple CMS programs consistency in the application of
provider directory requirements.
Currently among MA, QHPs and the Medicaid managed care programs, MA provides the least
prescriptive provider directory requirements. (See 42 C.F.R. §422.111(b)(3)(i) and explained in
sections 60.4 and 100.4 of the Medicare Marketing Guidelines (https://www.cms.gov/Medicare/
Health-Plans/ManagedCareMarketing/Downloads/2016-Medicare-Marketing-Guidelines-
Updated.pdf). The MA program also has the fewest data elements required for its provider
directory. In addition, both Medicaid and the QHPs have moved toward some level of machine
readability for online provider directory content (see 45 C.F.R. 156.230(c) with additional
guidance provided via Draft 2017 Letter to Issuers in the Federally-facilitated Marketplaces; and
Proposed Medicaid Final Rule CMS–2390–P, 42 C.F.R. 438.10(h)(4)), while MA has not. The
Office of Management and Budget (OMB) defines "machine readable" as a format in a standard
computer language (not English text) that can be read automatically by a web browser or
computer system.
We received a number of comments in support of harmonizing the provider directory
requirements across CMS programs. We received mixed comments regarding the additional data
elements that were identified. We will continue to review and consider additional data elements
in the future. As this is only a best practice at this time, we will share this information with our
counterparts who work on the QHPs and Medicaid requirements.
Regulatory updates to § 422.111 would generally be needed to require MA organizations to issue
provider directories that include the additional elements. CMS intends to propose such revisions
in the future and encourages the inclusion of the elements listed below in provider directory
requirements as a best practice and urges MAOs to incorporate them into their production of
such directories in advance of future rulemaking.
158
The following are the provider directory data elements we believe are appropriate to use in
current MAOs’ provider directories:
Machine readable content
Provider medical group
Provider institutional affiliation
Non-English languages spoken by provider
Provider website address
Accessibility for people with physical disabilities
We received a number of comments regarding machine readability, with commenters requesting
additional information and some requesting CMS select a standard for machine readability.
Since machine readability is currently a best practice for Medicare Advantage, CMS urges the
industry to look to the guidance provided by the QHPs and Medicaid to strengthen oversight
processes, as well as to identify a standardized format for machine readable information.
We recognize that MAO customer service call centers use a variety of approaches to address
calls from enrollees who need assistance in locating a provider that is accepting new patients.
We also understand that there is no single approach that can be used for all calls or situations.
To further augment the customer service experience, we are encouraging MAOs institute the best
practice of incorporating a “warm transfer” policy to their customer service call when practical.
For enrollees calling to request help finding a provider that is accepting new patients, the CSR
would close the call by calling the provider’s office, establishing the need(s) of the enrollee, and
transferring the enrollee to the provider’s office to complete the appointment process. When
determining if a warm transfer should be used, the MAO should guard against steering by
providing the enrollee with choices of providers and to provide any needed materials/resources
to aid in provider selection, the MAO should consider the time of the call and the likelihood of
the provider’s office being available, and most importantly, the MAO should determine if the
enrollee would like to be transferred to the providers office.
Overview of CY 2017 Benefits and Bid Review
Portions of this guidance apply to cost-based plans and MA plans (including EGWPs, Dual-
Eligible Special Needs Plans (D-SNPs), Chronic Care Special Needs Plans (C-SNPs), and
Institutional Special Needs Plans (I-SNPs)). We currently do not evaluate whether employer
group plans, D-SNPs, and 1876 Cost Plans are duplicative under §422.256(b)(4), also referred to
as the “meaningful difference” evaluation. Similarly, employer group plans and 1876 Cost Plans
are not evaluated for low enrollment under §422.506(b)(1)(iv) and (b)(2). CMS reserves the
right to review employer group plans for low enrollment and/or meaningful difference in future
years.
159
Medicare-Medicaid Plans in Capitated Financial Alignment Demonstrations are not subject to
the review criteria summarized in the table below and benefits and benefit review guidance for
these plans will be provided separately.
CMS makes all of the necessary tools and information available to MAOs in advance of the bid
submission deadline, and therefore expects all MAOs to submit their best, accurate, and
complete bid(s) on or before the Monday, June 6, 2016 deadline. Any organization whose bid
fails the published Part C Service Category Cost Sharing, PMPM Actuarial Equivalent Cost
Sharing, Meaningful Difference, Total Beneficiary Cost (TBC), and/or Optional Supplemental
Benefit requirements at any time prior to final approval will receive a compliance notice, even if
the organization is allowed to correct the deficiency. The severity of compliance notice may
depend on the type and/or severity of errors.
IMPORTANT NOTE: As indicated in the Rate Announcement, CMS has adopted the proposal
to waive MA employer bidding requirements beginning in CY 2017. Although this change
affects CMS’ ability to evaluate the PMPM Actuarial Equivalent Cost Sharing discussed in this
section, MA employer plans continue to be subject to all unwaived MA requirements regardless
of whether they are evaluated as part of bid review or reviewed in connection with other
oversight. Employer plans will not be submitting a Bid Pricing Tool (BPT), but must submit a
Plan Benefit Package (PBP) in accordance with CMS requirements (consistent with past years)
and make a good faith effort in projecting CY 2017 member months for each plan and place the
amount in Section A-2 of the PBP. Please see “Plan Benefit Package (PBP) Updates and
Guidance” of this Call Letter for additional information.
The following chart displays key MA bid review criteria and identifies which criteria are used in
reviewing the bids of the plan types identified in the column headings.

160
Table 13. Plan Types and Applicable Bid Review Criteria
Bid Review Criteria
Applies to Non-
Employer Plans
(Excluding Dual
Eligible SNPs)
Applies to
Non-Employer
Dual Eligible
SNPs
Applies to
1876 Cost
Plans
Applies to
Employer
Plans
Low Enrollment
Yes
Yes
No
No
Meaningful Difference
Yes
No
No
No
Total Beneficiary Cost
Yes
No
No
No
Maximum Out-of –
Pocket (MOOP) Limits
Yes
Yes
No
Yes
PMPM Actuarial
Equivalent Cost
Sharing
Yes
Yes
No
Yes
Service Category Cost
Sharing
Yes
Yes
Yes
1
Yes
Part C Optional
Supplemental Benefits
Yes
Yes
No
No
1
Section 1876 Cost Plans and MA plans may not charge enrollees higher cost sharing than is charged under Original Medicare
for chemotherapy administration, skilled nursing care and renal dialysis services (42 CFR §§417.454(e) and 422.100(j)).
CMS has made changes to service category cost sharing amounts, PMPM Actuarial Equivalence
factors, and Total Beneficiary Cost (TBC) requirements for CY 2017 and have provided these
changes in each applicable section below. Consistent with past years, MAOs must also address
requirements implemented under the Affordable Care Act, such as the medical loss ratio and
health insurance providers fee, and are expected to do so independently of our requirements for
benefits or bid review. Therefore, we are not making specific adjustments or allowances for
these changes in the benefits review requirements.
Plans with Low Enrollment
At the end of March, CMS sent affected MAOs a list of non-SNP plans that have fewer than 500
enrollees or fewer than 100 enrollees for SNP plans and that have been in existence for three or
more years [as of March 2016 (three annual election periods)]. The notification represents CMS’
decision not to renew such plans under 42 CFR §422.506(b)(1)(iv) and (b)(2). The list did not
include plans with low enrollment that CMS determines are located in service areas that do not

161
have a sufficient number of competing options of the same plan type (such that the low
enrollment plan still represents a viable plan option for enrollees).
Through return e-mail, MAOs must either (1) confirm that each of the low enrollment plans
identified by CMS will be eliminated or consolidated with another of the organization’s plans for
CY 2017, or (2) provide a justification for renewal. If CMS does not find a unique or compelling
reason that the low enrollment plan is a viable independent option for enrollees, CMS will
instruct the organization to eliminate or consolidate the plan. Instructions and the timeframe for
submitting business cases and the information required in those submissions were included with
the list of low enrollment plans sent to the MAO.
Note: These requirements do not apply to Section 1876 cost plans, employer plans, or MA
Medical Savings Account (MSA) plans.
CMS recognizes there may be certain factors, such as the specific populations served and
geographic location of the plan, that lead to a plan’s low enrollment. SNPs, for example, may
legitimately have low enrollments because they focus on a subset of enrollees with certain
medical conditions. CMS will consider this information when evaluating whether specific plans
should be non-renewed based on insufficient enrollment. MAOs should follow CMS
renewal/non-renewal guidance (see the Medicare Managed Care Manual: section 150 of Chapter
4, and/or section 60.2 of Chapter 16B) to determine whether a low enrollment plan may be
consolidated with another plan(s). CMS will continue to evaluate and implement low enrollment
requirements on an annual basis.
CMS received comments expressing concerns about applying low enrollment restrictions to
employer plans in the future. Although CMS does not intend to apply low enrollment criteria to
employer plans in CY 2017, we will consider in the future how to apply the applicable standard
(that the “plan does not have a sufficient number of enrollees to establish that it is a viable
independent plan option”) to employer plans and whether to take enforcement action in that
context.
Meaningful Difference (Substantially Duplicative Plan Offerings)
Pursuant to §422.254(a)(4), MAOs offering more than one plan in a given service area must
guarantee the plans are substantially different so that beneficiaries can easily identify the
differences between those plans in order to determine which plan provides the highest value at
the lowest cost to address their needs. For CY 2017, CMS will use plan-specific per member per
month (PMPM) out-of-pocket cost (OOPC) estimates to identify meaningful differences in
beneficiary costs among the same plan types. For CY 2017, benefits and the reduction in cost
sharing that are offered as part of the Value-Based Insurance Design (VBID) model test will not
be included in the meaningful difference evaluation. Documentation and instructions for the
OOPC model are available at: https://www.cms.gov/Medicare/Prescription-Drug-Coverage/
PrescriptionDrugCovGenIn/OOPCResources.html.
162
CMS considers HMO and HMO-POS as one plan type, unless the HMO-POS plan covers all
Parts A and B services outside the network, in which case the HMO-POS plan is considered
meaningfully different from the HMO plan. Consistent with CY 2016, this standard for
evaluating meaningful difference will not include geographic or provider limitations on the out-
of-network benefits. However, CMS in future years may consider HMO-POS plans
meaningfully different only if the plans do not place geographic or provider limitations on the
out-of-network benefits.
We received several comments recommending that CMS not move forward with further
restrictions on HMO-POS plans in the future. CMS will take these comments into consideration
as part of our ability to interpret and apply the meaningful difference regulatory requirement in
the future.
For CY 2017, CMS will evaluate meaningful differences among CY 2017 non-employer and
non-cost contractor plans offered by the same MAO, in the same county and, under the same
contract, as follows:
1. The MAO’s plan offerings will be separated into five plan type groups on a county basis:
(1) HMO and HMO-POS not offering all Parts A and B services out-of-network; (2)
HMO POS offering all Parts A and B services out-of-network; (3) Local PPO; (4)
Regional PPO; and (5) PFFS.
2. SNP plan offerings will be further separated into groups representing the specific target
populations served by the SNP. Chronic Care SNPs will be separated by the chronic
disease served and Institutional SNPs will be separated into the following three
categories: Institutional (Facility); Institutional Equivalent (Living in the Community);
and a combination of Institutional (Facility) and Institutional Equivalent (Living in the
Community). We currently do not apply the meaningful difference evaluation to D-
SNPs.
3. Plans within each plan type group will be further divided into MA-only and MA-PD sub-
groups for evaluation. That is, the presence or absence of a Part D benefit is considered a
meaningful difference.
4. The OOPC (Part C and Part D) PMPM estimate will be calculated for each plan. CMS
considers a difference of at least $20.00 PMPM between the OOPC for each plan offered
by the same MAO in the same county to be meaningful for purposes of applying the
meaningfully different standard.
CMS is considering whether to conduct this evaluation at either the legal entity or parent
organization level in future years. We received several comments recommending that CMS not
move forward with this approach in future years due to the potential restrictions it could place on
organizations and the benefits offered to the enrollees. CMS will take these comments into
163
consideration as part of our ability to interpret and apply the meaningful difference regulatory
requirement in the future.
Note that plan characteristics such as premium, variations in provider networks, and/or serving
different populations are not considered meaningfully different characteristics. Commenters
requested CMS to consider allowing premium and/or provider network differences as part of
their meaningful difference evaluation. We will continue to consider these comments, but will
maintain our current position. Premium is excluded from the criteria because the regulatory
meaningful difference requirement is intended to be an objective measure of benefits between
two plans; the inclusion of premium would introduce risk selection, costs, and margin into the
evaluation, resulting in a negation of the evaluation’s objectivity. Provider network differences
have also been excluded from our criteria because having a provider in one plan and not the
other is not a change in benefit coverage. In addition, plan providers can change throughout the
year (e.g., terminate their provider contract or close their practice to new members), so it is not
necessarily accurate or transparent to a beneficiary making a plan choice for the year.
CMS expects MAOs to submit CY 2017 plan bids that meet the meaningful difference standards,
but will not prescribe how the MAOs should redesign benefit packages to achieve the
differences. Furthermore, MAOs will have access to the necessary tools to calculate OOPC
estimates for each plan prior to bid submission. CMS will not approve plan bids that do not meet
these standards.
CMS notes that meaningful difference will be evaluated based on the "as submitted formulary"
prior to rebate reallocation, and "first approved formulary" following rebate reallocation. MAOs
must follow the CY 2017 renewal/non-renewal guidance in the Final Call Letter to determine if
their plans may be consolidated with other plans.
NOTE: Please see Plan Benefit Package (PBP) and policy updates below for changes to PBP that
may impact the OOPC model and could potentially affect the meaningful difference evaluation
for certain plans.
Total Beneficiary Cost (TBC)
CMS will exercise its authority under section 1854(a)(5)(C)(ii) of the Act to deny MAO bids, on
a case-by-case basis, if it determines the bid proposes too significant an increase in cost sharing
or decrease in benefits from one plan year to the next through the use of the TBC standard. A
plan’s TBC is the sum of the plan-specific Part B premium, plan premium, and estimated
beneficiary out-of-pocket costs. The change in TBC from one year to the next captures the
combined financial impact of premium changes and benefit design changes (i.e., cost sharing
changes) on plan enrollees; an increase in TBC is indicative of a reduction in benefits. By
limiting excessive increases in the TBC from one year to the next, CMS is able to confirm
enrollees who continue enrollment in the same plan are not exposed to significant cost increases.
As in past years, CMS will evaluate TBC for non-employer plans (excluding D-SNPs). For CY
164
2017, benefits and cost sharing that are offered as part of the Value-Based Insurance Design
(VBID) model test will not be included in the TBC evaluation. The MA plans that are
participating in the VBID model test will be evaluated under the TBC calculation, including plan
premium and non-VBID benefits and cost sharing.
Under §422.254, CMS reserves the right to further examine and request changes to a plan bid
even if a plan’s TBC is within the required amount. This approach not only protects enrollees
from significant increases in cost sharing or decreases in benefits, but also confirms enrollees
have access to viable and sustainable MA plan offerings.
CMS has focused on sharing information with and providing transparency to the MAOs as it
relates to the TBC year-to-year evaluation. CMS proposed to modify the payment adjustment in
a different way than indicated in the CY 2016 Final Call Letter. Rather than “discounting” the
plan-specific payment adjustment (including a coding intensity component), CMS proposed to
eliminate the coding intensity adjustment factor. Since most of the Affordable Care Act (ACA)
payment changes have been implemented, it is our expectation that MAOs are better positioned
to share payment changes and provide affordable and effective benefits for beneficiaries. Going
forward, the payment adjustment in the TBC calculation will account for changes in county
benchmarks, quality bonus payment, and/or rebate percentages.
CMS received comments from several organizations opposed to this change in interpretation and
implementation because future coding intensity and other rate pressures are unknown and could
result in unanticipated revenue pressure. Some commenters suggested CMS should keep the
coding intensity adjustment and also include an adjustment for changes in the risk score model to
provide greater flexibility in modifying benefits. Other comments supported our proposal since
most of the ACA payment changes have been implemented and MAOs should be positioned to
share in payment changes. We appreciate the comments and will move forward with eliminating
the coding intensity adjustment factor as part of our TBC analysis for CY 2017.
Other comments suggested giving consideration to indexing the TBC change amount to account
for annual medical inflation and that Institutional SNPs may warrant special consideration in
applying the TBC evaluation. We will give consideration to these suggestions as policy and
guidance is developed for CY 2018.
In addition, we received comments concerned about expectations related to the Health Insurance
Providers Fee moratorium as bids are prepared for CY 2017 and its year-to-year impact on the
TBC evaluation. Consistent with past years, MAOs must address requirements implemented
under the ACA, such as the medical loss ratio and health insurance providers fee, and are
expected to do so independently of our requirements for benefits or bid review. Therefore, we
are not making specific adjustments or allowances for these changes in the benefits review
requirements.
165
CMS will continue to incorporate the technical and payment adjustments described below and
expect organizations to address other factors, such as coding intensity changes, risk adjustment
model changes and payment of the health insurance provider’s fee independently of our TBC
requirement. As such, plans are expected to anticipate and manage changes in payment and
other environmental factors to minimize changes in benefit and cost sharing over time. CMS
also reminds MAOs that the Office of the Actuary extends flexibility on margin requirements so
MAOs can satisfy the TBC requirement.
In mid-April 2016, as in past years, CMS will provide plan specific CY 2016 TBC values and
the following adjustments that are incorporated in the TBC calculation to account for changes
from one year to the next:
Technical Adjustments: (1) annual changes in OOPC model software and (2) maximum
Part B premium buy-down amount change in the bid pricing tool, if applicable (no
change for CY 2017).
Payment Adjustments: (1) county benchmark, and (2) quality bonus payment and/or
rebate percentages.
CMS will maintain the TBC change threshold at $32.00 PMPM for CY 2017. A plan
experiencing a net increase in adjustments must have an effective TBC change amount below the
$32.00 PMPM threshold to avoid denial of the bid under section 1854(a)(5)(C)(ii). Conversely,
a plan experiencing a net decrease in adjustments may have an effective TBC change amount
above the $32.00 PMPM threshold. In an effort to support plans that improve quality
compensation and experience large payment adjustments, along with holding plans accountable
for lower quality, CMS will apply the TBC evaluation as follows.
For CY 2017, the TBC change evaluation will be treated differently for the following specific
situations:
Plans with an increase in quality bonus payment and/or rebate percentage, and an overall
payment adjustment amount greater than $32.00 PMPM will have a TBC change
threshold of $0.00 PMPM (i.e., −1 times the TBC change limit of $32 PMPM) plus
applicable technical adjustments.
Plans with a decrease in quality bonus payments and/or rebate percentage, and an overall
payment adjustment amount less than -$32.00 PMPM will have a TBC change threshold
of $64.00 PMPM (i.e., 2 times TBC change limit of $32.00 PMPM) plus applicable
technical adjustments. That is, plans would not be allowed to make changes that result in
greater than $64.00 worth of decreased benefits or increased premiums.
Plans with a star rating below 3.0 and an overall payment adjustment amount less than
−$32.00 PMPM will have a TBC change threshold of $64.00 PMPM (i.e., 2 times TBC
166
change limit of $32.00) plus applicable technical adjustments.
Plans not accounted for in the three specific situations above will be evaluated at the $32
PMPM limit, similar to last year.
CMS received feedback subsequent to last year’s Call Letter suggesting that CMS make changes
to the TBC evaluation for Special Needs Plans for End Stage Renal Disease (ESRD), which are
subject to larger increases and/or decreases in payment amounts. To moderate potentially large
payment changes and provide MAOs with the ability to maintain benefit stability year-to-year,
while helping provide protection for this vulnerable beneficiary population, CMS proposed this
year to apply limits to the payment adjustment for ESRD plans as described below:
Plans with an increase in the overall payment adjustment amount greater than $32.00
PMPM will have a TBC change threshold of $0.00 PMPM (i.e., −1 times the TBC
change limit of $32 PMPM) plus applicable technical adjustments.
Plans with a decrease in the overall payment adjustment amount less than -$32.00
PMPM will have a TBC change threshold of $64.00 PMPM (i.e., 2 times TBC change
limit of $32.00 PMPM) plus applicable technical adjustments. That is, plans would not
be allowed to make changes that result in greater than $64.00 worth of decreased
benefits or increased premiums.
We received comments acknowledging CMS’s efforts to address the TBC challenges facing
ESRD plans, but expressing concern that the proposed changes may not go far enough in
managing the potential impact of ESRD payment changes. Some commenters recommended a
separate TBC evaluation for ESRD plans. We understand that organizations may have concerns
related to this limitation when payments are decreasing, but are finalizing this guidance for CY
2017. CMS will monitor and evaluate potential modifications for CY 2018.
Consistent with the CY 2016 Final Call Letter, CMS proposed that each individual plan being
consolidated into another plan must meet the TBC requirement on its own merit. For CY 2017,
CMS will be moving forward with this interpretation and implementation; therefore,
organizations consolidating multiple plans into a single plan will no longer be permitted to use
the enrollment-weighted average TBC change of the consolidating plans.
We received comments from several organizations expressing concerns because multiple plans
may need to be consolidated due to organizational or marketplace changes, as well as CMS
pressures. Commenters pointed out that if plans were unable to meet this requirement, it could
result in disruption for beneficiaries. CMS is finalizing this approach for CY 2017 as it affords
greater protection for beneficiaries and enrollees in non-renewing plans will be able to actively
select another MA plan from the same or competing organization based on CMS non-renewal
guidance.

167
NOTE: Please see policy updates below for changes to the PBP that will impact the OOPC
model and may potentially affect the TBC evaluation for certain plans.
Maximum Out-of-Pocket (MOOP) Limits
As codified at 42 CFR §422.100(f)(4) and (5) and §422.101(d)(2) and (3), all MA plans,
including employer group plans and SNPs, must establish limits on enrollee out-of-pocket
spending that do not exceed the annual maximum amounts set by CMS. Although the MOOP
requirement is for Parts A and B services, an MAO can include supplemental benefits as services
subject to the MOOP. MA plans may establish as their MOOP any amount within the ranges
shown in the table.
Table 14 below displays the CY 2017 mandatory and voluntary MOOP amounts and the
combined (catastrophic) MOOP amount limits applicable to Local PPOs and Regional PPOs. A
plan’s adoption of a MOOP limit that qualifies as a voluntary MOOP ($0 - $3,400) results in
greater flexibility for individual service category cost sharing. We chose to display the possible
ranges of the MOOP amount within each plan type in order to illustrate that MOOP limits may
be lower than the CMS-established maximum amounts and what MOOP amounts qualify as
mandatory and voluntary MOOP limits.
Table 14. CY 2017 Voluntary and Mandatory MOOP Range Amounts by Plan Type
Plan Type
Voluntary
Mandatory
HMO
$0 - $3,400
$3,401 - $6,700
HMO POS
$0 - $3,400 In-network
$3,401 - $6,700 In-network
Local PPO
$0 - $3,400 In-network and
$0 -$5,100 Combined
$3,401 - $6,700 In-network and
$3,401 - $10,000 Combined
Regional PPO
$0 - $3,400 In-network and
$0 - $5,100 Combined
$3,401 - $6,700 In-network and
$3,401 - $10,000 Combined
PFFS (full
network)
$0 - $3,400 Combined
$3,401 - $6,700 Combined
PFFS (partial
network)
$0 - $3,400 Combined
$3,401 - $6,700 Combined
PFFS (non-
network)
$0 - $3,400
$3,401 - $6,700
168
We received a comment requesting clarification as to whether PPOs are permitted to offer a
combined MOOP amount within the mandatory range, while having an in-network MOOP
amount within the voluntary range. Although we will take this comment under consideration for
the future, CMS’s current policy is that the in-network MOOP amount dictates the combined
MOOP range for PPOs. The MOOP ranges stated in the Call Letter above are accurate.
As explained in the CY 2012 Call Letter, MOOP limits are based on a beneficiary-level
distribution of Parts A and B cost sharing for individuals enrolled in Original Medicare. The
mandatory MOOP amount represented approximately the 95th percentile of projected
beneficiary out-of-pocket spending. Stated differently, five percent of Original Medicare
beneficiaries are expected to incur approximately $6,700 or more in Parts A and B deductibles,
copayments and coinsurance. The voluntary MOOP amount of $3,400 represents approximately
the 85th percentile of projected Original Medicare out-of-pocket costs.
The Office of the Actuary conducts an annual analysis to help CMS determine the proposed
MOOP amount. Since the MOOP requirement was finalized in §422.100(f)(4) and (5), a strict
application of the 95th and 85th percentile would have resulted in MOOP limits fluctuating up
and down year-to-year. CMS has exercised discretion to maintain stable MOOP limits from
year-to-year, if the beneficiary-level distribution of Parts A and B cost sharing for individuals
enrolled in Original Medicare is approximately equal to the appropriate percentile. This
approach avoids enrollee confusion, allows plans to provide stable benefit packages, and does
not discourage the adoption of the lower voluntary MOOP amount if the limit increases one year
and then decreases the next. CMS expects to increase MOOP limits if a consistent pattern of
increasing costs emerges over a period of time.
Although it may be rare that a dual-eligible enrollee would be responsible for paying any cost
sharing (because the State Medicaid program is making those payments on his/her behalf), all
MA plans must track enrollees’ actual out-of-pocket spending for covered services in order to
make certain an enrollee does not spend more than the MOOP amount limit established by the
plan. If the plan charges cost sharing for covered services, some dual-eligible enrollees may
incur cost sharing and any enrollee losing his/her Medicaid eligibility would be responsible for
cost sharing. D-SNPs have the flexibility to establish $0 as the MOOP amount, thereby
guaranteeing there is no cost sharing for plan enrollees, including those who are liable for
Medicare cost sharing. Otherwise, if the D-SNP does charge cost sharing for Medicare covered
or non-covered services, it must track enrollees’ out-of-pocket spending and it is up to the plan to
develop the process and vehicle for doing so.
Per Member Per Month (PMPM) Actuarial Equivalent (AE) Cost Sharing Limits
IMPORTANT NOTE: As indicated in the Rate Announcement, CMS has adopted the proposal
to waive MA employer bidding requirements beginning in CY 2017. Although this change
affects CMS’ ability to evaluate the PMPM Actuarial Equivalent Cost Sharing discussed in this
169
section, MA employer plans continue to be subject to all unwaived MA regulatory requirements
whether they are evaluated as part of bid review or reviewed in connection with other oversight.
Total MA cost sharing for Parts A and B services must not exceed cost sharing for those services
in Original Medicare on an actuarially equivalent basis. See 42 CFR §422.254(b)(4). CMS will
apply this requirement separately to the following service categories for CY 2017: Inpatient,
Skilled Nursing Facility (SNF), Durable Medical Equipment (DME), and Part B drugs. Please
note that factors for Inpatient and SNF in Column 4 of the table below (Part B Adjustment Factor
to Incorporate Part B Cost Sharing) have been updated for CY 2017.
Whether in the aggregate, or on a service-specific basis, excess cost sharing is identified by
comparing two values found in Worksheet 4 of the BPT. Specifically, a plan’s PMPM cost
sharing for Medicare covered services (BPT Worksheet 4, Section IIA, column l) is compared to
Original Medicare Actuarially Equivalent Cost Sharing (BPT Worksheet 4, Section IIA, column
n). For Inpatient and SNF services, the AE Original Medicare cost sharing values, unlike plan
cost sharing values, do not include Part B cost sharing; therefore, an adjustment factor is applied
to these AE Original Medicare values to incorporate Part B cost sharing and to make the
comparison valid.
Once the comparison amounts have been determined, excess cost sharing can be identified.
Excess cost sharing is the difference (if positive) between the plan cost sharing amount (column
#1) and the comparison amount (column #5). The chart below uses illustrative values to
demonstrate the mechanics of this determination.

170
Table 15. Illustrative Comparison of Service-Level Actuarial Equivalent Costs to Identify
Excessive Cost Sharing
#1
#2
#3
#4
#5
#6
#7
BPT
Benefit
Category
PMPM
Plan
Cost
Sharing
Original
Medicare
Allowed
Original
Medicare
AE Cost
sharing
Part B
Adjustment
Factor to
Incorporate
Part B Cost
Sharing
Comparison
Amount
Excess
Cost
Sharing
Pass/Fail
(Parts
A&B)
(Based on
FFS data)
(BPT
Col. l)
(BPT
Col. m)
(BPT
Col. n)
1
(#3 × #4)
(#1 −
#5, min
of $0)
Inpatient
$33.49
$331.06
$25.30
1.382
$34.97
$0.00
Pass
SNF
$10.83
$58.19
$9.89
1.069
$10.58
$0.25
Fail
DME
$3.00
$11.37
$2.65
1
$2.65
$0.35
Fail
Part B-
Rx
$0.06
$1.42
$0.33
1
$0.33
$0.00
Pass
1
PMPM values in column 3 for Inpatient and Skilled Nursing Facility only reflect Part A fee-for-service actuarial equivalent cost
sharing for that service category.
Part C Cost Sharing Standards
For CY 2017, CMS will continue the current policy of affording MA plans greater flexibility in
establishing Parts A and B cost sharing by adopting a lower voluntary MOOP limit than is
available to plans that adopt a higher, mandatory MOOP limit. Table 16 below summarizes the
standards and cost sharing amounts by MOOP type (e.g., mandatory or voluntary) for local and
regional MA plans that we will not consider discriminatory or in violation of other applicable
standards. CY 2017 bids must reflect enrollee cost sharing for in-network services no greater
than the amounts displayed below. For LPPOs and RPPOs, these standards will be applied only
to in-network services. All standards and cost sharing are inclusive of applicable service
category deductibles, copayments and coinsurance, but do not include plan level deductibles.
Inpatient standards have been updated to reflect estimated changes in Original Medicare cost for
CY 2017.

171
Table 16. CY 2017 In-Network Service Category Cost Sharing Requirements
Cost Sharing Limits
Service Category
PBP Section B data
entry field
Voluntary
MOOP
Mandatory
MOOP
Inpatient - 60 days
1a
N/A
$4,177
Inpatient - 10 days
1a
$2,471
$1,977
Inpatient - 6 days
1a
$2,251
$1,801
Mental Health Inpatient - 60 days
1b
$2,606
$2,085
Mental Health Inpatient - 15 days
1b
$1,988
$1,590
Skilled Nursing Facility – First 20 Days
1
2a
$20/day
$0/day
Skilled Nursing Facility – Days 21 through 100
2
2a
$164.50/day
$164.50/day
Emergency Care/Post Stabilization Care
4a
$75
$75
Urgently Needed Services
3
4b
$65
$65
Partial Hospitalization
5
$55/day
$55/day
Home Health
6a
20% or $35
$0
Primary Care Physician
7a
$35
$35
Chiropractic Care
7b
$20
$20
Occupational Therapy
7c
$40
$40
Physician Specialist
7d
$50
$50
Psychiatric and Mental Health Specialty Services
7e and 7h
$40
$40
Physical Therapy and Speech-language Pathology
7i
$40
$40
Therapeutic Radiological Services
8b
20% or $60
20% or $60
DME-Equipment
11a
N/A
20%
DME-Prosthetics
11b
N/A
20%
DME-Medical Supplies
11b
N/A
20%
DME-Diabetes Monitoring Supplies
11c
N/A
20% or $10
DME-Diabetic Shoes or Inserts
11c
N/A
20% or $10
Dialysis Services
12
20% or $30
20% or $30
Part B Drugs-Chemotherapy
4
15
20% or $75
20% or $75
Part B Drugs-Other
15
20% or $50
20% or $50
1
MA plans and 1876 Cost Plans may not charge enrollees higher cost sharing than is charged under Original Medicare for
chemotherapy administration, skilled nursing care and renal dialysis services (42 CFR §§417.454(e) and 422.100(j)).
2
MA plans may have cost sharing for the first 20 days of a SNF stay. The per-day cost sharing for days 21 through 100 must not
be greater than the Original Medicare SNF amount. Total cost sharing for the overall SNF benefit must be no higher than the
actuarially equivalent cost sharing in Original Medicare, pursuant to §1852(a)(1)(B).
3
Emergency Care and Urgently Needed Care benefits are not subject to plan level deductible amount and/or out-of-network
providers.
4
Part B Drugs - Chemotherapy cost sharing displayed is for services provided on an outpatient basis and includes administration
services. MAOs have the option to charge either coinsurance or a copayment for most service category benefits. For example,
based on the cost sharing requirements indicated above for Part B Drugs – Chemotherapy, a plan can choose to either assign up
to a 20% coinsurance or $75 copayment to that particular benefit.
172
MAOs with benefit designs that use a coinsurance or copayment amount for which CMS does
not have an established amount (e.g., coinsurance for inpatient or copayment for durable medical
equipment) must submit documentation with their initial bid that clearly demonstrates how the
coinsurance or copayment amount satisfies CMS service category requirements. This
documentation must be submitted under the “cost sharing justification upload” section in the Bid
Submission module of HPMS (Navigation Path: Plan Bids > Bid Submission > CY 2017 >
Substantiation > Select Applicable Contract Number). CMS annually evaluates available
Medicare data and other information to apply MA requirements in accordance with applicable
law. Organizations are afforded the flexibility to design their benefits as they see fit so long as
they satisfy Medicare coverage requirements.
As indicated in the table above, for SNF days 1 through 20, CMS will reduce the cost sharing
limit for CY 2017 voluntary MOOP plans from $40 per day to $20 per day for beneficiary
protection. In addition, we also intend to reduce the cost sharing limit from $20 per day to $0
per day for CY 2018 MA plans so that SNF cost sharing will align with Original Medicare for
both voluntary and mandatory MOOP. We received comments from organizations in support of
this change because it aligns with Original Medicare and helps vulnerable beneficiaries
experiencing health care challenges, while other commenters expressed concerns about limiting
benefit flexibility. CMS appreciates these comments and is finalizing the change for CY 2017
and expects to make the proposed change for CY 2018.
CMS has traditionally afforded MAOs greater flexibility in establishing Parts A and B cost
sharing by adopting a lower, voluntary maximum out-of-pocket (MOOP) limit than is available
to plans that adopt a higher, mandatory MOOP limit. The number of MA plans with voluntary
MOOPs has decreased significantly over the past several years which may call into question the
value of allowing cost sharing flexibility and serve to minimize the impact of changes made to
this policy.
CMS requested comments about whether current cost sharing flexibility should still be available
to voluntary MOOP plans, and suggestions about other incentives to encourage MAOs to offer
plans with a lower voluntary MOOP for enrollees. For example, flexibilities to highlight
voluntary MOOP plans in marketing materials or a special indicator or priority sorting on
Medicare Plan Finder. These types of marketing-related incentives may encourage plans and
brokers to educate beneficiaries on the MOOP and its value to their overall financial protection
should they experience large medical expenses during a plan year.
Most commenters recommended that CMS continue to provide benefit flexibility so that
organizations would be encouraged to offer voluntary MOOP plans and also provided helpful
suggestions. For example, expanding the benefit flexibility to other categories, modifying both
the voluntary and mandatory MOOP amounts, providing potential marketing and/or preferential
treatment on Medicare Plan Finder. Some commenters supported efforts to limit high cost
173
sharing, but did not want plans to be discouraged from offering plans with lower MOOP amounts
which affords greater beneficiary protection.
We appreciate these comments and expect to continue cost sharing flexibility for voluntary
MOOP plans. CMS will consider expanding benefit flexibility to additional service categories,
adjusting MOOP amounts, and providing additional marketing and Medicare Plan Finder
incentives. However, the difference in cost sharing limits between a voluntary MOOP and
mandatory MOOP plan may be reduced somewhat to balance concerns about potentially
discriminatory benefit designs.
We received comments about increasing the limits for certain services (e.g., emergency care),
decreasing limits for certain services (e.g., physical therapy and speech-language pathology
services), and publishing limits for services that CMS communicated with organizations about
potentially high cost sharing (e.g., cardiac and pulmonary rehabilitation services). We also
received a comment expressing concern about having separate categories for mental health and
non-mental health benefits in the plan benefit package (PBP) and separate service category cost
sharing requirements.
MA plans may not charge enrollees higher cost sharing than is charged under Original Medicare
for chemotherapy administration, skilled nursing care and renal dialysis services (42 CFR
§422.100(j)). Although CMS has not established a specific service category cost sharing limit
for all possible services in the Call Letter, MA plans may not pay less than 50% of the contracted
(or Medicare allowable) rate and cost sharing for services cannot exceed 50% of the total MA
plan financial liability for the benefit. If a plan uses a copayment method of cost sharing, then
the copayment for an in-network Original Medicare service category cannot exceed 50% of the
average contracted rate of that service (Medicare Managed Care Manual, Chapter 4, Section
50.1). Organizations typically have much lower cost sharing for enrollees than this requirement
due to effective managed care principles, effective negotiations between organizations and
providers, and competition.
MAOs are not permitted to design “benefits to discriminate against beneficiaries, promote
discrimination, discourage enrollment or encourage disenrollment, steer subsets of Medicare
beneficiaries to particular MA plans, or inhibit access to services” (42 CFR §422.100(f)(2)).
CMS evaluates bid and marketplace data to identify areas of concern, conducts research, and
may add service category cost sharing limits in the future based on these analyses. For example,
cardiac and pulmonary rehabilitation services are areas of concern that we continue to monitor,
and we will ask MA organizations to provide justification for cost sharing above the following
amounts for CY 2017 benefit designs as part of bid review:
Cardiac Rehabilitation Services: $50
Intensive Cardiac Rehabilitation Services: $100

174
Pulmonary Rehabilitation Services: $30
CMS recognizes that mental health services may have a different cost structure than non-mental
health services which is reflected in the plan benefit package (PBP) by having different
categories. PBP documentation defines the differences between these categories and
organizations have the flexibility to use reasonable methods to distinguish between mental health
and non-mental health services.
Part C Optional Supplemental Benefits
As part of our evaluation whether the bid and benefits are not discriminatory against enrollees
with specific (or high cost) health needs, CMS will continue to review non-employer bid
submissions to verify enrollees electing optional supplemental benefits are receiving reasonable
value. As in CY 2016, CMS considers a plan to be not discriminatory when the total value of all
optional supplemental benefits offered to non-employer plans under each contract meets the
following thresholds: (a) the enrollment-weighted contract-level projected gain/loss margin, as
measured by a percent of premium, is no greater than 15% and (b) the sum of the enrollment-
weighted contract-level projected gain/loss margin and non-benefit expenses, as measured by a
percent of premium, is no greater than 30%.
CMS understands some supplemental benefits are based on a multi-year basis, but the plan bids
submitted each year are evaluated based on that particular plan year.
Plan Benefit Package (PBP) Updates and Guidance
Projected Member Months
As indicated in the Rate Announcement, CMS has adopted the proposal to waive MA employer
bidding requirements beginning in CY 2017. Employer plans will not be submitting a MA or
Part D Bid Pricing Tool (BPT), but must complete and submit a Plan Benefit Package (PBP) in
accordance with CMS requirements (consistent with past years). Organizations should make a
good faith effort in projecting CY 2017 member months for each plan and place the amount in
Section A-2 of the PBP. The following question must be completed for all MA and 1876 Cost
Plan organizations that do not submit a Bid Pricing Tool (BPT): “Indicate CY 2017 total
projected member months for this plan.”
Medical Services Performed in Multiple Health Care Settings
In our continuing effort to avoid duplication of medical services entered in the PBP, CMS is
offering additional guidance on how to place services that can be performed in different health
care settings (e.g., physician office, outpatient hospital, and free standing facility) in the
appropriate service category and correctly complete data entry within the PBP.
175
The outpatient hospital service category in the PBP has historically included a variety of services
that may have their own dedicated PBP category. By including the same service in multiple
locations throughout the PBP, we are concerned that marketing materials may be confusing and
that CMS cost sharing requirements could be compromised. Based on the out-of-pocket cost
(OOPC) model methodology, including services with zero cost sharing for the minimum amount
in a multiple service category will reduce the estimated out-of-pocket costs used by beneficiaries
in comparing plans on Medicare Plan Finder and adversely affect CMS bid review for
meaningful difference and Total Beneficiary Cost (TBC).
Our goal is to ultimately have PBP service categories reflect cost sharing for services provided in
different places of service. For example, Cardiac and Pulmonary Rehabilitation Services can be
administered in a number of health care settings including outpatient hospitals, free- standing
facilities, or a physician’s office. Instead of having these services appear in multiple PBP service
categories, we expect cost sharing for these services to appear only in PBP Service Category 3
(Cardiac and Pulmonary Rehabilitation Services). The minimum/maximum data fields allow
plans to reflect the varying cost sharing associated with different places of service, when needed.
The note for this service category will describe the cost sharing associated with the various
places of service and must be consistent with the data entry. Cardiac and Pulmonary
Rehabilitation Services in any other section of the PBP will not satisfy CMS requirements and
the organization will be asked to correct its bid submission.
Another area of particular concern is Medicare-covered preventive services. All Medicare-
covered zero dollar cost sharing preventive services must be included in PBP Service Category
14a and must not be included in any other service category (i.e., those benefits that are rated as A
or B by the United States Preventive Services Task Force). For example, we do not expect to see
a zero in the minimum data field in 9a (Outpatient hospital services) with a note that explains the
zero dollar amount is for preventive services. All of the zero dollar Medicare-covered preventive
services are to be placed in 14a only.
For CY 2016, plans were required to reflect cost sharing for the service categories listed in the
table below appropriately within each designated service category:

176
PBP Sec. B
Service Category
3
Cardiac and Pulmonary Rehabilitation Services
7a
Primary Care Physician Services
7d
Physician Specialist Services excluding Psychiatric Services
7f
Podiatry Services
9d
Outpatient Blood Services
11b
Prosthetics/Medical Supplies
12
Dialysis Services
14a
Medicare-Covered Zero Cost-Sharing Preventive Services
15
Medicare Part B Rx Drugs and Home Infusion Drugs
In addition to the service categories listed above, plans must enter cost sharing for the service
categories shown in the table below appropriately within each designated service category for
CY 2017. These services should not be referenced in any other service category. We anticipate
these changes will improve transparency and streamline the data entry so the cost sharing
associated with those PBP service categories below reflects the services provided across a
variety of healthcare settings.
PBP Sec. B
Service Category
7c
Occupational Therapy Services
7g
Other Health Care Professional Services
7i
Physical therapy and Speech Language Pathology Services
8a
Outpatient Diagnostic Procedures and Tests and Lab Services
8b
Outpatient Diagnostic and Therapeutic Radiological Services
9a
Outpatient Hospital Services
9b
Ambulatory Surgical Center Services (ASC)
CMS received several comments regarding PBP category B9a. One organization suggested this
service category be eliminated, while another commenter requested examples of services that

177
may be included in this category. Examples of services we expect to be identified under B9a in
the PBP include observation, outpatient palliative care, and outpatient surgical services (i.e.,
outpatient surgical services not provided in an Ambulatory Surgical Center as defined by
Original Medicare). We will continue to evaluate opportunities to streamline data entry and
avoid duplication in the PBP in the future.
We also received a comment requesting clarification on a service that may be related to more
than one PBP category during the same patient encounter. We do not expect a service to take
place in more than one service category during a patient encounter. For additional guidance
related to professional and facility fees being charged by providers during a patient encounter,
please refer to the section titled “Cost Sharing/Bundling and Facility.”
Medicare-Covered Preventive Services
In previous years, MAOs were able to include non-zero dollar Medicare-covered preventive
services in multiple service categories. CMS is modifying the PBP to rename B14a from
"Medicare-covered Preventive Services" to "Medicare-covered Zero Dollar Preventive Services,"
and will create a new service category where all other Medicare-covered preventive services and
any cost sharing (if applicable) can be identified clearly. This new services category will be
B14e "Other Medicare-Covered Preventive Services," and will replace B14e "Diabetes Self-
Management Training." PBP service category B14e "Other Medicare-Covered Preventive
Services" will include cost sharing fields for the glaucoma screening benefit, diabetes self-
management training, as well as up to five other optional Medicare-covered preventive services
for which a copayment may be required that can be entered by the MAO.
CMS received comments requesting examples of preventive services that may be included in the
B14a and B14e PBP service categories. Preventive services included in the B14a PBP service
category, are subject to §422.100(k), which requires coverage of preventive services by MA
plans without cost sharing, based on coverage under Original Medicare without cost sharing
because of a grade A or B recommendation by the US Preventive Services Task Force (USPSTF)
and are listed at §410.152(l). As noted in the 2011 final rule [76 FR 21475 (April 15, 2011)],
§422.100(k) is designed to require zero cost-sharing for services within the scope of
§1833(a)(1)(Y), which requires that the preventive service be graded A or B by USPSTF. Please
note that services not graded A or B by USPSTF and/or not covered without cost sharing by
Original Medicare are appropriate for the B14e service category.
We also received a comment recommending inclusion of information regarding Advance Care
Planning coverage in the Call Letter. Advance Care Planning is a Medicare covered benefit, and
as such, is required to be covered by MA plans.
178
Policy Updates
Tiered Cost Sharing of Medical Benefits
MAOs may choose to tier the cost sharing for contracted providers as an incentive to encourage
enrollees to seek care from providers the plan identifies based on efficiency and quality data. In
addition to other standards for this plan design that are provided in the Medicare Managed Care
Manual, Chapter 4, the tiered cost sharing must be applied so that all plan enrollees are charged
the same cost sharing amount for any specific provider and all providers are available and
accessible to all enrollees in the plan. CMS reminds organizations that they may not exclude any
members from being eligible to access tiered providers.
We received comments expressing concern about the criteria the plans are using to select tiered
providers, and about beneficiaries being challenged to navigate plans that tier medical benefits in
order to have access to the most appropriate physicians and hospitals. Organizations are
permitted to define their tiering approach based on their own efficiency and quality data. In
addition, organizations are required to satisfy all MA provider contracting and benefit
requirements, as well as communicate benefits in a clear and transparent manner through
marketing materials.
CMS received comments requesting further clarification on tiering requirements and the tiering
request submission process. For CY 2017, MAOs will be submitting tiering requests through an
electronic mailbox. Organizations must submit the benefit design to CMS prior to bid
submission to help make sure benefits are acceptable and communications are transparent for
beneficiaries. Organizations also are permitted to modify proposed cost sharing amounts in their
actual bid submission. Further details regarding the process will be provided in an HPMS
memorandum in mid-April.
Cost Sharing /Bundling and Facility
As discussed in the draft Call Letter, CMS wants to make sure that cost sharing requirements are
transparent to MA enrollees and Medicare beneficiaries who are considering enrolling in MA.
We look to MA plans to present enrollee cost sharing so that it is simple and easy to understand.
Specifically, MA plans should not unbundle Medicare services and charge multiple cost sharing
for services. For example, we are aware that in some cases an enrollee may receive a service in a
facility setting that includes an additional facility fee that does not apply when the service is
furnished in a physician’s office. While MA plans may have higher copays based on place of
service, the enrollee’s entire cost sharing responsibility should be apparent and included in a
single copayment or coinsurance. This approach makes it easier for enrollees to understand and
anticipate the cost sharing they will incur prior to receiving services. Our policy to provide as
much transparency as possible about MA benefits and enrollee cost sharing, is long-standing and
is consistent with MA disclosure requirements at 42 CFR section 422.111(b)(2) which require

179
that MA plans clearly and accurately disclose benefits and cost sharing. Accordingly, in
situations where there is a difference in cost sharing based on place of service, charges such as
“facility fees,” should be combined (bundled) into the cost sharing amount for that particular
place of service and clearly reflected as a total copayment in appropriate materials distributed to
beneficiaries. Our goal is not to prevent appropriate cost sharing, but to ensure that cost sharing
is transparent.
We received several comments on this issue, a number of which were supportive and a few that
asked for additional clarification and examples. Our expectation is that an MA enrollee will see
the actual and complete cost sharing for a particular service fully and clearly disclosed in the
members’ Evidence of Coverage (EOC) document, in Medicare Plan Finder, and in plan
materials. We have encountered instances where it was not readily apparent in plan disclosure
documents that the member would be charged cost sharing for a particular service furnished in a
specific place of service in addition to a separate facility fee. To avoid the enrollee confusion
caused by charging multiple cost share amount for a single service we are clarifying that we
expect MAOs to charge a single cost sharing amount to enrollees that combines all cost sharing
associated with a particular service.
Interoperability-MA Plans and Contracted Providers
Background
Interoperability is the ability of systems to exchange and use electronic health information from
other systems without special effort on the part of the user.
19
The health care industry is moving
towards interoperability because it promotes more effective exchange of health information,
seamless care transitions, improved care coordination and enrollee health outcomes and enables
providers and communities to deliver smarter, safer and more efficient care.
We believe that commercial payers as well as the Medicaid program have taken steps to promote
interoperability across provider settings, and align with Office of the National Coordinator for
Health Information Technology (ONC) standards for meaningful use and certified electronic
health records (EHRs). CMS issued a final rule on October 16,
2015 requiring eligible
professionals to utilize certified technology to promote health information exchange as part of
the Medicare and Medicaid EHR Incentive Program. This is a broader effort, however, to
support delivery system reform and quality initiatives focused on patient outcomes.
In addition, §13112 of the American Recovery and Reinvestment Act of 2009 (ARRA), requires
that our contracts require MAOs to utilize, where available, health information technology
systems and products that meet standards and implementation specifications adopted under
§3004 of the Public Health Services Act, as amended by §13101 of the ARRA.
19
Institute of Electrical and Electronic Engineers- http://www.ieee.org/200Bindex.html?WT.mc_id=mn_ieee.
180
In alignment with the referenced legislation and Medicaid, CMS is currently exploring how best
to encourage the adoption of technology that supports interoperability between MAOs and their
contracted providers, and the need for rulemaking to require such adoption. In the draft Call
Letter, CMS sought comment from the industry regarding their experience with these activities,
including barriers to successful adoption.
We received several comments regarding experience with the adoption of technology supporting
interoperability between MAOs and contracted providers. Most of the comments received were
supportive of interoperability and recognized the benefits of sharing information and having a
more complete and informed view of enrollees. Commenters outlined the barriers to adopting
the necessary technology and made recommendations. We appreciate the comments received on
this topic and will take them into consideration as we consider future policy-making, especially
with respect to providers participating in alternative payment models. In addition, CMS will
continue to gain insight from the industry and other stakeholders, into the complexities of
adopting technology that supports interoperability.
Alternative Payment Models (APMs)
Alternative Payment Models (APMs) are provider payment structures that incentivize health care
quality, emphasize value over volume, and improve care coordination activities. To help
promote the transformation of our health care delivery system away from rewarding volume over
value, the Administration has set a goal to have 30 percent of Medicare fee-for-service payments
made tied to APMs by the end of 2016 and 50 percent by the end of 2018. The Administration
announced that an estimated 30 percent of Medicare payments are tied to alternative payment
models as of January 2016.
In the Contract Year (CY) 2016 Call Letter, CMS indicated that we would reach out to MAOs to
gain a better understanding of their use of provider incentives and value based contracting for
physician services. Subsequently, CMS had conversations with a number of MAOs concerning
their use of APMs. As a result of the high level of interest in the use of APMs and the long term
Administration payment goals, CMS has added APM questions to the Part C reporting
requirements. Specifically, CMS will ask MAOs to report on the proportion of payments made
to providers based on the HHS developed four categories of value based payment: fee-for-
service with no link to quality; fee-for-service with a link to quality; alternative payment models
built on fee-for-service architecture; and population-based payment.
In order to maintain consistency with HHS goals of increasing the proportion of payment made
based on quality and value, CMS will continue to support MAOs’ efforts to improve cost
efficiency, reduce costs, and improve health outcomes through the use of APMs. In order to
better support the continued implementation, growth, and sustainability of these models in MA,
in the draft Call Letter, CMS sought comments from the industry regarding challenges and
concerns associated with the use of APMs in MA.

181
We received many comments from physician groups, beneficiary advocates, MAOs, and other
stakeholders, expressing support for CMS’s efforts in this area. Some MAOs asked that CMS
further clarify and define the HHS categories of value based payment. For further information
concerning these categories, we ask that plans refer to the LAN APM Definitional Framework
White Paper at https://hcp-lan.org/workproducts/apm-whitepaper.pdf.
Connecting Beneficiaries to Care
As a reminder, MA beneficiaries are entitled to an introductory “Welcome to Medicare”
preventive visit within their first twelve months in Medicare. Each year thereafter, MA
beneficiaries are then entitled to an Annual Wellness Visit (AWV). CMS recognizes the
importance of yearly preventive visits to drive quality improvement in the care beneficiaries
receive and will continue to look at ways in which MAOs can further engage beneficiaries and
connect them to preventive and needed care.
Counseling and Related Support Services
Recognizing that Alzheimer’s disease and related dementias pose a serious and growing threat to
Medicare beneficiaries and their families, CMS encourages MAOs to offer enrollees who are
diagnosed with Alzheimer’s or other related dementias innovative supplemental benefits that
could enable their enrollees to remain in the community. Such benefits would provide a defined
set of counseling and related supports to the enrollee or to the enrollee together with their
informal (non-paid) caregivers. In designing their supplemental benefits, MAOs can take
advantage of a variety of resources, including those provided by the Alzheimer’s Association,
and learning from models such as the New York University Caregiver Intervention (NYUCI) and
the Department of Veterans’ Affairs Resources for Enhancing Alzheimer’s Caregivers Health
(REACH) program.
Prohibition on Billing Medicare-Medicaid Enrollees for Medicare Cost-Sharing
We remind all Medicare Advantage (MA) plans of their obligation to protect dual eligible
beneficiaries from incurring liability for Medicare cost-sharing. In July 2015, CMS released a
study finding that confusion and inappropriate balance billing persist notwithstanding laws
prohibiting Medicare cost-sharing charges for QMB beneficiaries, Access to Care Issues Among
Qualified Medicare Beneficiaries (QMB) (“Access to Care”) https://www.cms.gov/Medicare-
Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-
Coordination-Office/Downloads/
Access_to_Care_Issues_Among_Qualified_Medicare_Beneficiaries.pdf. These findings
underscore the need to re-educate providers, plans, and beneficiaries about proper billing
practices for dual eligible enrollees.
Under 42 CFR §422.504(g)(1)(iii), all MAOs --without exception-- must educate providers about
balance billing protections applicable to dual eligible enrollees. Federal law bars Medicare

182
providers from collecting Medicare Part A and Medicare Part B deductibles, coinsurance, or
copayments from those enrolled in the Qualified Medicare Beneficiaries (QMB) program, a dual
eligible program which exempts individuals from Medicare cost-sharing liability. (See Section
1902(n)(3)(B) of the Social Security Act, as modified by 4714 of the Balanced Budget Act of
1997). Balance billing prohibitions may likewise apply to other dual eligible beneficiaries in MA
plans if the State Medicaid Program holds these individuals harmless for Part A and Part B cost
sharing. See 42 CFR §422.504(g)(1)(iii). For more information about dual eligible categories
and benefits, please visit: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-
Network-MLN/MLNProducts/downloads/
medicare_beneficiaries_dual_eligibles_at_a_glance.pdf.
In contracts with providers, MAOs must specify these balance billing prohibitions and instruct
providers to either accept the MA payment as payment in full or bill the State for applicable
Medicare cost-sharing for enrollees that are eligible for both Medicare and Medicaid. MA plans
can find information about an enrollee’s dual eligible status in the Monthly Membership Detail
Data File. (See Appendix F.12, # 85 Dual Status Code in the Plan Communications User Guide
Appendices at https://www.cms.gov/Research-Statistics-Data-and-Systems/CMS-Information-
Technology/mapdhelpdesk/Plan_Communications_User_Guide.html).
In addition, CMS encourages MAOs to take affirmative steps to address common points of
confusion among providers regarding balance billing. For example, we urge MAOs to explain
that all MA providers-- not only those that accept Medicaid-- must abide by the balance billing
prohibitions. Further, CMS suggests that plans clarify that balance billing restrictions apply
regardless of whether the State Medicaid Agency is liable to pay the full Medicare cost sharing
amounts. (Federal law allows State Medicaid Programs to reduce or negate Medicare cost-
sharing reimbursements for QMBs in certain circumstances. See Section 1902(n)(3)(B) of the
Social Security Act, as modified by 4714 of the Balanced Budget Act of 1997).
Finally, to monitor provider compliance with balance billing rules and target provider outreach,
CMS encourages MAOs to identify problem areas from plan grievance and CMS Complaint
Tracking Module data. These steps will complement continued MAO efforts to remediate
individual violations and clarify appropriate billing procedures.
We received several supportive comments regarding the draft Call Letter’s reminder to MA
plans of their obligations to protect dual eligible beneficiaries from balance billing by educating
providers about billing prohibitions. Numerous commenters concurred that confusion and
inappropriate billing still exist, agreed that provider contracts must specify applicable rules, and
supported our recommendations that plans address common points of confusion and use
grievance and Complaint Tracking Module data to monitor plan compliance. We thank
commenters for these comments and note that we are adopting the draft language in its entirety.
183
Additionally, we received a number of requests seeking further information for providers and
additional CMS recommendations to improve compliance. In response to commenters’ request
for clarification, we note that our interpretation of the applicable anti-discrimination provisions is
that MA providers are prohibited from discriminating against patients based on their QMB
status. (See Managed Care Manual, Ch. 4, Section 10.2.5). We will consider adding a policy
clarification to future guidance in this regard. We point out that CMS has stepped up efforts to
educate providers and beneficiaries about balance billing rules and is considering administrative
options to help providers better identify QMB patients. Finally, CMS continues to explore
further measures to address and track billing problems and to promote adherence to billing rules.
Medicare Advantage Organization Responsibilities for Clinical Trials
We want to remind MAOs of their responsibilities regarding clinical trials. These
responsibilities are also specified in section 10.7 of Chapter 4 of the Medicare Managed Care
Manual. While Original Medicare is generally responsible for payment of costs for most clinical
trials, under National Coverage Determination (NCD) 310.1, MAOs are responsible for payment
in the following instances:
Category A and B investigational device exemption trials
MAOs are responsible for payment of claims related to enrollees’ participation in both
Category A and B investigational device exemption (IDE) studies that are covered by the
Medicare Administrative Contractor (MAC) with jurisdiction over the MA plan’s service
area. The MAO is responsible for payment of routine care items and services in CMS-
approved Category A IDE studies and for routine care items and services, as well as the
Category B device under study in Category B IDE studies.
The local MAC(s) with jurisdiction over the MA plan’s service area determines coverage
of IDE studies.
NCDs for clinical trials with coverage with evidence development
In separate NCDs requiring coverage with evidence development (CED), original
Medicare covers items and services in CMS-approved CED studies. MAOs are
responsible for payment of items and services in CMS-approved CED studies unless
CMS determines, for each NCD, that the significant cost threshold is exceeded for that
item or service (see 42 CFR §422.109). Approved CED studies are posted on the CMS
Coverage with Evidence Development webpage (see
http://www.cms.gov/Medicare/Coverage/Coverage-with-Evidence-
Development/index.html). Billing instructions are issued for each NCD.
In the case of clinical trials that are paid for by Original Medicare under NCD 310.1, we require
MAOs, to provide coverage for: (1) services to diagnose conditions covered by clinical trial

184
services, (2) most services furnished as follow-up care to clinical trial services and (3) services
already covered by the MAO. Should an MA plan beneficiary choose to participate in a clinical
trial, he or she may remain in his or her MA plan while paying Original Medicare costs for a
qualifying clinical trial.
20
We received one comment on this section during the public comment period. The commenter
disagreed with CMS’s current policy of paying on a fee-for-service basis for qualified clinical
trials items and services provided to MA beneficiaries that are covered under the relevant NCDs
on clinical trials. CMS is not revising its current clinical trial policy.
Dual-Eligible Special Needs Plans
We received broad support from commenters, including D-SNP sponsors, states, and beneficiary
advocates, to take administrative steps that enhance CMS-state cooperation in managing the D-
SNP program and improving the experience for dually-eligible beneficiaries enrolled in these
plans. We are grateful for this support. Commenters provided helpful recommendations on how
we could best operationalize the steps proposed in the draft Call Letter and suggested other
actions we could take in this area. We are taking all those comments into consideration as we
move forward.
In addition to the comments on the specific areas below, we received comments regarding four
additional areas in which CMS should use its administrative flexibility: (1) the use of integrated
model marketing materials; (2) translation requirements; (3) joint CMS and State oversight of D-
SNPs; and (4) use of Medicare-Medicaid Plan (MMP) network adequacy standards and
processes. Several commenters recommended that CMS expand the use of modified MMP
member materials to other D-SNPs beyond those participating in the Minnesota Demonstration
to Align Administrative Functions for Improvements in Beneficiary Experience. CMS has
received positive feedback from states and plans, including those in Minnesota, regarding
integrated model materials, such as a Summary of Benefits, Annual Notice of Change, Evidence
of Coverage/Member Handbook, List of Covered Drugs (formulary), and Provider and Pharmacy
Directory, developed for both the Financial Alignment Initiative demonstrations as well as the
Minnesota demonstration. The materials integrate Part C, Part D, and Medicaid benefits
information and have been consumer tested. CMS will continue to explore the feasibility of
allowing integrated D-SNPs to use these model material templates in lieu of the Medicare
Advantage and Part D models.
Several commenters requested that CMS expand its translation requirements to encompass more
materials and more languages than are currently required under the MA and Part D regulations
and the Medicare Marketing Guidance. While changing the translation standard for Medicare
health plans would require a regulation change, we will continue to explore other options for
20
Clinical trials are covered under the Clinical Trials National Coverage Determination (NCD) (NCD manual, Pub. 100-3, Part 4,
Section 310).
185
addressing the concerns about receipt of the Multilanguage Insert, as well as translation of
additional materials than those currently required in the Medicare Marketing Guidelines pursuant
to 42 CFR§ 422.2264(e) and § 423.2264(e). We also note that states can impose additional
requirements regarding translation of member materials via their MIPPA contracting with D-
SNPs. In addition, as outlined in 42 CFR § 422.111(h)(1)(iii) and § 423.128(d)(1)(iii),
MAOs/Part D sponsors must provide interpreter service to all non-English speaking and limited
English proficient beneficiaries regardless of the percentage of non-English speaking
beneficiaries in the service area.
We received several comments requesting the collaborative contract oversight process and the
network standards used in the Minnesota demonstration be extended to other integrated D-SNPs.
CMS intends to continue to test the network standards that target the dual eligible population in
the Minnesota demonstration before making a determination on using the standards for other
integrated D-SNPs.
CMS will continue to evaluate how best to provide effective oversight in other states with
integrated D-SNPs. We note that CMS has already established joint monitoring calls in one
other state.
D-SNP Non-Renewals
We received broad support to notify states of pending nonrenewals, service area reductions, and
terminations of integrated D-SNPs that deliver Medicaid benefits prior to the public release of
this information in the fall, when D-SNPs and other MA plans must send their nonrenewal
notices. Commenters stated that early notification would allow states to make preparations to
minimize any disruption in the delivery of Medicaid benefits provided by nonrenewing
integrated D-SNPs and to work with their contracted D-SNPs to ensure D-SNP messaging,
including the required nonrenewal notice, accurately conveys the impact nonrenewal will have
on the delivery of Medicaid benefits and the options Medicare-Medicaid enrollees have for their
Medicaid coverage. We will work with states and plan sponsors as we develop procedures,
including appropriate assurances of confidentiality when notifying states of pending nonrenewals
of their contracted D-SNPs. In addition, we will work with stakeholders to improve the model
nonrenewal notice for integrated D-SNPs that we piloted last year in Arizona.
D-SNP Model of Care
Beneficiary advocates, states, and D-SNP sponsors were generally supportive of a process for
interested states to add specificity to existing elements that describe state requirements related to
the management of Medicaid Long-Term Services and Supports (LTSS) to the CMS review
criteria for model of care (MOC) employed by D-SNPs that deliver Medicaid LTSS. Similarly,
we received support for allowing states to review MOCs against their requirements concurrent
with NCQA’s review of MOCs in HPMS. Taken together, these proposals would help the MOC
review ensure that the D-SNP MOCs fully address state goals for the delivery of LTSS by their
186
contracted D-SNPs. We intend to work with stakeholders to ensure that this process does not
create a more burdensome MOC review process for D-SNP sponsors.
While we intend to create a process that would allow states to share the results of their review
with CMS, we reiterate that the joint review process would not change the current CMS
requirements for review and approval of D-SNP MOCs by NCQA. We also note that states have
the ability now through their D-SNP MIPPA contracts to require that the MOC address delivery
of Medicaid benefits, in particular LTSS, and to require their contracted D-SNPs to revise their
MOCs to meet state requirements. This process does not alter that ability but integrates the state
and CMS process for review of the MOC for integrated D-SNPs.
Finally, we recognize that the review of MOCs at the contract level may require some changes to
the way in which the MOC describes different care processes for different populations under the
contract, particular when some D-SNPs under the same contract may deliver Medicaid LTSS
while other D-SNPs do not. We will work with D-SNP sponsors so that the contract-level MOC
can reflect the differing care needs of different populations under the contract.
Section III – Part D
Formulary Submissions
CY 2017 Formulary Submission Window
The CY 2017 HPMS formulary submission window will open this year on May 16, 2016 and
close at 11:59 pm PDT on June 6, 2016. CMS must be in receipt of a successfully submitted and
validated formulary submission by the deadline of June 6, 2016 in order for the formulary to be
considered for review. The Part D formulary is part of the plan’s complete bid and therefore a
failure to submit and link a formulary to each plan that uses a formulary by the June 6th deadline
will result in denial of that bid submission.
CY 2017 Formulary Reference File
CMS released the first CY 2017 Formulary Reference File (FRF) in March 2016. The March
FRF release will be used in the production of the Out-of-Pocket Cost (OOPC) model tool,
scheduled to be released in April 2016, in order to assist plan sponsors in satisfying meaningful
difference and MA TBC requirements prior to bid submission. Sponsors should note that the
OOPC model released in April will not be modified to incorporate any subsequent FRF updates,
as described below.
In May 2016, CMS is planning to provide a subsequent release of the 2017 FRF prior to the June
6th formulary submission deadline. We will aim to make the May FRF available earlier this
year, although it will be released in mid to late-May in order to allow for sufficient time to
evaluate and add new Part D drugs that become available in our datasets. Since the OOPC
187
model incorporates Medicare Current Beneficiary Survey (MCBS) data from 2010 and 2011,
new Part D drugs cannot be included in the OOPC model since they would not have appeared in
the survey. Further, given the limited timeframe between the May release of the 2017 FRF and
the June 6th deadline, CMS is unable to accommodate an updated version of the 2017 OOPC
model to incorporate the new generics that may be added to the May FRF. Therefore, CMS
cautions plan sponsors that any newly added drugs on the May release of the 2017 FRF will not
be included in the 2017 OOPC model.
CMS will continue to offer a summer formulary update; however, formulary changes during this
particular update submission will be limited to: 1) the addition of drugs that are new to the
summer release of the FRF (historically posted in July); and 2) the submission of negative
changes on brand drugs, only if the equivalent generic is added to the summer FRF and
corresponding formulary file. Thus, plan sponsors need to carefully consider any newly added
drugs to the May release of the 2017 FRF, since additional limitations will be imposed on the
summer formulary update window. While moving the summer formulary update window later in
the year would result in more up-to-date formulary information, this benefit must be weighed
against Part D sponsors’ ability to print marketing materials by necessary deadlines. We will,
however, investigate whether an additional HPMS formulary enhancement-only window is
possible for CY 2017.
Part D sponsors are reminded that they may enhance their formularies by adding Part D drugs
(with or without utilization management restrictions), reducing beneficiary cost-sharing, or
removing utilization management edits between the summer update window and the first HPMS
submission of the upcoming plan year. Consistent with section 60.5 of the Medicare Marketing
Guidelines, these enhancements must be included in the Part D sponsor’s marketing materials
and must be submitted during the next available HPMS formulary submission
window. Sponsors are encouraged to notify beneficiaries of formulary additions in a timely
manner since in some cases, such as new generics, an earlier conversion could lead to better
value for the beneficiary and potentially reduce program costs.
In an effort to better align plan sponsors’ submission of quantity limits (QLs) with CMS’ review,
a new column will be added to the HPMS-posted FRF that indicates the unit for which sponsors
must submit their QLs. While the vast majority of submitted QLs, such as those for solid oral
dosage forms are straightforward, this additional information will be useful for products such as
kits that contain prefilled syringes. The HPMS formulary submission will not be validated
against this field. Rather, it will serve as a point of reference for CMS and Part D sponsors
during the review of submitted QLs. Finally, we are evaluating the feasibility of including an
informational column on the FRF that would periodically track price changes for FRF drugs.

188
Appropriate Utilization of Prior Authorization Requirements to Determine Part D
Drug Status
Consistent with 42 CFR §423.153(b), CMS reminded sponsors in the 2015 Call Letter that they
must establish utilization management controls, such as prior authorization (PA), in order to
reduce costs and to prevent inappropriate utilization of prescribed medications under Part D.
Currently, we permit Part D sponsors to implement point of sale (POS) PA edits to determine
whether a drug is: 1) covered under Medicare Parts A or B; 2) being used for a Part D medically-
accepted indication (MAI) (as defined in section 1860D-2(e)(4) of the Social Security Act); or 3)
a drug, drug class, or has a medical use that is excluded from coverage or otherwise restricted
under Part D as defined in section 1860D-2(e)(2) of the Act (e.g., when used for cosmetic
purposes or hair growth). While CMS allows sponsors to implement these PAs during transition
(either for new enrollees into a plan or for current enrollees affected by formulary changes) to
prevent Part D coverage for excluded drugs or for non-medically-accepted indications of Part D
drugs, sponsors continue to be confused about which POS PA edits are permitted during
transition. Section 30.4.8 of Chapter 6 of the Prescription Drug Benefit Manual (available at
https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/
Downloads/Part-D-Benefits-Manual-Chapter-6.pdf) discusses edits for transition fills. The
requirements for Part D sponsors to limit coverage to Part D drugs and Part D medically-
accepted indications, assist in preventing over-utilization and under-utilization of prescribed
medications, and utilize quality assurance measures and systems to reduce medication errors and
adverse drug interactions and improve medication use apply regardless of the transitional status
of an enrollee’s medication(s). In other words, POS PA edits for such purposes are appropriate
even during transition.
The 2015 Call Letter encouraged sponsors to utilize PA for drugs that have a high likelihood of
use for a non-medically-accepted indication. Section 10.6 of Chapter 6 of the Prescription Drug
Benefit Manual discusses medically-accepted indication (available at:
https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/
Downloads/Part-D-Benefits-Manual-Chapter-6.pdf)
The 2015 Call Letter specified Transmucosal Immediate Release Fentanyl (TIRF) products and
Cialis as examples of drugs that have a high likelihood of use for non-medically-accepted
indications. Our guidance is focused on those drugs that pose the greatest risk for non-medically
accepted indications, and, therefore, CMS does not expect to see POS PA edits during transition
to determine the indication on most Part D drugs.
Coverage duration is a required component of criteria that are submitted to CMS as part of the
formulary review process for PA approval. Sponsors often approve criteria for the duration of
the plan year or for one calendar year from the initial approval date. Once a PA is approved,
sponsors are not prohibited from utilizing “grandfathering” policies that allow beneficiaries to
receive a drug from year to year without a requirement to satisfy the PA criteria in the future. In

189
general, policies that facilitate appropriate access to medications for beneficiaries with chronic
conditions are looked upon favorably by CMS. However, if such policies are implemented for
products that have significant safety concerns and the high potential for non-MAI use (e.g., TIRF
drugs), we expect sponsors to periodically confirm that beneficiaries continue to use these drugs
for medically-accepted indications. This confirmation can be accomplished by establishing
limits to the “grandfathering” processes for these drugs or through robust retrospective drug
utilization review processes. This expectation would also apply to cases where members are
moving across plans or when a new PBM is being utilized, for example.
Medication Therapy Management (MTM)
Annual MTM Eligibility Cost Threshold
Targeted beneficiaries for a Part D plan’s MTM program, in general, are enrollees who meet all
of the following criteria: have multiple chronic diseases, are taking multiple Part D drugs, and
are likely to incur annual Part D drug costs that meet or exceed a certain threshold. Per
§423.153(d), for 2012 and subsequent years, the annual cost threshold for targeting beneficiaries
is specified as costs for covered Part D drugs in an amount greater than or equal to $3,000
increased by the annual percentage specified in §423.104(d)(5)(iv). The 2016 MTM program
annual cost threshold is $3,507. The 2017 MTM program annual cost threshold is updated for
2017 using the annual percentage increase of 11.75%, as specified in the Calendar Year (CY) 2017
Medicare Advantage Capitation Rates and Medicare Advantage and Part D Payment Policies.
Therefore, the 2017 MTM program annual cost threshold is $3,919.
Annual MTM Submission and Approval Process
A memo containing MTM program guidance and submission instructions is released each year
by CMS and is available on the CMS.gov MTM page at: https://www.cms.gov/Medicare/
Prescription-Drug-Coverage/PrescriptionDrugCovContra/MTM.html. The guidance memo for
CY 2017 will be released approximately one month before the 2017 MTM program submission
deadline. The CY 2017 guidance memo will include the MTM program submission template.
Questions regarding the MTM submission process or policy may be sent via email to
Annually, Part D plan sponsors must submit an MTM program description to CMS through the
Health Plan Management System (HPMS) for review and approval. CMS evaluates each
program description to verify that it meets the current minimum requirements for the program
year.
Due to enhancements to the HPMS MTM submission module and expanded guidance and
submission instructions over the years, MTM program submissions have increasingly high rates
of initial approval. Beginning with the CY 2017 submissions, we will implement a modified

190
annual MTM program review process and add attestations to the HPMS submission module as
described below.
All Part D sponsors will continue to submit an MTM program description through
HPMS each year. Sponsors will continue to submit change requests throughout the
year.
Attestations of the Part D sponsor’s compliance with Part D MTM program
requirements will be added to the MTM submission module in HPMS. The
attestation will be included in the CY 2017 guidance memo.
Sponsors must attest to meeting the MTM program requirements during the annual
submission. Sponsors must re-attest when they submit change requests. The MTM
Attestation must be completed via HPMS by the Chief Executive Officer (CEO),
Chief Operating Officer (COO), or the Chief Financial Officer (CFO).
A subset of MTM program submissions will be comprehensively reviewed including:
o Any new contracts;
o Any contracts whose MTM submission failed initial review the prior year;
o Any contracts that failed reporting requirements data validation or audit for
MTM (when implemented);
o Any contracts that scored less than 3 stars on the MTM comprehensive
medication review completion rate measure; and
o Any contracts selected based on a random sample of other program submissions.
The Annual Calendar in this Call Letter highlights key dates for the submission of MTM
programs and attestations, as applicable. Of note, the attestation deadline is two weeks after the
deadline for submission of CY 2017 MTM programs in HPMS. We will continue to monitor
beneficiary complaints, validation results of plan-reported MTM data, and CMS program audits
of MTM programs.
Submission Requirements for Enhanced MTM Model Participants
The CMS Center for Medicare and Medicaid Innovation announced the Part D Enhanced MTM
Model, an opportunity for stand-alone basic Prescription Drug Plans (PDPs) in selected regions
to offer innovative MTM programs, aimed at improving the quality of care while also reducing
costs. More information about the model test is available at https://innovation.cms.gov/
initiatives/enhancedmtm/.
The Enhanced MTM Model test will begin January 1, 2017 with a five-year performance
period. CMS will test the model in 5 Part D regions: Region 7 (Virginia), Region 11 (Florida),
191
Region 21 (Louisiana), Region 25 (Iowa, Minnesota, Montana, Nebraska, North Dakota, South
Dakota, Wyoming), and Region 28 (Arizona). Eligible defined standard, actuarially equivalent,
or basic alternative stand-alone PDPs in these regions, upon approval from CMS, can vary the
intensity and types of MTM items and services based on beneficiary risk level and seek out a
range of strategies to individualize beneficiary and prescriber outreach and engagement.
The current MTM requirements are waived for the PBPs approved to participate in the Enhanced
MTM Model and data on participating PBPs must not be reported per the Part D Reporting
Requirements under the current MTM program. This MTM data will instead be reported in
accordance with model terms and conditions.
Plan sponsors with contracts that include PBPs that are not eligible to participate in the model
must ensure that those non-participating plans comply with all standard MTM program
requirements, including the submission of MTM program details in HPMS. More information
will be provided in the CY 2017 guidance memo.
Part D Reporting Requirements for MTM
For monitoring purposes, Part D sponsors are responsible for reporting several data elements to
CMS related to their MTM program per the Part D Reporting Requirements. Element X,
“Topics discussed with the beneficiary during the comprehensive medication review (CMR),
including the medication or care issue to be resolved or behavior to be encouraged,” is suspended
for the 2016 Part D Reporting Requirements until a more standardized set of data can be
collected.
The industry, including the Pharmacy Quality Alliance (PQA) and the Academy of Managed
Care Pharmacy (AMCP), is working on a framework to define drug therapy problems (DTPs).
Once finalized by industry, sponsors should begin to develop the capacity to collect and report
drug therapy problems using a standard framework and common terminology. Also, after
industry development, we will consider proposing new MTM data elements for the Part D
Reporting Requirements through the Paperwork Reduction Act (PRA) process as early as the
2018 Part D Reporting Requirements to capture drug therapy problems at the beneficiary-level
using standard categories and definitions. This process allows for public comment.
Improving Clinical Decision-Making for Certain Part D Coverage Determinations
In the draft Call Letter, CMS solicited stakeholder feedback on potentially proposing regulatory
changes that would permit Part D plans to extend the adjudication timeframe for certain coverage
determination requests for drugs subject to prior authorization (PA) or step therapy (ST) where
the plan has been unable to obtain needed clinical information from the prescriber and the
adjudication timeframe has been impacted by a weekend or holiday. We received numerous
comments from a range of stakeholders in response to our request, and thank all commenters for
their helpful feedback. Almost all commenters were strongly supportive of our goal to ensure
192
that coverage determinations are made with the benefit of all information and clinical
documentation necessary for making a correct and clinically sound decision as quickly as
possible and, whenever possible, at the initial coverage determination level.
About half the comments we received were from Part D plan sponsors and PBMs. Most were in
favor of longer timeframes, but many expressed concerns that the limitations we suggested
would be confusing, as well as costly and difficult for plans to implement. Several plans and
PBMs noted that the problem of prescribers not responding to requests for additional information
is not limited to weekends and holidays, and a few stated that providing a short extension will
not likely resolve the problem of non-responsive prescribers. Some commenters expressed
concern that the Part D adjudication timeframes, even with a limited extension, would be too
short to allow for written notice of the extension without causing significant confusion, since the
written notice would be likely to arrive in the mail after the plan has rendered a decision and
provided verbal notification to the enrollee. Commenters also noted that implementation of an
extension for some types of coverage determinations, along with tolling of exception requests for
prescriber supporting statements, would create additional implementation difficulties.
For the reasons described above, most plans and PBMs that supported implementation of
extensions in Part D sought more expansive opportunities to extend the timeframes, including
allowing both tolling and extensions, allowing extensions for all coverage determinations,
eliminating the written notice requirement to the beneficiary, extending the adjudication
timeframes for standard and/or expedited cases by adding 24 or 48 hours, or advocated changes
that would allow tolling for all coverage determinations where the timeframe does not begin until
all information is received. A few plans urged CMS to immediately proceed with proposed
rulemaking that would provide longer timeframes.
Some plans and PBMs expressed concerns that CMS must ensure the use of extensions does not
adversely affect beneficiary access, and a few recommended that extensions not be allowed for
expedited requests. A few commenters believed that prescribers are more likely to respond to a
denial notice than a request for information, suggesting that issuing the denial rather than
delaying the decision may actually reduce any delay in accessing needed medications. One PBM
recommended that CMS approach this issue by urging network MA-PD and Medicare-enrolled
prescribers to be more accountable to beneficiaries when seeking coverage of a needed drug.
We received several comments from beneficiary and patient advocacy organizations, which were
also in favor of informed decision-making, but expressed significant concerns about potential
overuse of extensions and adverse impact on beneficiary health. These commenters agreed with
CMS statements in the draft Call Letter that any extensions would have to be carefully limited to
protect beneficiary access to drugs. Some commenters did not support extensions for expedited
requests. Beneficiary advocates strongly supported testing a potential policy change through a
pilot or demonstration that is open to stakeholder feedback in its design and includes benchmark
testing.
193
Comments received from pharmacies and manufacturers were mixed, with some support for
allowing sufficient time to obtain missing information and reduce rejected claim and appeals
volumes, but they also urged CMS to establish clear rules and safeguards to avoid unnecessary
delays and adverse impact on beneficiary health status. LTC pharmacies opposed extensions,
noting existing payment issues due to their requirement to dispense; further delays would cause
additional payment issues. Pharmaceutical manufacturers opposed extensions for expedited
requests because of the risk of beneficiary harm.
We received comments from a few prescriber organizations. Prescribers are opposed to
utilization management generally because they believe it does not improve quality of care and
requires too much time and paperwork. Commenters expressed concern that delays in approval
can delay or interrupt treatment and result in beneficiary harm. One commenter argued that
plans would use extensions when they failed to conduct appropriate outreach to the prescriber.
After review of all comments submitted, CMS does not intend to move forward with any
proposed regulatory changes for extensions in Part D at this time. As we stated in the draft Call
Letter, we recognize the challenge posed by the short adjudication timeframes for plans to
successfully obtain needed information from prescribers and provide a fully informed decision
within the timeframe. However, we agree with the commenters who noted that written notice of
the extension—an important beneficiary protection—would not be feasible, and that the
limitations we suggested could be confusing for plans, beneficiaries and prescribers, and difficult
for plans to implement and oversee effectively. We also agree with the numerous commenters
who expressed concerns about making broader changes to adjudication timeframes, including a
more expansive extension opportunity, given the more immediate need for access to drug therapy
and that fact that coverage must be approved before the enrollee can access the drug.
Acknowledging the challenges inherent in existing timeframes, we also recognize the limitations
we have in extending those timeframes while still complying with the statutory requirement for
timely determinations that emphasize the health needs of the beneficiary. This is particularly
true for expedited requests, where the prescriber or the plan has determined that taking additional
time to render a decision could seriously jeopardize the life or health of the beneficiary. While
retaining existing requirements, which do not allow extensions, may increase the likelihood that
plans will have to deny requests to meet the timeframes, we believe that there is great value in
the enrollee receiving the standardized denial notice that includes a written denial rationale and
an explanation of the appeals process.
While we do not intend to move forward with any rulemaking to allow extensions in Part D,
CMS will continue to explore how we might assist plans and PBMs in providing fully informed
coverage determinations, limiting unnecessary denials, and avoiding delays that could potentially
cause beneficiary harm. After consideration of the comments received on the draft Call Letter,
we intend to direct our efforts on reducing the volume of coverage determination requests that
are initially incomplete, including exploring how increased use of electronic health records and

194
other technology could make the information needed from prescribers more accessible outside of
business hours; encouraging the increased use of e-prescribing and e-prior authorization to
increase dissemination of plan formularies to prescribers at the point of care; and leveraging
MA-PD plan contracting arrangements with network providers who are prescribing Part D drugs.
CMS is currently developing additional subregulatory guidance to help ensure that Part D plan
sponsors are consistently conducting appropriate outreach to prescribers to obtain missing
information and make informed decisions within the existing Part D timeframes.
Some plans and PBMs who commented on this proposal included related plan data, e.g., rates of
adverse coverage determinations based on missing information and rates of appeals of those
denials. We want to particularly thank those commenters for providing this information as we
continue to contemplate how we might improve clinical decision-making as early as possible in
the coverage and appeals process.
Access to Preferred Cost-Sharing Pharmacies
In the CY 2016 Call Letter, CMS announced several steps we would take to address low access
to preferred cost-sharing pharmacies (PCSPs). First, we announced that we would post
information about 2016 PCSP access levels on the CMS website. Second, we announced that we
would require plans who were outliers with respect to access to PCSPs to disclose that their
plan’s PCSP network offered lower access than other plans. Outliers were set at the bottom 10
th
percentile compared to all Part D plans in a given geographic type, using 2014 data. CMS
required marketing materials to include specific disclaimer language for plans offering access
within 2 miles of less than 40% of beneficiaries’ residences in urban areas, within 5 miles of less
than 87% of beneficiaries’ residences in suburban areas, and within 15 miles of less than 70% of
beneficiaries’ residences in rural areas. Finally, we announced that we would work with plans
that were extreme outliers to address concerns about beneficiary access and marketing
representations relating to preferred cost-sharing. We worked with several such plans to either
improve access or develop targeted marketing strategies to ensure that beneficiaries selecting
these plans were aware of their status as extreme outliers.
CMS is pleased to note that plans increased PCSP access dramatically for 2016. As shown in the
table below, the bottom 10
th
percentile of plans in 2016 offer access within two miles to 71% of
urban beneficiaries, compared to 40% in 2014.
Table 17. PCSP Access Rates for the Bottom 10
th
Percentile of Plans, 2014 through 2016
2014
2015
2016
Convenient Access Standard
for All Retail Pharmacies
Urban Access Rate
40%
62%
71%
90%
Suburban Access Rate
87%
92%
95%
90%
Rural Access Rate
77%
77%
82%
70%

195
Because we believe the current policy is increasing access to PCSPs, we do not plan to make
significant changes for 2017. Specifically, we will not change the outlier thresholds for 2017 to
reflect the higher access levels achieved for 2016.
Therefore, CMS will continue its PCSP policy as announced in the 2016 Call Letter and
implemented for the 2016 plan year. Plans that provide PCSP pharmacy access within 2 miles of
less than 40% of beneficiaries’ residences in urban areas, within 5 miles of less than 87% of
beneficiaries’ residences in suburban areas, and within 15 miles of less than 70% of
beneficiaries’ residences in rural areas will be identified as outliers in 2017. Outlier plans will be
required to disclose in marketing materials, including websites, that their plans’ PCSP networks
offer lower access. Contract Year 2016 disclaimer language was announced in the June 24, 2015
HPMS memo “Marketing Disclaimer Language for Plans with Limited Access to Preferred Cost-
Sharing Pharmacies,” and in the final “Medicare Marketing Guidelines” released on July 2,
2015. CMS continues to expect that plans will analyze their own 2016 and 2017 networks to
determine whether they are below outlier thresholds. CMS will analyze preferred cost-sharing
pharmacy access on a quarterly basis and will remind plans of their outlier status periodically.
CMS will also continue to work with extreme outliers to address concerns about beneficiary
access and marketing representations related to preferred cost-sharing. CMS will notify these
plans in or around April 2016 that we plan to address 2017 PCSP access issues with them during
bid negotiations. In 2016, most plans identified as extreme outliers opted to improve access
rather than develop marketing plans to better inform beneficiaries of low PCSP access. We
anticipate plans will take similar steps during 2017 negotiations.
We will continue to publish information about PCSP access levels annually on the CMS website
at: https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/
index.html. We will also explore the feasibility of incorporating this information into the
Medicare Plan Finder in the future.
Sponsors that fail to include required marketing disclosure language and/or do not meet the terms
of bid negotiation agreements will be subject to compliance and/or enforcement actions.
Part D Benefit Parameters for Non-Defined Standard Plans
Each year, in order to implement certain regulations, we set forth certain benefit parameters,
which are based on updated data analysis, and therefore, are subject to change from year to year.
Specifically, pursuant to §423.272(b)(3)(i), CMS will only approve a bid submitted by a Part D
sponsor if its plan benefit package (other than defined standard) or plan cost structure is
substantially different from those of other plan offerings by the sponsor in the service area with
respect to key characteristics such as premiums, cost-sharing, formulary structure, or benefits
offered; and, pursuant to 42 CFR §423.104(d)(2)(iii), tiered cost-sharing for non-defined
standard benefit designs may not exceed levels annually determined by CMS to be
discriminatory. The benefit parameters for CY 2017 are set forth in Table 19 below.

196
Adjustments to the Minimum Meaningful Difference and specialty tier thresholds are described
below. The other cost-sharing thresholds are established consistent with previous years
methodology based on the 95th percentile of the CY 2016 Bid Data. For CY 2017, we will be
maintaining the copayment cost-sharing thresholds without the inflation adjustment.
Tier Labeling and Composition
We again remind sponsors that we expect Drug Tier Labels to be representative of the drugs that
make up that tier. However, we have received a number of plan sponsors’ comments via the
2016 Call Letter and in response to the Request for Comments on Non-Defined Standard Plan
Tier Models for CY 2017, solicited through a HPMS memo in June 2015, recommending that
CMS provide a non-preferred drug tier option that will allow for a drug mix regardless of
generic/brand status. Based on the comments received and as part of our continued efforts to
provide tier label options that provide flexibility and transparency in benefit design, CMS
included additional tier models for CY 2017 with a non-preferred drug tier option. The details of
CY 2017 tier model options are included in the CY 2017 Plan Benefit Package Software and
Formulary Submission PRA information collection request, now pending approval at the Office
of Management and Budget, Office of Information and Regulatory Affairs. This information
collection request is available on the CMS website at: https://www.cms.gov/Regulations-and-
Guidance/Legislation/PaperworkReductionActof1995/PRA-Listing-Items/CMS-R-262.html?
DLPage=4&DLEntries=10&DLSort=1&DLSortDir=descending.
With the addition of a non-preferred drug tier, sponsors will have the option of selecting a non-
preferred drug tier or non-preferred brand tier but not both. If sponsors continue to use a non-
preferred brand tier, CMS will evaluate the brand/generic composition of that tier as part of the
bid review process. Non-preferred brand tier outliers will be communicated for any plans that do
not have a majority of brand drug products in that tier.
Table 18. 2015 Prescription Drug Event Data
2015 PDE Data
Average of % Beneficiary Cost-Share
Generic Drugs
Brand Drugs
All Drugs
Non-Preferred Brand Total
32.56%
20.77%
22.81%
Plan w/ Copay
35.75%
19.90%
22.48%
Plan w/ Coinsurance
26.02%
22.72%
23.54%
197
CMS review of preliminary 2015 prescription drug event data (PDE) (Table 18.) showed that
beneficiaries pay a lower cost-share for generics in plans that have a coinsurance cost-sharing
structure (26.02%) for their non-preferred brand tier than in plans that use a copay cost-sharing
structure (35.75%). Overall, on average for all drugs on the non-preferred brand tier, there was
no substantial difference in beneficiary cost-sharing between plans that use a copay cost-sharing
structure and those that use coinsurance. However, based on industry comments received, it is
our understanding that the new non-preferred drug tier likely will contain a greater proportion of
generic drug products than the current non-preferred brand tier composition. While we
appreciate that generic drug price increases are changing the paradigm, we also acknowledge that
sponsors may include lower cost generics on the non-preferred drug tier in an effort to balance
the brand/generic drug composition of the tier and maintain actuarial equivalence. As cost trends
in the Part D program are increasingly driven by high cost drugs it is important that we consider
policy impacts on beneficiaries with lower overall drug costs. In the draft Call Letter, we
proposed that Part D sponsors consider the use of a coinsurance structure for the non-preferred
drug tier instead of a copay. While the analysis outlined above in Table 18 demonstrated
reduced cost-sharing for generics on non-preferred brand tiers with coinsurance cost structures,
we did receive comments that suggest beneficiaries tend to prefer copay structures and that Part
D sponsors would like to continue to have options in their benefit design. We recognize that
there are advantages and disadvantages of copay/coinsurance cost-sharing structures, including
the consistency that a copay structure offers to beneficiaries. As such, CMS will allow Part D
sponsors the flexibility to determine what cost-sharing structure is most appropriate for their
benefit design. We will expect, however, that sponsors evaluate, and be prepared to demonstrate
if necessary, that the cost-sharing structure chosen provides a value for beneficiaries. During the
first year of implementation and until further notice, CMS will conduct an outlier test for those
Part D sponsors who choose a copay for the non-preferred drug tier, to determine if beneficiaries
will receive a benefit for drugs on this tier at the proposed copay. Moving forward, we will
continue to evaluate the type and level of cost-sharing that is most appropriate for this tier and
that balances the Part D sponsor’s ability to mix brand and generic drugs within a tier while
maintaining transparency and a meaningful benefit offering for the beneficiaries who enroll in
plans with non-preferred drug tiers.
A few commenters requested guidance on how to handle tiering exceptions for the non-preferred
drug tier option. Sponsors should refer to existing tiering exception guidance, which can be
found at 42 CFR §423.578(a) and in Chapter 18, section 30.2.1 of the Prescription Drug Benefit
Manual. This guidance is applicable to this new tiering option. Tiering exceptions allow an
enrollee to request coverage of a drug in a higher cost-sharing tier at the more favorable terms
applicable to drugs in a lower cost-sharing tier provided certain conditions are met. The
applicability of a tiering exception is generally not determined by the name of the tier (e.g.,
Preferred Generic, Non-Preferred Brand), but rather by the drugs included on that tier, the
availability of therapeutically equivalent drugs on the plan sponsor’s formulary, and a
determination by the plan, based on the prescriber’s supporting statement, that the drug in the
198
lower cost-sharing tier for the treatment of the enrollee’s condition 1) would not be as effective
as the requested drug in the higher cost-sharing tier and/or 2) would have adverse effects.
For purposes of determining whether coverage gap cost-sharing thresholds specified in Table 19
have been met, we will continue to rely on the FDA marketing status to identify formulary drugs
as applicable or non-applicable. The maximum coinsurance of 60% applies to tiers that contain
only applicable drugs. If non-applicable (i.e., generic) drugs or a combination of both generic
and applicable drugs are on a tier, then the maximum coinsurance of 31% applies. We remind
sponsors that when cost-sharing reductions beyond the standard benefit are offered through a
supplemental Part D benefit, the plan liability is applied to applicable drugs for applicable
beneficiaries before the manufacturer discount.
Benefit Review
We will continue to scrutinize the expected cost-sharing amounts incurred by beneficiaries under
coinsurance tiers in order to more consistently compare copay and coinsurance cost-sharing
impacts. If a sponsor submits coinsurance values (instead of copayment values) for its non-
specialty tiers that are greater than the standard benefit of 25%, we will compare the average
expected cost-sharing amounts submitted by sponsors in the PBP to the established copay
thresholds to determine whether the coinsurance values are discriminatory. Please note that we
will conduct the same cost-sharing analysis for the Select Care/Diabetic Drug Tiers, even though
the maximum allowable coinsurance value is less than 25%. We will also continue to disallow
incentives such as $0 or very low cost-sharing for 30 day supplies at mail service, unless offering
the same cost-sharing at the retail network.
Despite ACIP recommendations and Healthy People 2020 targets, adult immunization rates still
remain low. We encourage Part D sponsors to consider offering $0 or low cost-sharing for
vaccines to promote this important benefit. While the inclusion of a dedicated vaccine tier or a
Select Care/Select Diabetes tier that contains vaccine products as part of a 5 or 6 tier formulary
structure is not a requirement, sponsors who choose to offer one of these formulary tiers must set
the cost-sharing at $0 for that tier. This policy is unchanged from CY 2016.
Over the last three years, we have seen a continuing decrease in the 95
th
percentile meaningful
difference between basic and enhanced alternative (EA) plans which indicates there is a
decreasing differential between basic and EA plan drug benefits. In order to continue to drive
the participation of plans that provide distinct product offerings, CMS will use a meaningful
difference threshold based on the 50
th
percentile for CY 2017 instead of the 95
th
percentile. As a
result of the closing of the coverage gap, the change for CY 2017 to the 50
th
percentile is
necessary to maintain an OOPC differential within the range of the original meaningful
difference threshold. Specifically, the meaningful difference threshold will be based on the 50
th
percentile of the October CY 2016 Bid Data run through the CY 2016 OOPC MPF model which
incorporates CY 2016 Formulary Data, 2010/11 MCBS Data, and FDA data for brand/generic
199
determinations related to coverage gap cost-sharing estimates. In contrast to the continuing
decrease in the 95
th
percentile meaningful difference between basic and EA plans, we have seen
a continuing increase in year over year meaningful difference between EA to EA plans. The
increase in meaningful difference between EA to EA plans makes it more challenging for plan
sponsors to offer second EA plans. For CY 2017, we will also use the 50
th
percentile, instead of
the 95
th
percentile, to establish the meaningful difference threshold between EA to EA plans to
lessen the impact of EA to EA differences year over year and help maintain stability in the
program.
Therefore, in 2017 the minimum monthly cost-sharing OOPC difference between basic and
enhanced PDP offerings will be $23 and the minimum monthly cost-sharing OOPC difference
between enhanced PDP offerings will be $34. These values remain in close range of those
established originally for this policy in 2012.As in the past, these meaningful difference
requirements apply to all stand-alone PDPs, including those belonging to sponsors under a
consolidation plan. We also continue to expect that the additional EA PDPs within a service area
will have a higher value than the first EA plan and will include additional gap cost-sharing
reductions for at least 10 percent of their formulary brand drugs.
In the CY 2012 Call Letter CMS explained that it does not believe that sponsors can demonstrate
meaningful differences based on expected OOPCs between two stand-alone basic Part D benefit
designs while maintaining both the statutory actuarial equivalence requirements and fulfilling the
requirement to maintain cost effective drug utilization review programs. As we approach CY
2020 and the coverage gap closes, CMS believes that Part D sponsors will find it difficult to
maintain three plans (a basic and at most two EA plans) that will meet the meaningful difference
test between all plans when the coverage gap is closed. Therefore, CMS encourages plan
sponsors to consider the impact of the coverage gap closing on their current and future plan
offerings to minimize future beneficiary disruption. We expect that for CY 2017 our application
of the meaningful difference standard will still allow us to approve up to 3 plan benefit packages
(1 basic and at most, two enhanced plans).
The methodology for developing the CY 2017 out-of-pocket costs (OOPC) model is consistent
with last year’s methodology. For more information, please reference the HPMS memorandum
dated December 18, 2015 titled “Medicare Plan Finder (MPF) Plan Version (V1) of Out-of-
Pocket Cost (OOPC) Model for CY 2016 and Updated Total Beneficiary Costs (TBC) Data
Released on HPMS.” Customary updates for utilization data, as well as PBP and formulary data
used for CY 2017 bid submissions, are also included in the 2017 model.
In the 2016 Call Letter, we proposed instituting a Total Beneficiary Cost (TBC) measure for
PDPs, similar to what has been in place for MAOs. The proposed change was intended to meet
CMS’s goals of establishing a more transparent and predictable process that beneficiaries can use
to select plans that meet their health care needs, while also being protected from high or
unexpected cost-sharing. After completing analysis and engaging in discussions with
200
stakeholders, CMS will not implement for CY 2017 an out-of-pocket cost (OOPC) or market
basket approach to set thresholds for increases in cost-sharing and premiums whereby we would
deny Part D plan bids with significant increases, pursuant to our authority in Section 3209 of the
Affordable Care Act. Instead CMS will calculate and publish the Part D TBC to support
transparency related to the out-of-pocket beneficiary costs year over year.

201
Table 19. Benefit Parameters
CY 2017 Threshold Values
Minimum Meaningful Differences (PDP Cost-Sharing OOPC)
1
Enhanced Alternative Plan vs. Basic Plan
$23
Enhanced Alternative Plan vs. Enhanced Alternative Plan
$34
Maximum Copay: Pre-ICL and Additional Cost- Sharing Reductions in
the Gap (3 or more tiers)
S
2,3
Preferred Generic Tier
<$20
4
Generic Tier
$20
Preferred Brand/Brand Tier
$47
Non-Preferred Drug Tier
$100
Non-Preferred Brand Tier
$100
Injectable Tier
$100
Select Care/Diabetic Tiers
5
$11
Maximum Coinsurance: Pre-ICL (3 or more tiers)
S
2,3
Preferred Generic Tier
25%
Generic Tier
25%
Preferred Brand/Brand Tier
25%
Non-Preferred Drug Tier
50%
Non-Preferred Brand Tier
50%
Injectable tier
33%
Select Care/Diabetic Tiers
5
15%
Maximum Coinsurance: Additional Cost-Sharing Reductions in the
Gap for Applicable Beneficiaries (all tier designs)
6
S
3
Preferred Generic Tier
31%
Generic Tier
31%
Preferred Brand/Brand Tier
60%
Non-Preferred Drug Tier
60%
Non-Preferred Brand Tier
60%
Injectable Tier
60%
Select Care/Diabetic Tiers
5
60%
Minimum Specialty Tier Eligibility
1-month supply at in-network retail pharmacy
$670
1
The Enhanced Alternative Plan to Basic Plan meaningful difference minimum threshold is based on the 50
th
percentile of
the October CY 2016 Bid Data run through the CY 2016 OOPC MPF model which incorporates CY 2016 Formulary Data,
2010/11 MCBS Data, and FDA data for brand/generic determinations related to coverage gap cost-sharing estimates. For each
parent organization, any cost-sharing OOPC comparison between a basic plan and EA plan in the same region must meet the
minimum Enhanced Alternative Plan vs. Basic Plan threshold. For each parent organization, any cost-sharing OOPC
comparison between two EA plans in the same region must meet the threshold established annually by CMS.
2
These thresholds are based on the 95
th
percentile of the CY 2016 Bid Data. As in previous years, we will also set similar
thresholds for plans with atypical tiering structures, such as a two tier formulary.
202
3
“S” in the above chart refers to “standard retail cost-sharing” at a network pharmacy. Standard retail cost-sharing (S) is cost-
sharing other than preferred retail cost-sharing offered at a network pharmacy.
4
Cost-sharing for the Preferred Generic Tier need only be lower than that for the cost-sharing of the Generic Tier. There is not
a separate maximum cost-share threshold for the Preferred Generic Tier.
5
The Select Care Drug and Select Diabetic Drug Tiers must provide a meaningful benefit offering with low or $0 beneficiary
cost-sharing for drugs targeting specific conditions (e.g., $0 tier for drugs related to diabetes and/or smoking cessation). The
coinsurance threshold for these tiers is derived from an average expected copayment amount using PDE data for drugs
submitted on preferred cost-sharing tiers. As noted earlier in this section, we continue to expect cost-sharing for the Vaccine
tier, or Select Care/Select Diabetes tiers that contain vaccines, to be $0.
6
Additional gap cost-sharing reductions for applicable beneficiaries are communicated in the PBP at the tier level and
sponsors may elect to provide this gap benefit for all drugs on a tier (full tier coverage) or a subset of drugs on a tier (partial
tier coverage). If the additional gap cost- sharing reduction benefit for a brand labeled tier applies to only non-applicable (i.e.,
generic) drugs or both generic and applicable drugs on that tier, then the generic drug beneficiary coinsurance maximum of
31% applies. Injectable, Specialty, Select Care and Select Diabetic Drug labeled tiers for which additional gap coverage is
offered, if any, will be analyzed in the same manner as brand labeled tiers with respect to beneficiary coinsurance maximums.
Note, the beneficiary coinsurance maximums for the coverage gap reflect the plan liability, but exclude the 50% manufacturer
discount for applicable drugs.
Specialty Tiers
Per 42 CFR 423.578 (a)(7), if a Part D plan sponsor maintains a formulary tier (the specialty tier)
in which it places very high cost and unique items, such as genomic and biotech products, the
sponsor may design its exception process so that very high cost or unique drugs are not eligible
for a tiering exception. Only Part D drugs with sponsor-negotiated prices that exceed an
established dollar-per-month threshold are eligible for specialty tier placement. The current cost
threshold of $600 was established in CY 2008.
In order to make sure that a Part D sponsor does not substantially discourage enrollment by
specific patient populations reliant upon these medications, CMS will only approve specialty
tiers within formularies and benefit designs that meet the standards set forth in Section 30.2.4 of
Chapter 6 of the Prescription Drug Benefit Manual. Part D sponsors offering prescription drug
benefit plans with a specialty tier are limited to the defined standard cost-sharing of 25%, if the
plan requires the standard deductible, and up to 33% cost-sharing if no deductible is required, or
some percentage in-between dependent on a decreased deductible. In return Part D sponsors are
shielded from tier exceptions for the most expensive drugs, and as a result would not need to
increase their bids or their Part D premiums to maintain actuarial equivalence.
As noted in the CY 2016 Call Letter, we continue to evaluate the specialty tier eligibility cost
threshold. The current $600 threshold repeatedly identified outlier prescription drug event
(PDE) data – less than one percent of 30 day equivalent fills exceeded $600. However, initial
analyses of 2015 PDE indicate that this percentage now slightly exceeds one percent. This,
coupled with the significant increase in the cost of Part D drugs since the last adjustment to the
specialty tier threshold, supports an increase in the specialty tier threshold for CY 2017. To

203
adjust the threshold, we propose applying the annual percentage increase used in the Part D
benefit parameter updates to the existing threshold. Thus, for CY 2017, the specialty tier cost
threshold will be $670. We may or may not increase the threshold on an annual basis moving
forward. Annually, we will test the proposed increased threshold and continue to perform other
analyses to assess whether threshold adjustments are necessary. To assist in future policy
decisions, we will also conduct a series of analyses to investigate 1) whether the inclusion of Part
D drugs on a specialty tier adversely affects drug utilization or enrollment decisions by certain
types of beneficiaries, and 2) the impact of tiering exceptions for specialty tier drugs.
To support CMS’s transparency initiatives, raise awareness, and educate beneficiaries on the cost
of prescription drugs and their impact on the Part D program, CMS intends to add a hyperlink on
the Medicare Plan Finder on Medicare.gov to the Medicare Drug Spending Dashboard, which is
published on CMS.gov, and estimates implementation for 2017 Open Enrollment in fall 2016.
Generic Tier $0 Copay Plans
Since the program began in 2006, use of lower cost generic alternatives by Medicare Part D
enrollees has been high and steadily increasing as single source drugs lose patent exclusivity.
However, low-income subsidy (LIS) enrollees continue to have lower use of generics compared
to enrollees without income subsidies. Lower generic use is often attributed to the small
differential between generic and brand drug copays legislatively mandated for LIS enrollees.
Changes in copay to increase cost differential between brand and generic drugs for LIS
beneficiaries requires Congressional authority; however, lowering the generic copay does not
and in 2012, 685 or 21.1% of plans offered generic-tier $0-copay plans. Of those 685 plans, 265
were PDP plans and 420 were MA-PD plans. We, therefore, explored the impact of enrollment
in generic-tier $0 copay plans on generic substitution rates between both LIS and Non-LIS
enrollees compared to enrollment in generic-tier non-$0 copay plans.
Using 2012 prescription drug event data, our analysis found that generic substitution rates (GSR)
for generic-tier $0 copay plans were 1.2 to 3.0 percentage points higher than in non-$0 copay
plans. This finding held true for both Enhanced PDP and MA-PD plans, and PDP Basic plans
for both LIS and non-LIS Part D populations. Within MA-PD Basic plans, GSR was not
statistically different for LIS or non-LIS populations, but there were very few MA-PD generic-
tier $0 copay basic plans. The lack of basic MA-PD plans is attributed to policy that does not
require MA plans to offer a basic plan if they offer an EA plan without a monthly supplemental
Part D premium in the same service area. Overall, if Part D enrollment were shifted from
generic-tier non-$0 into $0 copay plans, generic use could potentially increase. Even small
increases in generic use could mean significant savings to beneficiaries and to the Medicare Part
D program. However, our analysis is not without limitations. A complete description of the
study is found here: https://www.cms.gov/Medicare/Prescription-Drug-Coverage/
PrescriptionDrugCovGenIn/ProgramReports.html. At this time, CMS is providing these results
204
as informational only and as an opportunity for further discussion on ways to increase generic
use in Part D and in particular, the LIS population.
CMS has seen an increase in the number of plans with deductibles in 2016 compared to 2015.
Some of these plans have a $0 cost-share for generic drugs but require the beneficiary to meet a
deductible prior to receiving generic medications for free. One option available to Part D
sponsors is to provide first dollar generic coverage for medications on the $0 generic copay tier
by exempting the $0 cost-sharing tier from the deductible. CMS encourages plan sponsors to
consider first dollar coverage for generic medications and other ways to increase generic use in
the Part D program.
Part D Employer Group Waiver Plans (EGWPs)
Since January 1, 2014, supplemental benefits provided by employer group waiver plans
(EGWPs) beyond the parameters of the defined standard benefit are always considered non-
Medicare other health insurance (OHI). (See 77 Federal Register 22072 (April 12, 2012); and 80
Federal Register 7912 (February 12, 2015).) As a result of this change, we have continued to
receive industry questions regarding the effect, if any, it had on other EGWP and Part D rules.
The purpose of this guidance is to clarify CMS requirements for EGWPs with respect to some
Part D rules involving plan design and formularies that consistently have been the focus of these
and other inquiries.
Section 1860D-22(b) of the Social Security Act gives CMS the authority to waive or modify Part
D requirements that hinder the design of, offering of, or enrollment in EGWPs. All Medicare
Part D requirements apply unless explicitly waived or modified by CMS, and the waivers are
only available to those EGWPs that meet the circumstances and conditions imposed as part of
those waivers. See 42 CFR §423.458(c)(3) and (4). In general, Part D sponsors cannot offer
EGWPs with combined benefits (i.e., Part D plus employer OHI) with lesser value than the basic
Part D benefit nor establish benefit designs that substantially discourage enrollment by certain
Part D eligible beneficiaries. EGWPs must follow Part D rules in cases in which the provision of
employer OHI is inextricably intertwined with drugs offered under the Part D benefit such that
the two cannot be separated as a practical matter. (See also January 25, 2013 HPMS memo
including Insurance Standards Bulletin Series guidance: “Because the Affordable Care Act has
increased basic Part D benefits in the coverage gap, as of 2013 there will be very few claims that
do not contain some basic Part D benefits and would not ultimately be governed (as a practical
matter) by the Part D regulations.”)
As conditions of the waivers identified below, we remind Part D sponsors of EGWPs of the
following: (Please note that other conditions may attach to these waivers.)
Waiver: Part D sponsors offering EGWPs are not required to submit the same bid packages in
their entirety as are Part D sponsors of individual plans. Prescription Drug Benefit Manual
(PDBM), Ch. 12, EGWPs, §20.9. (For details, see 2016 HPMS Memo entitled “Release of the
205
2016 Plan Benefit Package and Bid Pricing Tool Software and Related Technical Bidding
Guidance for Part D Employer/Union-Only Group Waiver Plans” (April 10, 2015).
EGWP benefits (meaning, the Part D benefits, taking into consideration employer OHI)
must continue to meet the following applicable actuarial standards in 42 CFR
§423.104(e):
o Deductible is limited to no greater than defined standard deductible;
o Total Benefit is at least actuarially equivalent to the basic Part D benefit; and
o Catastrophic Benefit is at least actuarially equivalent to the basic Part D
catastrophic benefit.
See also PDBM, Ch. 12, EGWPs, §20.9.
Part D sponsors of EGWPs should take into consideration the annual established copay
and coinsurance tier maximum thresholds for Part D plans when designing their tiered
benefits to ensure they are not discriminating and discouraging certain beneficiaries from
enrolling in the EGWP. See 2012 final Call Letter, page 146 (April 4, 2011).
Waiver: EGWPs do not need to submit a unique formulary variation for each individual
employer/union sponsored group health plan. PDBM, Ch. 12, EGWPs, §20.14.
EGWPs that provide benefits with formularies will continue to:
o Submit for CMS approval through the HPMS formulary module a base formulary,
utilization management criteria, and transition policy that represent the minimum
drug benefit upon which all other formulary variations in the same plan must be
built. See 2015 final Call Letter, page 127 (April 7, 2014). In other words,
EGWPs cannot provide a formulary benefit that is less than what is included in
the base formulary.
Submit a base formulary which has the fewest drugs and the most
restrictive UM that any EGWP formulary variation will offer. For EGWPs
with multi-tiered formularies, submit the maximum number of tiers that
will be offered by any EGWP formulary variation in that same 800 series
plan and ensure each drug is placed on the tier where it has the highest
possible cost-sharing of any formulary variation. See 2015 final Call
Letter, page 127 (April 7, 2014).
Assign all EGWP 800 series Part D plans to a formulary through the
formulary crosswalk process. See Release of the Contract Year (CY) 2016
Bid Upload Functionality in HPMS (May 8, 2015 HPMS memo).

206
o Only make enhancements to approved formularies (i.e., enrich formularies) that
increase the value for any beneficiary who uses the drug(s). See 2015 final Call
Letter, page 127 (April 7, 2014).
o Follow all applicable (that is, non-waived) CMS rules, including those found in
PDBM, Chapter 6, Part D Drugs and Formulary Requirements, when restricting
access (often referred to as making negative maintenance and non-maintenance
changes) to drugs covered under the Part D benefit that appear in any EGWP
formulary (whether base or enriched). EGWPs restrict access when they, for
instance, remove drugs; increase cost-sharing; and impose or make more
restrictive existing prior authorization or step therapy requirements or quantity
limits. See PDBM, Ch. 12, EGWPs, §§10.1, 20.14. To provide further
clarification, please note:
When required by the circumstances of the negative change, we would
require EGWPs to, for instance, provide notice of the changes; exempt
affected enrollees from the proposed change for the plan year; update
formularies and other applicable beneficiary communications; and process
enrollee requests for exceptions.
EGWPs making negative changes to drugs on the base formulary must
request CMS approval through the HPMS negative change request (NCR)
module. In contrast, when an EGWP adds drugs to enhance the base
formulary, CMS does not require the sponsor to submit the additional
drugs in HPMS for CMS approval. See PDBM, Ch. 12, EGWPs, §20.14.
Subsequently, if an EGWP wanted to make a negative change to a drug
that was not included in the base formulary, as a matter of operations, it
would not be possible for the EGWP to submit a negative change request
for that drug through HPMS. Therefore, while we continue to require
EGWPs to follow all other applicable rules regarding negative changes to
drugs included under the Part D benefit that appear on an enriched EGWP
formulary, we do not require them to submit such changes to the HPMS
NCR module.
Improving Drug Utilization Review Controls in Medicare Part D
In the final 2013 Call Letter and supplemental guidance, CMS described a medication safety
approach by which sponsors are expected to reduce beneficiary overutilization of opioids and
maintain access to needed medications.
21
In July 2013, CMS launched the Overutilization
21
An excerpt from the Final 2013 Call Letter, the supplemental guidance and additional information about the OMS are available
on the CMS webpage, Improving Drug Utilization Controls in Part D (https://www.cms.gov/Medicare/Prescription-Drug-
Coverage/PrescriptionDrugCovContra/RxUtilization.html).

207
Monitoring System (OMS) to help oversee sponsors’ compliance with this CMS overutilization
guidance.
CMS continues to focus on and expect sponsors to further reduce opioid and acetaminophen
(APAP) overutilization in the Medicare Part D program. In this section, we describe the results
of Part D sponsors’ implementation of improved drug utilization controls to prevent
overutilization and improve medication use since January 2013, and our additional expectations
for further reductions of overutilization based on enhancements and clarifications of the policy.
We appreciate the comments and suggestions submitted by sponsors, PBMs, and other
organizations about the policies described below to reduce the unsafe overutilization of
medications by Part D beneficiaries and increase access to treatment.
Timeliness of beneficiary-level opioid point of sale (POS) edit submissions to the
Medicare Advantage and Prescription Drug System;
Discontinuation of OMS APAP reporting through the OMS;
Changes to the OMS opioid overutilization methodology;
Formulary-level cumulative morphine equivalent dose (MED) POS edits;
Soft opioid POS edit following initiation of buprenorphine -for the treatment of opioid
use disorder;
Access to medication-assisted treatment for opioid use disorder;
Elimination of utilization management processes that may lead to inappropriate use of
methadone in pain management.
In addition, the Enhancements to the 2017 Star Ratings and Beyond section of the 2017 Call
Letter discusses implementation of three new PQA-endorsed opioid overutilization measures.
New Expectation for Entering Opioid Point of Sale Claims Edit Information in the
Medicare Advantage and Prescription Drug System (MARx)
CMS enhanced MARx in February 2014 to automate the process by which sponsors notify other
sponsors about their beneficiary-level opioid POS claim edit decisions. In accordance with
current guidance, sponsors enter information in MARx when they have made a decision to
implement a beneficiary-level opioid POS claim edit. MARx then alerts a new sponsor when a
beneficiary identified in this manner by the previous sponsor enrolls in the new sponsor’s plan.
To facilitate data sharing between Part D sponsors, CMS has expected sponsors to submit POS
edit notifications into MARx in a timely manner, which we are now specifying as within seven
(7) business days of the date on the beneficiary’s written advance notice. CMS also expects
sponsors to submit implementations, terminations, and modifications of such POS edits within

208
seven (7) business days of the event. We encourage sponsors to use the MARx User Interface
for faster submissions than the batch file process; instructions are available in the Medicare
Advantage and Prescription Drug Plans Communications User Guide, which is available on the
CMS webpage, https://www.cms.gov/Research-Statistics-Data-and-Systems/CMS-Information-
Technology/mapdhelpdesk/Plan_Communications_User_Guide.html. As of March 10, 2016,
CMS has received 2,693 contract-beneficiary-level opioid POS edit notifications through MARx
for 2,520 unique beneficiaries.
Results of Overutilization Policy
Part D sponsors have had a significant impact on reducing overutilization of opioids and APAP.
From 2011 through 2015, there was a 47% decrease or 13,753 fewer Medicare Part D
beneficiaries identified as potential opioid overutilizers (i.e., beneficiaries with at least 90
consecutive days with greater than 120 mg MED daily with more than 3 prescribers and more
than 3 pharmacies contributing to their opioid claims). This represents a 57% decrease in the
share of beneficiaries using opioids who are identified as potential opioid overutilizers (see Table
20).
Table 20. OMS Part D Potential Opioid Overutilization Rates, 2011 – 2015*
Year
Total Part
D Enrollees
Total Part
D Enrollees
Utilizing
Opioids
% Part D
Enrollees
Utilizing
Opioids
Total Beneficiaries with at Least
90 Consecutive Days >120 mg
MED Daily AND
> 3 Prescribers &
> 3 Pharmacies for Opioid Claims
Difference Year-
to-Year
Share of
Opioid
Utilizers
Flagged as
Outliers
Difference in
Share Year-to-
Year
2011
31,483,841
10,049,914
31.9%
29,404
0.29%
2013
37,842,632
11,794,908
31.2%
25,347
− 4,057
0.21%
−0.08%
2014
39,982,962
12,308,735
30.8%
21,838
− 3,509
0.18%
−0.04%
2015
41,835,016
12,510,448
29.9%
15,651
− 6,187
0.13%
−0.05%
*Table 20 includes partial year inactive contracts, and hospice and cancer patients are excluded from utilizer and potential
overutilizer counts. For these opioid utilization comparisons, CMS used OMS methodology and prescription drug event (PDE)
TAP Data processed with cut-off dates in the early January of the following year.
47%
decrease
57%
decrease

209
The number of beneficiaries identified annually as potentially overutilizing APAP from 2011 to
2015, based on the CMS definition in the OMS, decreased by 94%, from 76,681 to 4,539 (see
Table 21).
Table 21. OMS Part D Potential APAP Overutilization Rates, 2011-2015*
*For these APAP utilization comparisons, CMS used OMS methodology and PDE TAP Data. For 2011, PDE TAP Data were
processed through 13AUG2012; subsequent year analyses used PDE TAP data processed with cut-off dates in the early January
of the following year.
Updates to Overutilization Policy for Contract Year (CY) 2017
Discontinuation of APAP Reporting through the OMS
Since the annual number of beneficiaries overutilizing APAP has decreased dramatically since
2011, we will discontinue the reporting of APAP overutilization tickets in the OMS beginning
with the April 2016 OMS reports. However, we will continue to monitor APAP overuse through
a new Patient Safety measure. The High APAP Daily Dose Rate will be defined as the number
of APAP days exceeding a 4 g daily dose (DD) per 1,000 APAP user days, and will be reported
for CY 2016 at the contract level for information purposes only. We will also identify outliers at
the contract level, and will implement new outlier response requirements beginning in 2017
similar to the process used for other Patient Safety measures. The current Patient Safety outlier
methodology can be found on the Patient Safety Website under Documentation › Help
Documents › Outlier Threshold Reports. CMS thanks sponsors for their APAP utilization
efforts, encourages continuation of these efforts, and reinforces that implementation of APAP
safety edits based on FDA labelling do not require a formulary submission to CMS.
Opioids
Compliance Activities and Changes to the OMS Opioid Overutilization Methodology
Since the OMS was launched in July 2013, CMS has used the following criteria to identify
beneficiaries who may potentially be overutilizing opioids:
Year
Total Part
D Enrollees
Total Part
D Enrollees
Utilizing
APAP
% Part D
Enrollees
Utilizing
APAP
Total Beneficiaries with Daily
APAP Dose Exceeding 4 g for 30
or More Days Within Any Six-
month Period with at Least One
Day Exceeding 4 g Within the
Most Recent Calendar
Difference Year-
to-Year
Share of
APAP
Utilizers
Flagged as
Outliers
Difference in
Share Year-to-
Year
2011
31,483,841
9,449,693
30.0%
76,581
0.81%
2013
37,842,632
10,591,651
28.0%
26,122
−50,459
0.25%
−0.56%
2014
39,982,962
10,845,499
27.1%
6,286
−19,836
0.06%
−0.19%
2015
41,835,016
10,712,430
25.6%
4,539
−1,747
0.04%
−0.02%

210
Use of opioids with cumulative daily MED exceeding 120 mg for at least 90 consecutive
days with more than 3 prescribers and more than 3 pharmacies contributing to their
opioid claims, during the most recent 12 months, excluding beneficiaries with cancer
diagnoses and beneficiaries in hospice.
In the 2015 Call Letter, we described our concern that some sponsors’ internal criteria or
processes to identify and address potential opioid overutilization may be insufficient. For the
January 2014 OMS reports, 67% of the potential opioid overutilization responses were that the
beneficiary did not meet the sponsor’s internal criteria (OMS response code BSC). CMS also
announced that beginning January 2015, sponsors’ internal opioid criteria for retrospective
identification of egregious patterns of opioid overutilization and subsequent case management
should be no less restrictive than 120 mg daily MED over at least 90 consecutive days.
22
Other
criteria, such as the number of prescribers and pharmacies, could vary from CMS specifications.
Sponsors may also vary the measurement period, and our understanding is that most sponsors
look back 90 to 120 days.
Continued review of sponsors’ responses to the OMS in 2015 suggested potential noncompliance
with CMS guidance. In light of this, we performed additional outreach to assess compliance
with CMS guidance by select Part D sponsors who were identified as outliers based on their
APAP and opioid responses to the OMS. CMS contacted Part D sponsors at the parent
organization level to obtain information about their overutilization criteria and case management
programs, and for the sponsors to explain their responses to specific tickets received through the
OMS. Overall, we found that sponsors were generally compliant with CMS guidelines.
Based on our analysis of the information from this effort, we identified opportunities to
potentially modify the OMS opioid overutilization criteria in the future (as early as 2018) to
reduce the number of tickets for which sponsors repetitively submit response codes BSC (No
further review planned: Beneficiary did not meet the sponsor’s internal criteria) and BOR
(Beneficiary-level POS edit determined not necessary: Beneficiary’s overutilization resolved).
Ideas include to:
Shorten the measurement period from 12 months to 6 months; and
Use average MED rather than a count of 90 consecutive days of high MED.
The revised ‘Overutilization of Opioids’ criteria would be:
Use of opioids with an average daily MED exceeding 120 mg for an episode of at least
90 days with more than 3 prescribers and more than 3 pharmacies contributing to their
22
Note: The OMS ‘Overutilization of Opioids’ criteria was developed and the compliance activities occurred prior to the recent
publication of the CDC Guideline for Prescribing Opioids for Chronic Pain discussed later in the Call Letter. We will consider
changes to the criteria based on the CDC Guideline for presentation in the 2018 Call Letter.
211
opioid claims, during the most recent 6 months, excluding beneficiaries with cancer
diagnoses and beneficiaries in hospice.
The average MED is calculated by summing each PDE’s MED and dividing this sum by the
duration of the opioid episode in days. An opioid episode consists of at least two opioid PDE
fills. The episode duration is the number of days between the first and last opioid PDE’s
dispensing date during the measurement period plus the last PDE’s days’ supply plus 1 day (end-
date). If the end-date is beyond the last day of the measurement period, the quantity is multiplied
by the percent of the days’ supply that occurs during the measurement period, and the end-date
becomes the last calendar day of the measurement period.
By allowing gaps between prescription fills and days’ supply in the calculation, the average
MED per 90-day episode methodology may identify more beneficiaries who are chronic users of
high opioid doses than the consecutive days method. Shortening the measurement period from 12
months to the most recent 6 months may better identify current potential overutilization and
reduce the number of repeat cases reported by the OMS. We are analyzing the impact of these
potential revisions in identifying beneficiaries who may potentially be overutilizing opioids.
In addition, CMS is investigating how prescribers are counted in the OMS opioid overutilization
criteria. We are analyzing the feasibility of grouping NPIs (National Provider Identifiers) within
a clinical practice as reported in the Medicare Provider Enrollment, Chain, and Ownership
System (PECOS) rather than count unique NPIs, which would reduce false positives in the group
practice setting. Suggestions include grouping based upon Tax ID number (TIN), Employer ID
number (EIN), or primary location address. Identifying common clinical practice groups based
on prescribers whose NPIs are associated only with one primary location TIN or a single EIN
could prevent mismatching of prescribers who participate in multiple clinical practices. This
conservative grouping methodology resulted in a 4.8% decrease in the number of beneficiaries
potentially overutilizing opioids that would have been identified by the OMS in the October
2015 cycle.
We thank those commenters who offered suggestions on how to improve the metric and the
grouping of NPIs. CMS plans to continue to investigate potential modification of this measure
for implementation in 2018 based on experience from compliance activities, additional analyses,
and the CDC guideline (as described further below).
Other findings and takeaways from our compliance activities include:
Sponsors should review repeat OMS response replies. For example, instead of
resubmitting the BSC response code repeatedly for the same case, sponsors may
confirm medical necessity with the prescribers. The DMN (Determined Medically
Necessary) response code triggers the OMS exception logic for one year.
Although several morphine equivalent conversion factors exist, CMS encourages

212
sponsors to use the CDC morphine milligram equivalent (MME
23
) conversion factors
within their opioid overutilization programs. The MME conversion table is available
on the CMS webpage, Improving Drug Utilization Controls in Part D
(https://www.cms.gov/Medicare/Prescription-Drug-Coverage/
PrescriptionDrugCovContra/RxUtilization.html), which contains information to help
Part D sponsors create or revise their programs to address the unsafe use of opioid
pain medications.
We thank the sponsors that participated in this outreach effort. We were not only able to assess
potential non-compliance, but we gained information on ways to improve our guidance and
overutilization methodology.
CMS’ Expectation for Formulary-Level Cumulative Opioid POS Edits in CY 2017
Although the overutilization of opioids has decreased in Part D as discussed above, CMS has
indicated on multiple occasions that we believe Part D sponsors should implement formulary-
level cumulative opioid edits at POS to prospectively prevent opioid overutilization. Industry
reaction had previously been that such edits were premature due their complexity. As described
in the final 2016 Call Letter, we commenced a pilot project in 2015 to assess the feasibility and
impact of such POS edits.
Through the pilot project, we noted that Part D sponsors demonstrated that they can effectively
implement a soft or hard formulary-level cumulative opioid MED edit at POS while blocking the
edit for beneficiaries with known exceptions. The sponsors evaluated their own data when
developing edit specifications and exclusion criteria to identify potential opioid overutilization
while maintaining access to opioids when needed for their enrollees. Formal complaints were
not received from beneficiaries or providers. Additional information about the pilot project
experience was described in the draft CY 2017 Call Letter.
For CY 2017, we proposed that sponsors’ implement both the soft and hard
24
cumulative MED POS edits. Soft edit claim rejections could be overridden at the
pharmacy level by the pharmacist submitting appropriate NCPDP codes, and with
respect to hard edit claim rejections, the rejected prescription drug claim would not be
approved in the absence of a plan decision to override the edit. In the draft Call
Letter, we proposed the following parameters for the POS edits: Soft edits that can be
overridden at the pharmacy level when a prescription claim will result in the
23
Note: CDC’s terminology, morphine milligram equivalents (MME), is equal to morphine equivalent dose (MED) in milligrams
as used by CMS. Often calculated as a daily dose.
24
More information about soft and hard rejects and edits is available from the Medicare Prescription Drug Benefit Manual
Chapter 6 – Part D Drugs and Formulary Requirements, https://www.cms.gov/Medicare/Prescription-Drug-
Coverage/PrescriptionDrugCovContra/Downloads/Part-D-Benefits-Manual-Chapter-6.pdf, and the National Council for
Prescription Drug Programs: “Telecommunication Version D and Above Questions, Answers and Editorial Updates,” NCPDP,
February 2014, http://www.ncpdp.org/NCPDP/media/pdf/VersionD-Editorial.pdf (accessed 1/22/2015).

213
beneficiary’s active or overlapping opioid prescriptions reaching or exceeding a
certain daily cumulative MED threshold. This threshold may be set at 90 mg to 120
mg MED. The soft-edit rejection can be overridden by the pharmacist submitting
appropriate NCPDP codes.
Hard edits for daily cumulative MED threshold at or above 200 mg MED.
We also described methods to minimize false positives by accounting for known exceptions.
Commenters supported our original proposal for both types of edits, and some supported only
soft or hard edits for CY 2017. Others expressed concern for potential delay of beneficiary
access to needed medications, the short time between the final Call Letter and the formulary
submission deadline, and the need for more time to develop, test, and implement the edits. Due
to the comments received, we are revising our expectations for CY 2017 formulary-level
cumulative opioid MED POS safety edits. For CY 2017, we expect sponsors to implement either
a soft edit or a hard edit, or they may use both soft and hard edits as we originally proposed in
the draft Call Letter, and work toward a hard edit at a minimum in 2018 using reasonable
controls to limit false positives. We will review 2016 and 2017 experience with these edits to
inform content in the CY 2018 Call Letter.
For CY 2017, we expect sponsors’ Pharmacy and Therapeutics (P&T) committees to develop the
specifications for their formulary-level cumulative MED POS edit(s) based on the opioid
overutilization in their Part D plans, and reasonable numbers of targeted beneficiaries for plan
oversight. We recommend that a soft opioid edit threshold should be set at levels no lower than
90 mg MED, and a hard opioid edit threshold should set no lower than 200 mg MED. We also
expect sponsors to apply specifications to minimize false positives by accounting for known
exceptions, such as hospice care, certain cancer diagnoses, reasonable overlapping dispensing
dates for prescription refills or new prescription orders for continuing fills, and high-dose opioid
usage previously determined to be medically necessary such as through coverage determinations,
prior authorization, case management, or appeals processes. If sponsors decide to include a
provider count criterion in the soft or hard edit specifications, we recommend two prescribers of
the active opioid prescriptions as the threshold (at a minimum). We also do not recommend a
consecutive high-MED days criterion because it would not prevent beneficiaries from reaching
high opioid doses.
In order to allow more time to develop and test the full edit specifications, Part D sponsors will
have until September 1, 2016 to submit the detailed operational information to CMS for review.
The documentation must include information such as the type of edit(s), the MED level being
utilized, exclusion criteria, and other screening information, as well as a written description of
the program’s mechanics, including the mechanism by which the edits will be resolved. This
information must be submitted via e-mail to [email protected] with a subject line
of “Cumulative MED – [applicable FID number].” A submission template will be provided to

214
Part D sponsors’ formulary contacts at a later date. Finally, we wish to clarify the HPMS
formulary submission requirements with respect to quantity limits. Opioids that have a quantity
limit that is below any applicable FDA-approved maximum doses must be submitted as part of
the HPMS formulary submission. However, if the only quantity restriction that will be applied at
POS is a cumulative MED edit described in this section, a quantity limit does not need to be
reflected on the HPMS formulary submission. The cumulative MED edit is considered to be a
safety edit. This guidance updates that which is included in section 30.2.2.1 of Chapter 6 of the
Medicare Prescription Drug Benefit Manual. We are also clarifying that non-formulary opioids
can be included in the cumulative MED editing even though they are not included on the
formulary.
Concurrent Use of Opioids and Buprenorphine
As described in the 2016 Call Letter, we investigated the concurrent use of buprenorphine and
opioids in Part D as a potential new measure for the OMS as informational only. Currently, the
sublingual (SL) and buccal formulations of buprenorphine and buprenorphine-naloxone film or
tablets are only approved by the Food and Drug Administration (FDA) for the treatment of
opioid use disorder and not for the treatment of pain. Because buprenorphine effectively blocks
the analgesic properties of other opioids used to treat acute pain, it generally prevents the use of
other opioids as an adjunctive treatment for pain syndromes.
An analysis of PDE data from April 1, 2014 through March 31, 2015 identified over 24,500
Medicare Part D beneficiaries with concurrent buprenorphine buccal and SL formulations and
opioid use, including over 20% with 30 or more concurrent opioid days. CMS believes there are
additional opportunities for improvements through drug utilization management. Therefore, we
expect sponsors to implement a soft POS edit when an opioid prescription is presented following
the initiation of buprenorphine for the treatment of opioid use disorder. CMS believes that a soft
edit that only rejects the opioid prescription following the buprenorphine claim should not
impede access to buprenorphine for the treatment of opioid use disorder. It is very important that
a sponsor should only implement this edit if it has the technical ability to not reject
buprenorphine claims. At this time, we will not include a measure of concurrent use of opioids
and buprenorphine in the OMS, but we will continue to monitor utilization trends. For additional
guidance in the use of buprenorphine in the treatment of opioid use disorders refer to
http://buprenorphine.samhsa.gov/Bup_Guidelines.pdf.
Concurrent Use of Opioids and Benzodiazepines
CMS is also concerned with the concurrent use of opioids and benzodiazepines, and we want to
raise public awareness of this important issue. The combination of opioids and benzodiazepines
can exacerbate respiratory depression, the primary factor in fatal opioid overdose. The risk of
opioid-related morbidity and mortality is increased in all patients, even those who do not show
signs of aberrant drug behavior. In a 2015 study, investigators found that 49% of a study

215
population who died from a drug overdose while taking opioid analgesics were concurrently
prescribed benzodiazepines.
25
Further, the CDC advises clinicians to avoid prescribing opioids
and benzodiazepines concurrently whenever possible.
26
We found through analysis of 2015 PDE data (as of March 2016) that almost 3.1 million
beneficiaries were dispensed an opioid medication with at least one day overlap with a
benzodiazepine medication, excluding beneficiaries enrolled in hospice or with a cancer
diagnosis. This represents 24% of opioid users and 8% of Part D enrollees (non-hospice/non-
cancer). Also, about one-third of beneficiaries concurrently utilizing opioids and
benzodiazepines only had one event (most less than 30 days), whereas over two-thirds had more
than one event of overlap usage. The top three opioid and benzodiazepine combinations by
number of events in 2015 included hydrocodone-acetaminophen with alprazolam, lorazepam, or
clonazepam. We encourage Part D sponsors to evaluate their claims data and use drug utilization
management tools that are available to them as necessary to help address the concurrent use of
these drug classes.
CMS will continue to monitor concurrent use of opioids and benzodiazepines among Medicare
Part D enrollees. Also, we are aware that a measure concept, Double Threat: Concurrent Use of
Opioids and Benzodiazepines, is in development by the PQA, which may be considered for
future use in oversight or performance measurement.
Access to Medication-Assisted Treatment
Despite efforts such as those outlined above, opioid use disorder continues to be a significant
public health concern. In October 2015, the President issued a Memorandum to Federal
Departments and Agencies to identify barriers to medication-assisted treatment (MAT) for
opioid use disorders and develop action plans to address these barriers. In response, CMS will
use available vehicles to inform physicians, MA organizations and Part D sponsors about MAT
coverage, including clarifying that MA plans have the same obligation to cover substance use
disorder treatment as is available under Original Medicare and that Part D plans must ensure
access to MAT that are covered under Medicare Part D.
Currently only buprenorphine, buprenorphine/naloxone, and naltrexone are covered Part D drugs
when used for medication-assisted treatment (MAT) of opioid use disorder. It is critical that
Medicare beneficiaries who are in need of these therapies have appropriate access to these drugs
in Part D. Given the requirements imposed by the Drug Addiction Treatment Act of 2000 and
Risk Evaluation and Mitigation Strategy for buprenorphine-containing products for MAT, Part D
sponsors should not impose prior authorization criteria that simply duplicate these requirements.
When prior authorizations are utilized, Part D sponsors must also carefully consider approval
25
Park TW, Saitz R, Ganoczy D, et al. Benzodiazepine prescribing patterns and deaths from drug overdose among US veterans
receiving opioid analgesics: case-cohort study. BMJ 2015;350:h2698.
26
http://www.cdc.gov/drugoverdose/prescribing/guideline.html.

216
durations so as to not subject beneficiaries who are in need of these therapies to unnecessary
hurdles or lapses in treatment. Part D formulary and plan benefit designs that hinder access,
either through overly restrictive utilization management strategies or high cost-sharing, will not
be approved.
Under current statute, methadone, an FDA-approved medication for the treatment of opioid use
disorder, is not covered by Part D for substance use disorder treatment because it does not meet
the Part D requirement that it “may be dispensed only upon a prescription” since it must be
dispensed in an opioid treatment program and cannot be dispensed upon a prescription at a
pharmacy when used for this purpose. We appreciate comments submitted on whether or not
this statutory requirement is a barrier to treatment. Absent a change in law, Medicare is unable
to cover methadone for MAT under Medicare Part B or Part D. However, under Part C, MA
organizations may cover methadone for MAT as a supplemental benefit.
A Note about the Centers for Disease Control and Prevention (CDC) Guideline for
Prescribing Opioids for Chronic Pain
The CDC prepared a guideline for opioid prescribing to assist primary care providers in
delivering safer, more effective chronic pain management for patients with pain outside of active
cancer treatment, palliative care, and end-of-life care. The guideline, which was published on
March 15, 2016, was developed through a rigorous scientific process using subject matter
experts, the most recent scientific evidence, and public comment. Topics include 1) when to
initiate or continue opioids for chronic pain; 2) opioid selection, dosage, duration, follow-up, and
discontinuation; and 3) assessing risk and addressing harms of opioid use, including the use of
opioids in patients age 65 and older. In the guideline, CDC identifies 50 mg MME daily dose as
a threshold for increased risk of opioid overdose, and to generally avoid increasing dosage to 90
MME per day. The guideline also presents tapering methodology for long-term, high opioid
dose users, which may be useful to reduce high opioid doses. We encourage sponsors’ P&T
committees to carefully review and consider CDC’s recommendations, and to share the CDC
guideline with opioid prescribers. The CDC Guideline for Prescribing Opioids for Chronic Pain
is available on the CDC website at http://www.cdc.gov/drugoverdose/prescribing/guideline.html.
During 2016, we will consider potential revisions to CMS overutilization guidance and the OMS
opioid overutilization methodology based on the CDC guideline, for presentation in the 2018
Call Letter. In addition, we will consider recommendations set forth in the guideline during the
CY 2017 formulary and benefits review. For example, CDC notes that methadone has been
associated with a disproportionately high number of overdose deaths relative to its prescribing
frequency for pain management. As a result, the guideline states that methadone should not be
used as a first line agent for pain management when an extended-release/long-acting opioid is
indicated, and that only providers who are familiar with the complexities of methadone’s
pharmacokinetic and pharmacodynamics properties should prescribe it for pain. Part D sponsors
should evaluate their utilization management strategies and eliminate processes that may lead to
217
inappropriate utilization of methadone in pain management. Submitted Part D benefit packages
and formularies will be reviewed to ensure that methadone is not the sole preferred opioid
analgesic within a plan design.
Point of Sale Pilot
In the draft Call Letter, CMS provided an overview of the Point of Sale (POS) pilot we
conducted in 2015. We shared initial takeaways from the pilot and solicited feedback from
stakeholders on: (1) how CMS and Part D plans might reduce the volume of rejected claims on
the front end by resolving certain issues before the prescription arrives at the pharmacy; and (2)
how plans might employ proactive processes to resolve certain POS issues without the enrollee
having to request a coverage determination.
Most of the comments we received about the POS pilot were generally supportive of the
project’s goals to reduce rejected claims at the POS when possible, and explore ways to reduce
unnecessary delays in access to needed drugs. Several commenters asked for clarification on any
guidance CMS will provide for future changes to POS processes, including potential regulatory
changes, and more information about the pilot findings. A few commenters asked for
clarification on whether initiation of a proactive outreach approach starts the clock on a coverage
determination, or whether denial notices would be required if proactive outreach does not result
in authorization of the requested drug.
Overall, commenters expressed a range of concerns about potential policy changes in this area.
Some commenters, while noting that the pilot was a positive step toward improving beneficiary
access to needed drugs, also expressed concerns about the methodology, including the usefulness
of findings without benchmark data for comparison and a lack of information about how the pilot
may have impacted affected beneficiaries. Other commenters stated a belief that the pilot was
too limited in scope to form the basis of a regulatory change, recommended seeking more
industry feedback before introducing new requirements, and underscored the need to allow plans
and PBMs sufficient time to make any necessary systems or process modifications before any
required changes become effective. A few commenters voiced concerns that the proactive
outreach developed and tested in the pilot represents an additional financial and operational
burden on plan sponsors, and provided no added benefit to enrollees or the program. Comments
related to implementation of a potential policy change varied: some commenters recommended
that changes allow for flexibility, one commenter requested that CMS identify target drugs, and
another commenter stated that any proposed changes should not circumvent the existing
coverage and appeals process by creating a new flexible, informal process for plans/PBMs that
would lack transparency and be difficult to oversee.
A number of commenters responded to our request to identify additional means to address POS
issues, and we thank them for their responses. Commenters offered a variety of suggestions,
including:
218
CMS could develop additional guidance and requirements related to electronic
prescribing (eRx) and electronic prior authorization (ePA), which the commenter believes
will increase adoption of eRx and the more consistent use of a single standard for ePA;
Part D plan sponsors could improve existing or implement new review of enrollee claims
history to facilitate authorizations when appropriate;
MA-PD plans could leverage existing provider contracting arrangements to make
formularies more accessible to prescribers who are contracted with the plan; and
CMS could consider how lessons learned from the POS Pilot might be applied to the Part
D Enhanced MTM Model Test.
We received a few additional comments related to the Part D coverage and appeals process
generally which were outside the scope of the POS pilot and will not be addressed in the Call
Letter. We thank all commenters for sharing their feedback, ideas and concerns related to this
project.
After analyzing the results of the pilot and the comments received in response to the draft Call
Letter, we agree that additional exploration of these issues is warranted before proposing any
regulatory changes, and CMS will not impose changes to operational requirements for the 2017
plan year. While we made sure to include a variety of organizations in the pilot—large and small
plans, standalone Part D and MA-PD plans, and PBMs—all participants expressed concerns
about the resources necessary to implement their varied proactive outreach processes on a larger
scale, including the need to spend more time conducting outreach to prescribers to obtain
necessary information than is generally needed during the coverage determination process.
Participants and CMS have concerns about diverting plan resources from the coverage
determination process to a proactive process to resolve POS issues where the enrollee has not
requested a coverage decision and believe this approach may not provide the most benefit to
enrollees.
While we appreciate commenters’ concerns about the methodology of the pilot, we believe our
flexible approach yielded robust and varied findings. By allowing participants to devise their
own processes and select which drugs to target, we obtained information on where flexibility
could maximize the benefit for enrollees and minimize any additional burden on plans, PBMs,
and prescribers. This methodology also gave us insight into where we might target continued
exploration of POS issues by seeing where varied organizations diverged in process design, drug
selection, and ideas that went beyond the framework CMS initially devised. Additionally, one of
the main reasons CMS conducted this pilot was to explore potential solutions to POS issues
without the enrollee having to take action, and to more seamlessly address situations where
beneficiary advocacy groups have advised CMS that enrollees can be confused by the coverage

219
determination process and uncertain about what action they should take when a pharmacy claim
rejects under Part D.
Despite our concerns about the significant resources needed for, and potential limits of, a
proactive process to resolve rejected claims, we identified multiple opportunities to address POS
issues which CMS will continue to explore to develop best practices and potential future policy
changes. These opportunities include developing additional guidance and exploring additional
requirements related to eRx and ePA to increase adoption of these technologies, testing the use
of “smart edits” where information is or could be made available in real-time to allow certain
claims to favorably auto-adjudicate at the POS, and further exploring how certain rejected claims
may be targeted for proactive outreach in concert with existing rejected claim review and MTM
requirements. We agree with many commenters that additional research in these areas is
advisable before suggesting best practices or implementing new requirements on a larger scale.
We do, however, encourage Part D sponsors to continue to analyze POS access issues, and to
identify methods for resolving POS edits whenever possible without the beneficiary having to
take action, such as initiating or expanding rejected claims review processes. We also encourage
Part D plans and PBMs to continue to share ideas and information, as well as questions and
concerns with CMS, by sending an email to [email protected].
On January 21, 2016, CMS hosted a conference call and invited the pilot participants to share
information about their experiences in the pilot with other Part D plan sponsors, PBMs and
interested stakeholders. Participants discussed how they identified target drugs, the processes
they developed for outreach, challenges and successes of the process, resource allocation and
comparison to the coverage determination process, and recommendations for any CMS policy
changes, including ideas for increasing prescriber awareness of formulary information at the
point of care. We have recently posted presentation materials, as well as the audio recording and
transcript of that call on the CMS website at https://www.cms.gov/Medicare/Appeals-and-
Grievances/MedPrescriptDrugApplGriev/index.html.
While CMS is not imposing any new operational requirements for 2017, we want to take this
opportunity to remind MA-PD plans of the new requirements at 42 CFR §422.112(b)(7), which
became effective January 1, 2016. MA-PD plans are required to coordinate all Medicare benefits
administered by the plan for prescription drugs that may be provided under Part B or Part D by
establishing and maintaining a process to ensure timely and accurate POS transactions, and to
issue a decision and authorize or provide the benefit as appropriate under Part B or Part D when
a party requests a coverage determination. CMS intends to develop additional subregulatory
guidance for MA-PD plans related to our expectations for coordination of benefits when drug
claims are rejected at the POS because of a B v. D prior authorization requirement.
220
Extended Days’ Supply and First Fill Quantity Limits
Part D sponsors that offer an extended (2 or 3 month) days’ supply are not required to uniformly
apply this benefit across each tier. Sponsors must indicate in the plan benefit package (PBP) if
an extended days’ supply for a given tier applies across an entire tier, or applies only to a subset
of drugs on a tier. Currently there is no process for sponsors to indicate which specific drugs on
a partial extended days’ supply tier qualify for extended days’ supplies verses those drugs that do
not.
In an effort to increase transparency, beginning in CY 2017, sponsors that indicate a partial
extended days’ supply tier within their PBP will be required to submit the specific drugs not
available as extended days’ supply as an HPMS supplemental file. This file (“Non-Extended
Day Supply”) includes the RXCUIs that will not be available as an extended days’ supply during
initial formulary submission and as necessary during formulary update window submissions.
Detailed submission guidance will be provided during the formulary submission training at a
later date.
Part D sponsors of EGWPs offering this option will not be required to provide a “Non-Extended
Day Supply” supplemental file because they do not complete the Medicare Rx section of the
PBP. We continue to require EGWPs to otherwise follow non-waived rules governing extended
days’ supply.
We understand many plans offer beneficiaries 2 or 3 month supplies of medications as a
convenient and potentially cost saving option. However, consistent with good medical practice,
it can often be appropriate for the prescriber to follow up sooner with a patient starting a new
therapy. This is especially true in the case of complex therapies or drugs with a narrow
therapeutic index or a high risk of side effects. With any multi-day fill there is the potential that
a patient’s dose may change or he or she discontinue therapy due to side effects, adverse
reactions, or lack of clinical response. In these cases, the remaining amount of medication is
often wasted. The potential for drug waste is especially pronounced when starting on a new drug
therapy, as the effectiveness and tolerability are unknown for the patient. Dispensing a 2 or 3
month supply as a first fill to a patient who is naïve to therapy may result in excessive waste, as
well as unnecessary expense, if the patient ultimately does not use the full amount dispensed.
Starting in 2017, plan sponsors will now also have the option to indicate in the PBP at the tier
level if any drugs are available for an extended days’ supply on all but the first fill. This change
allows sponsors to designate drugs where they will only cover up to a one month supply the first
time the drug is filled, providing an opportunity to limit drug waste when a new therapy is not
working for the patient or has adverse effects. While some prescribers may choose to schedule
another visit with a patient beginning a complex therapy to determine the need for adjustments or
discontinuation of therapy, Part D sponsors may not require such a step or a new prescription for
221
the second fill to be covered for the extended days’ supply. After the first one month supply, the
change to extended days’ supply should be seamless for the beneficiary.
Given the support received, sponsors will be permitted to implement this starting in 2017;
however, the specific drugs available for an extended days’ supply on all but the first fill will not
be included in an HPMS supplemental file for 2017. Sponsors should make clear in beneficiary
materials information about first fill quantity limits and which drugs are affected.
Establishing Mail Order Protocols for Urgent Need Fills to Prevent Gaps in Therapy
Many Part D sponsors contract with mail order pharmacies to offer beneficiaries an alternative
way to fill prescriptions under the Part D benefit, often at much lower cost-sharing than is
available at network retail pharmacies. While mail order pharmacies make up a relatively small
percentage of total prescriptions filled under the Part D program, we are committed to ensuring
consistent and reliable beneficiary access to medications, regardless of what type of pharmacy
fills the prescription.
One aspect of providing consistent access includes responding to urgent medication needs.
Various scenarios can result in a beneficiary running out or having only a small amount of a
medication remaining, such that a standard mail order fill may arrive too late to avoid a gap in
therapy. As stated in §423.120, a Part D sponsor’s contracted pharmacy network may be
supplemented by non-retail pharmacies, including pharmacies offering mail order, provided the
requirements assuring pharmacy access are met. In our experience, under such circumstances
some Part D sponsors direct their enrollees to retail pharmacies to obtain a needed medication.
Other sponsors provide rush orders (e.g., next day delivery) from mail order pharmacies to
supply the medication.
CMS has received beneficiary complaints about mail order pharmacies indicating that they will
rush ship an urgently needed order, but the order does not arrive when promised or at all,
potentially resulting in gaps in therapy. To protect beneficiaries from inconsistent or unreliable
practices that may jeopardize timely access to medications, CMS expects Part D sponsors to
work with their mail order pharmacies to develop and implement protocols for providing access
to urgently needed medications. Further, beneficiaries should be informed of their options when
requesting a rush order, with clear steps detailed in all applicable beneficiary materials. Having
established protocols and beneficiary information in place can streamline how sponsors respond
to such needs. We expect sponsors to have protocols in place to address how to handle urgently
needed medication requests from beneficiaries by CY 2017 if not sooner and to be able to clearly
communicate this to their beneficiaries. We will continue to monitor complaints for issues
related to mail order or access to urgently needed medications.

222
Coordination of Benefits (COB) User Fee
CMS is authorized to impose user fees on Part D sponsors for the transmittal of information
necessary for benefit coordination between sponsors and other entities providing prescription
drug coverage. We review and update this user fee annually to reflect the costs associated with
COB activities for the specific year. The 2017 COB user fee will be collected at a monthly rate
of $0.116 for the first 9 months of the coverage year (for an annual rate of $0.087 per enrollee
per month) for a total user fee of $1.05 per enrollee per year. Part D sponsors should account for
this COB user fee when developing their 2017 bids.
In contract year 2017, we will use the COB user fees for activities including:
Part D Transaction Facilitator operation and maintenance;
The Benefit Coordination and Recover Center (BCRC) operation and maintenance;
Drug data processing system management, which is used to collect prescription drug
event (PDE) data for Part D payment purposes and to produce invoices for the coverage
gap discount program;
Medicare Advantage and Prescription Drug System (MARx) management of COB data;
and
Review of Workers’ Compensation settlement set-aside funds, which verify that medical
services are paid for by the appropriate party
Part D Low Enrollment
CMS has the authority under 42 CFR §423.507(b)(1)(iii) to non-renew Part D plans (at the
benefit package level) that do not have sufficient number of enrollees to establish that they are
viable plan options. While we are particularly concerned with plans that have fewer than 500
enrollees, we urge sponsors to voluntarily withdraw or consolidate any stand-alone plan with less
than 1,000 enrollees. Sponsors are strongly encouraged to view data on plan enrollment at:
https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/
MCRAdvPartDEnrolData/index.html to determine if any of their plans meet this criterion. By
April 2016, we will notify plans with less than 1,000 enrollees of available options for
consolidation/withdrawal options. We reserve the right to require low enrollment plans to
consolidate/withdraw in the future based on the marketplace at that time to ensure that all Part D
plans offered in the marketplace are attractive to beneficiaries and do not add to their confusion
in selecting a plan best suited to their prescription drug coverage needs.
223
Section IV – Medicare-Medicaid Plans
Medicare-Medicaid Plan Annual Requirements and Timeline for CY 2017
This section provides an overview of the contract year (CY) 2017 Medicare requirements and
timeframes for Medicare-Medicaid Plans (MMPs). We will also provide guidance shortly after
the issuance of the Final CY 2017 Call Letter about which provisions in other sections apply to
MMPs. Finally, we remind MMPs of the policy regarding the use of past performance
information for determining plan eligibility to receive passive enrollment.
Annual submission timelines for MMPs are aligned with the standard Medicare Advantage (MA)
and Part D annual schedule, as detailed in this Call Letter. As is the case for other MA and Part
D plans, MMPs must submit a formulary, medication therapy management (MTM) program, and
plan benefit package (PBP).
In addition to the requirements for MA-PD plans and PDPs, MMPs must also submit:
On an annual basis, information to ensure the plan has a network adequate to provide
enrollees with timely and reliable access to providers and pharmacies for Medicare drug
and medical benefits based on requirements in the Medicare Parts C and D programs. In
addition, states will evaluate networks for Medicaid service providers, including long-
term supports and services.
If applicable based on the approval period given to the most recent model of care (MOC)
submission, a MOC that meets CMS’s requirements for SNPs, as well as any applicable
state requirements.
The Additional Demonstration Drug (ADD) file to supplement the Part D formulary
submission.
Table 22 below catalogues previously released guidance for MMPs or guidance that may be of
particular interest to MMPs. CMS will release updated or new guidance as necessary; where
more recent guidance exists or is released for topics that appear in previously released
documents, MMPs should use the most recent document.

224
Table 22: Previously Released Guidance
Topic
Link to document
MMP Enrollment and
Disenrollment Guidance
https://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-
Medicaid-Coordination/Medicare-Medicaid-Coordination-
Office/Downloads/MMPFinalEnrollGuidance.pdf
Additional State-specific
Enrollment Guidance
https://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-
Medicaid-Coordination/Medicare-Medicaid-Coordination-
Office/FinancialAlignmentInitiative/InformationandGuidanceforPlans.html
State-specific Marketing
Guidance
https://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-
Medicaid-Coordination/Medicare-Medicaid-Coordination-
Office/FinancialAlignmentInitiative/InformationandGuidanceforPlans.html
Waiver of Part D LIS Cost-
Sharing Amounts
https://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-
Medicaid-Coordination/Medicare-Medicaid-Coordination-
Office/Downloads/Part_D_Cost_Sharing_Guidance.pdf
Past Performance Review
Methodology Updates for
CY 2017
https://www.cms.gov/Medicare/Prescription-Drug-
Coverage/PrescriptionDrugCovContra/index.html
Network Adequacy Determinations
MMPs will be required to resubmit the Medicare medical provider and facility portion of their
network information in September 2016 to ensure that each MMP continues to maintain a
network of providers that is sufficient in number, variety, and geographic distribution to meet
the needs of the enrollees in its service area. MMPs may assess the Medicare portion of their
networks at any time using the plan-only upload functionality in the HPMS Network
Management Module (NMM). The current reference file that provides the MMP standards is
available at: https://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-
Coordination/Medicare-Medicaid-Coordination-Office/
FinancialAlignmentInitiative/InformationandGuidanceforPlans.html as well as on the reference
page within the NMM. CMS will release additional guidance on the submission process,
including how MMPs will be able to submit exception requests in the summer of 2016. The
Medicare pharmacy portion of the network will be checked per the requirements in the Part D
reporting requirements.
Model of Care (MOC)
As discussed in January 14, 2016 HPMS memorandum, “Changes to Special Needs Plans and
Medicare-Medicaid Plan Model of Care Submissions and Updates in the Health Plan
225
Management System for CY 2017,” we strongly encourage MMPs to avail themselves of the
new off-cycle update process, as MMPs’ MOC submissions preceded the development of three-
way contract requirements on care management and care coordination under each demonstration.
Submission of changes through this process, as outlined in that memorandum and other guidance
from CMS, will allow MMPs to align their current MOCs with all relevant demonstration
requirements.
Formulary and Supplemental Drug Files
Each contract year, MMPs must submit and be approved to offer a demonstration-specific,
integrated formulary that meets both Medicare Part D and Medicaid requirements. For CY 2017
formulary approval, MMPs must submit: (1) an updated base Part D formulary and supplemental
Part D formulary files, as applicable, consistent with CY 2016 Part D formulary application
guidance; and (2) an updated Additional Demonstration Drug (ADD) file containing non-Part D
drugs. MMPs must submit their base formularies no later than June 6, 2016. Supplemental
formulary files are due in HPMS on June 10, 2016 at 11:59 a.m. EDT.
All MMPs must submit an ADD file which can only contain non-Part D drugs. Non-Part D drugs
include drugs in Medicare Part D excluded categories, over-the-counter drugs, and other
products required by the state to be included on the integrated formulary. CMS will work with
states to provide ADD file guidance to MMPs by May 2016. This guidance should include a list
of the drugs the MMPs are required to include on the ADD file (by NDC and/or UPC). It is at
the states’ discretion whether to require their plan applicants to include one proxy NDC or
multiple NDCs on the ADD file for each covered product.
State reviewers are solely responsible for reviewing and approving the ADD file. CMS will
approve all other submitted formulary files. Reviews will begin immediately after the
submission deadlines and will continue until all deficiencies have been resolved.
We clarify that mid-year ADD file change submissions – that is, changes to the ADD file after
the contract year has begun – are at the discretion of each state. CMS will work with states to
open HPMS gates for ad hoc and/or regular ADD file resubmissions as necessary.
CMS released a CY 2017 formulary training video for plans in on March 24, 2016.
We received several comments recommending better coordination of the ADD file and Part D
formulary portions of the formulary review and approval process to avoid access issues related to
prescription drugs that could be covered by either Part D or Medicaid depending on the
circumstances. CMS will work to further streamline the formulary submission and review
process to ensure that such access issues are mitigated.
226
Plan Benefit Package (PBP)
MMPs’ plan benefit packages (PBPs) are reviewed annually to ensure that MMPs accurately
describe the coverage details and cost-sharing for all Medicare, Medicaid, and demonstration-
specific benefits. CMS will launch the HPMS PBP module on April 8, 2016, and we expect to
provide further guidance at that time on MMP-specific updates to the PBP software for CY 2017.
In addition, CMS will release an online training module on the CY 2017 PBP software for plans
on April 8, 2016.
MMPs must submit their integrated PBPs to CMS no later than June 6, 2016 (11:59 p.m. PDT).
Non-timely submission of a PBP is considered a plan notice of non-renewal. In addition, to the
PBP, MMPs are required to submit the following as part of a complete bid submission:
Service Area Verification
Plan Crosswalk (NOTE: This is only for renewing contracts in CY 2017)
Formulary Crosswalk
CMS will work with states to issue PBP guidance that clearly defines the state-required Medicaid
benefits and supplemental demonstration benefits by the time the PBP module is launched in
April 2016. The PBP review will be conducted jointly between CMS and states to ensure the
data entry is consistent with minimum coverage and cost-sharing requirements under Medicaid,
Medicare Parts A, B, and D, and each state’s demonstration.
As part of our demonstration implementation activities, the Medicare-Medicaid Coordination
Office, in partnership with the Center for Medicare, has provided additional flexibility to MMPs
with respect to PBP corrections after the time of final PBP approval. This flexibility has been
necessary to make accommodations, including but not limited to mid-year legislative changes to
Medicaid benefits, as well as the timing of payment rate finalization.
The following policies apply to MMP changes to PBPs:
CMS will consider MMPs’ requests to make PBP revisions to add or remove plan-offered
supplemental benefits between the time of the release of the National Average Monthly
Bid Amount in early August and sign-off of PBPs in HPMS in late August 2016. This
opportunity, if approved, will allow plans to accommodate any benefit changes in their
required documents (including the Annual Notice of Change, Evidence of
Coverage/Member Handbook, and Summary of Benefits) during the Annual Election
Period.
Rate-related PBP corrections to supplemental benefits are permissible during the Center
for Medicare’s annual correction window in September 2016 (see the calendar in this
Call Letter for more information), but only for purposes of adding supplemental benefits
to PBPs. MMPs that elect to correct their PBPs must work with their contract
227
management team on an appropriate member communication strategy (e.g., addenda or
errata sheets for materials that have already been mailed to members; updates to other
materials for current and prospective members). In addition, there will be no compliance
penalty for a PBP correction provided an MMP meets these conditions.
Any PBP corrections after the Center for Medicare’s annual correction window in
September 2016 will be considered on a case-by-case basis. PBP corrections due to plan
error will be subject to compliance action, regardless of whether they are positive or
negative changes.
Past Performance Information and Eligibility for Passive and Opt-in Enrollment
Our policy regarding the use of past performance information is articulated in previous guidance
memoranda, including – most recently – in the February 23, 2015 HPMS memorandum,
“Medicare-Medicaid Plan Annual Requirements and Timeline for CY 2016.” MMPs should refer
to that guidance for additional information regarding the impact of sanctions, treatment of new
legal entities, and eligibility for passive enrollment after effectuation of the three-way contract.

228
Appendix 1 – Contract Year 2017 Guidance for Prescription Drug Plan (PDP) Renewals
and Non-Renewals (Updated)
Prescription Drug Plan (PDP) regions are defined by CMS and consist of one or more entire
states (refer to Appendix 3, Chapter 5, of the Prescription Drug Benefit Manual for a map of the
34 PDP regions). Each PDP sponsor’s Plan Benefit Packages (PBPs) must be offered in at least
one entire region and a PDP sponsor’s PBP cannot be offered in only part of a region. Please
note that PDP bidding rules require PDP sponsors to submit separate bids for each region to be
covered. HPMS only accepts a PDP sponsor’s PBPs to cover one region at a time for individual
market plans (e.g., a PDP sponsor offering a “national” PDP must submit 34 separate PBP bids
in order to cover all PDP regions).
A PDP sponsor may expand the service area of its offerings by submitting additional bids in the
PDP regions the sponsor expects to enter in the following contract year, provided the sponsor
submits a PDP Service Area Expansion (SAE) application and CMS approves that application
and then approves the sponsor’s submitted bids for the new region or regions. For more
information about the application process, refer to: http://www.cms.gov/Medicare/Prescription-
Drug-Coverage/PrescriptionDrugCovContra/RxContracting_ApplicationGuidance.html.
Conversely, a PDP sponsor may reduce its service area by electing not to submit bids for those
regions from which it expects to withdraw. A PDP sponsor must notify CMS in writing (by
sending an email to [email protected]) of its intent to non-renew one or more plans
under a contract by the first Monday in June (June 6, 2016). The same procedure applies to
PDPs converting contracts from offering both individual and employer products to employer-
only products because the individual plan is being non-renewed. However, even absent written
notification to CMS, a PDP sponsor’s failure to submit a timely bid to CMS constitutes a
voluntary non-renewal of the plan by the sponsor. (Note that PDP sponsors reducing their
service areas must provide notice of their action to affected beneficiaries consistent with
regulatory requirements, CMS’ PDP Eligibility, Enrollment, and Disenrollment Guidance,
Chapter 3 of the Prescription Drug Benefit Manual and annual summer CMS non-renewal and
service area reduction guidance.)
Each renewal/non-renewal option available to PDP sponsors for CY 2017 is summarized below
and defined in Appendix 2. These are the same options that existed in CY 2016. All but one of
these actions can be effectuated by PDP sponsors in the HPMS Plan Crosswalk.
Please note, Medicare Advantage Organizations should reference Chapter 4, Chapter 16a, and
Chapter 16b of the Medicare Managed Care Manual for Contract Year 2017 guidance on
renewals and non-renewals.
229
1. New Plan Added
A PDP sponsor may create a new PBP for the following contract year with no link to a PBP it
offers in the current contract year in the HPMS Plan Crosswalk. In this situation, beneficiaries
electing to enroll in the new PBP must complete enrollment requests, and the PDP sponsor
offering the PBP must submit enrollment transactions to MARx. No beneficiary notice is
required in this case beyond receipt of the Evidence of Coverage (EOC), and other documents as
required by current CMS guidance, following enrollment.
2. Renewal Plan
A PDP sponsor may continue to offer a current PBP that retains all of the same service area for
the following year. The renewing plan must retain the same PBP ID number and benefit design
(basic or enhanced alternative) as in the previous contract year in the HPMS Plan Crosswalk.
Current enrollees are not required to make an enrollment election to remain enrolled in the
renewal PBP, and the sponsor will not submit enrollment transactions to MARx for current
enrollees. New enrollees must complete enrollment requests, and the sponsor will submit
enrollment transactions to MARx for those new enrollees. Current enrollees of a renewed PBP
must receive a standard Annual Notice of Change (ANOC) notifying them of any changes to the
renewing plan.
3. Consolidated Renewal Plan
PDP sponsors are permitted to merge two or more entire PBPs offered in the current contract
year into a single renewal plan in the HPMS Plan Crosswalk. A PDP sponsor may not divide a
current PBP among more than one PBP for the following contract year. A PDP sponsor
consolidating two or more entire PBPs must make certain that the consolidated renewal PBP ID
is the same as one of the original consolidating PBP IDs. This is particularly important with
respect to minimizing beneficiary confusion when a plan consolidation affects a large number of
enrollees. When consolidating two existing PBPs into a single renewal PBP, it is permissible for
the single renewal PBP to result in a change from:
A basic benefit design (meaning either defined standard, actuarially equivalent standard,
or basic alternative benefit designs) to another basic benefit design;
An enhanced alternative benefit design to a basic benefit design; or
An enhanced alternative benefit design to another enhanced alternative benefit design.
Current enrollees of a plan or plans being consolidated into a single renewal plan will not be
required to take any enrollment action, and the sponsor will not submit enrollment transactions to
MARx for those current members, although it may need to submit updated 4Rx data to CMS for
the current enrollees affected by the consolidation. New enrollees must complete enrollment
requests, and the sponsor will submit enrollment transactions to MARx for those new enrollees.

230
Current enrollees of a consolidated renewal plan must receive a standard ANOC.
CMS will no longer approve bids that include a PBP that would change a basic plan to an EA
plan because of the potential for beneficiary confusion and disruption, as noted above, absent a
compelling reason in CMS’s determination, such as a sponsor that is under a consolidation plan.
4. Renewal Plan with a Service Area Expansion (“800 Series” EGWPs only)
A PDP sponsor offering an 800 series EGWP PBP in the current contract year may expand its
EGWP service area to include additional PDP regions for the following contract year through the
Part D application process. In order for currently enrolled beneficiaries to remain in the renewed
PBP, the sponsor must retain the same PBP ID number for the following contract year.
Current enrollees will not be required to take any enrollment action, and the sponsor will not
submit enrollment transactions to MARx for those current enrollees. New enrollees must
complete enrollment requests, and the sponsor will submit enrollment transactions to MARx for
those new enrollees. Current enrollees of a renewed PBP with a SAE must receive a standard
ANOC notifying them of any changes to the renewing plan.
5. Terminated Plan (Non-Renewal)
A PDP sponsor may elect to terminate a current PBP for the following contract year and must
notify CMS in writing (by sending an email to [email protected]) by June 6, 2016.
CMS expects the sponsor to crosswalk the affected enrollees into the most comparable plan,
which includes the sponsor’s basic plan if that is the only plan available. However, as stated in
the CY 2015 Call Letter, CMS reminds sponsors that we do not intend to approve bids under
which a PDP sponsor would propose to non-renew its current basic plan in a PDP region, thus
disenrolling all the plan’s current members at the end of the year, and offer a brand new basic
plan during the upcoming benefit year. In a situation where enrollees are crosswalked to a
comparable plan, the sponsor will not submit disenrollment transactions to MARx for affected
enrollees. When a sponsor terminates a PBP, plan enrollees must make a new election for their
Medicare coverage in the following contract year. To the extent that a current enrollee of a
terminated PBP elects to enroll in another plan offered by the current or another PDP sponsor –
or, alternatively, elects to enroll in an MA plan – he/she must complete an enrollment request,
and the enrolling organization or sponsor must submit enrollment transactions to MARx so that
those individuals are enrolled. Enrollees of terminated PBPs will be sent a model termination
notice that includes notification of a special election period, as well as information about
alternative options.
6. Consolidated Plans under a Parent Organization
For purposes of ensuring compliance with transition requirements following an acquisition or
merger under our significant differences policy, or to make plan transitions following a novation,
231
CMS may elect to allow the merger of two or more entire PBPs offered under different contracts
(the contracts may be offered by the same legal entity or represent different legal entities). PDP
sponsors must complete this renewal option by submitting a crosswalk exception request through
HPMS. CMS will provide detailed technical instructions for completing a crosswalk exception
request through HPMS in forthcoming guidance. Requests will be reviewed and, if approved,
the action will be completed on behalf of the requesting PDP. Current enrollees of a plan or plans
being merged across contracts in this manner will not be required to take any enrollment action,
and the sponsor will not submit enrollment transactions to MARx for those current members,
although it may need to submit updated 4Rx data to CMS for the current enrollees affected by
the consolidation. New enrollees must complete enrollment requests, and the sponsor will
submit enrollment transactions to MARx for those new enrollees. Current enrollees of a
consolidated renewal plan must receive a special notice along with a standard ANOC.

232
Appendix 2 – Contract Year 2017 Guidance for Prescription Drug Plan (PDP) Renewals and Non-Renewals Table
Activity
Definitions
HPMS Plan Crosswalk
Systems Enrollment
Activities
Enrollment
Procedures
Beneficiary
Notifications
1
New Plan
(PBP) Added
A PDP sponsor
creates a new PBP.
HPMS Plan Crosswalk
Definition:
A new plan added for 2017
that is not linked to a 2016
plan.
HPMS Plan Crosswalk
Designation: New Plan
The PDP sponsor must
submit enrollment
transactions.
New enrollees must
complete an
enrollment request.
None.
2
Renewal Plan
A PDP sponsor
continues to offer a
CY 2016 PBP in CY
2017. The same PBP
ID number and
benefit design (basic
or enhanced
alternative) must be
retained in order for
all current enrollees
to remain in the same
PBP in CY 2016.
HPMS Plan Crosswalk
Definition:
A 2017 plan that links to a
2016 plan and retains all of
its plan service area from
2016. The 2017 plan must
retain the same plan ID as
the 2016 plan.
HPMS Plan Crosswalk
Designation:
Renewal Plan
The renewal PBP ID must
remain the same so that
current enrollees will
remain in the same PBP ID.
The PDP sponsor does not
submit enrollment
transactions for current
enrollees.
No enrollment
request for current
enrollees to remain
enrolled in the
renewal PBP in
2017. New
enrollees must
complete
enrollment request.
Current
enrollees are
sent a
standard
ANOC.
233
Activity
Definitions
HPMS Plan Crosswalk
Systems Enrollment
Activities
Enrollment
Procedures
Beneficiary
Notifications
3
Consolidated
Renewal Plan
A PDP sponsor
combines two or
more PBPs offered in
CY 2016 into a single
renewal PBP for CY
2017. The PDP
sponsor must
designate which of
the renewal PBP IDs
will be retained in
CY 2016 after
consolidation.
HPMS Plan Crosswalk
Definition:
Two or more 2016 plans
that merge into one 2017
plan. The 2017 plan ID
must be the same as one of
the consolidating 2016
plan IDs.
HPMS Plan Crosswalk
Designation: Consolidated
Renewal Plan
The PDP sponsor’s
designated renewal PBP ID
must remain the same so
that CMS can consolidate
current enrollees into the
designated renewal PBP ID.
The PDP sponsor does not
submit enrollment
transactions for current
enrollees. Sponsors may
need to submit updated 4RX
data for enrollees affected
by the consolidation.
No enrollment
request for current
enrollees to remain
enrolled in the
renewal PBP in
2017.
Current
enrollees are
sent a
standard
ANOC.

234
Activity
Definitions
HPMS Plan Crosswalk
Systems Enrollment
Activities
Enrollment
Procedures
Beneficiary
Notifications
4
Renewal Plan
with an SAE
(applicable
only to
employer/
union group
waiver plans)
A PDP sponsor
continues to offer an
800 series CY 2016
prescription drug
PBP in CY 2017 and
expands its EGWP
service area to
include additional
regions. The PDP
sponsor must retain
the same PBP ID
number in order for
all current enrollees
to remain in the same
PBP in CY 2017.
HPMS Plan Crosswalk
Definition:
A 2017 800-series plan
that links to a 2016 800-
series plan and retains all
of its plan service area
from 2016, but also adds
one or more new regions.
The 2017 plan must retain
the same plan ID as the
2016 plan.
HPMS Plan Crosswalk
Designation:
Renewal Plan with an SAE
The renewal PBP ID must
remain the same so that
current enrollees in the
current service area will
remain in the same PBP ID.
The PDP sponsor does not
submit enrollment
transaction for current
enrollees.
No enrollment
request for current
enrollees to remain
enrolled in the
renewal PBP in
2017. New
enrollees must
complete
enrollment request.
Current
enrollees are
sent a
standard
ANOC.
235
Activity
Definitions
HPMS Plan Crosswalk
Systems Enrollment
Activities
Enrollment
Procedures
Beneficiary
Notifications
5
Terminated
Plan (Non-
Renewal)
A PDP sponsor
terminated the
offering of a 2016
PBP.
HPMS Plan Crosswalk
Definition:
A 2016 plan that is no longer
offered in 2017. HPMS Plan
Crosswalk Designation:
Terminated Plan
CMS expects the sponsor
to crosswalk the affected
enrollees into the most
comparable plan. The
PDP sponsor does not
submit disenrollment
transactions.
If the terminated enrollee
elects to enroll in another
PBP with the same or
another PDP sponsor or
MAO, the enrolling PDP
sponsor or organization
must submit enrollment
transactions to enroll the
terminated enrollees.
Terminated
enrollees must
complete an
enrollment request
if they choose to
enroll in another
PBP, even a PBP
offered by the same
PDP sponsor.
Terminated
enrollees are
sent a CMS
model
termination
notice
including
SEP
information
and receive a
written
description
of options for
obtaining
prescription
drug
coverage in
the service
area.

236
Activity
Definitions
HPMS Plan Crosswalk
Systems Enrollment
Activities
Enrollment
Procedures
Beneficiary
Notifications
6
Consolidated
Plans across
Contracts
under the
Same Parent
Organization
A parent organization
merges two or more
whole PBPs under
different contracts
(the contracts may be
the same legal entity
or represent different
legal entities) as a
result of a merger,
acquisition, or
novation. A PDP
sponsor cannot
complete this renewal
option in the HPMS
Plan Crosswalk.
Exceptions Crosswalk
Request: Sponsors must
submit an exceptions
request to CMS, which
will complete the
crosswalk on behalf of the
sponsor
HPMS Plan Crosswalk
Designation:
The plan being crosswalk-
ed must be marked as a
terminated plan in the
HPMS crosswalk.
The remaining 2017 plan
must be active and contain
the applicable service area
from the terminated plan
being crosswalked.
PDP sponsors cannot
complete this renewal
option in the HPMS Plan
Crosswalk. CMS will
effectuate this renewal
option and HPMS will
record the merger of two
or more whole PBPs. The
PDP sponsor does not
submit enrollment
transactions for current
enrollees. Sponsors may
need to submit updated
4RX data for enrollees
affected by the
consolidation.
No enrollment
election for current
enrollees to remain
enrolled in the
renewal PBP in
2017. New
enrollees must
complete
enrollment request.
Current
enrollees are
sent a
standard
ANOC.

237
Appendix 3 – Improvement Measures (Part C & D)
Part
C or D
Measure
Measure Type
Weight
Improvement
Measure
C
Breast Cancer Screening
Process Measure
1
Yes
C
Colorectal Cancer Screening
Process Measure
1
Yes
C
Annual Flu Vaccine
Process Measure
1
Yes
C
Improving or Maintaining Physical
Health
Outcome Measure
3
No
C
Improving or Maintaining Mental
Health
Outcome Measure
3
No
C
Monitoring Physical Activity
Process Measure
1
Yes
C
Adult BMI Assessment
Process Measure
1
Yes
C
Special Needs Plan (SNP) Care
Management
Process Measure
1
Yes
C
Care for Older Adults – Medication
Review
Process Measure
1
Yes
C
Care for Older Adults – Functional
Status Assessment
Process Measure
1
Yes
C
Care for Older Adults – Pain
Assessment
Process Measure
1
Yes
C
Osteoporosis Management in
Women who had a Fracture
Process Measure
1
Yes
C
Diabetes Care – Eye Exam
Process Measure
1
Yes
C
Diabetes Care – Kidney Disease
Monitoring
Process Measure
1
Yes
238
Part
C or D
Measure
Measure Type
Weight
Improvement
Measure
C
Diabetes Care – Blood Sugar
Controlled
Intermediate Outcome Measure
3
Yes
C
Controlling Blood Pressure
Intermediate Outcome Measure
3
Yes
C
Rheumatoid Arthritis Management
Process Measure
1
Yes
C
Reducing the Risk of Falling
Process Measure
1
Yes
C
Plan All-Cause Readmissions
Outcome Measure
3
Yes
C
Getting Needed Care
Patients’ Experience and Complaints Measure
1.5
Yes
C
Getting Appointments and Care
Quickly
Patients’ Experience and Complaints Measure
1.5
Yes
C
Customer Service
Patients’ Experience and Complaints Measure
1.5
Yes
C
Rating of Health Care Quality
Patients’ Experience and Complaints Measure
1.5
Yes
C
Rating of Health Plan
Patients’ Experience and Complaints Measure
1.5
Yes
C
Care Coordination
Patients’ Experience and Complaints Measure
1.5
Yes
C
Complaints about the Health Plan
Patients’ Experience and Complaints Measure
1.5
Yes
C
Members Choosing to Leave the
Plan
Patients’ Experience and Complaints Measure
1.5
Yes
C
Beneficiary Access and
Performance Problems
Measures Capturing Access
1.5
No
C
Health Plan Quality Improvement
Improvement Measure
5
No
C
Plan Makes Timely Decisions
about Appeals
Measures Capturing Access
1.5
Yes
C
Reviewing Appeals Decisions
Measures Capturing Access
1.5
Yes
C
Call Center – Foreign Language
Interpreter and TTY Availability
Measures Capturing Access
1.5
Yes

239
Part
C or D
Measure
Measure Type
Weight
Improvement
Measure
D
Call Center – Foreign Language
Interpreter and TTY Availability
Measures Capturing Access
1.5
Yes
D
Appeals Auto–Forward
Measures Capturing Access
1.5
Yes
D
Appeals Upheld
Measures Capturing Access
1.5
Yes
D
Complaints about the Drug Plan
Patients’ Experience and Complaints Measure
1.5
Yes
D
Members Choosing to Leave the
Plan
Patients’ Experience and Complaints Measure
1.5
Yes
D
Beneficiary Access and
Performance Problems
Measures Capturing Access
1.5
No
D
Drug Plan Quality Improvement
Improvement Measure
5
No
D
Rating of Drug Plan
Patients’ Experience and Complaints Measure
1.5
Yes
D
Getting Needed Prescription Drugs
Patients’ Experience and Complaints Measure
1.5
Yes
D
MPF Price Accuracy
Process Measure
1
No
D
High Risk Medication
Intermediate Outcome Measure
3
Yes
D
Medication Adherence for Diabetes
Medications
Intermediate Outcome Measure
3
Yes
D
Medication Adherence for
Hypertension (RAS antagonists)
Intermediate Outcome Measure
3
Yes
D
Medication Adherence for
Cholesterol (Statins)
Intermediate Outcome Measure
3
Yes
D
MTM Program Completion Rate
for CMR
Process Measure
1
Yes

240
Appendix 4 - 2017 Draft Call Letter Star Ratings Summary of Comments and Responses
Call Letter Section
Summary of Comments
CMS Final Course of Action
Improvement Measures (C & D)
A few comments were received from sponsors with specific suggestions
for methodology changes to the Improvement Measures, including:
Calculate Star Ratings separately for Part C and Part D with and
without the Improvement Measures, or allow for inclusion of the Part
C or D Improvement Measures.
Evaluate performance on a log scale instead of a linear scale.
Adjust the threshold for what is considered an improvement relative
to the plan’s level of performance.
Weight improvement achieved relative to current performance.
A small number of comments were received about specific measures in
the Improvement Measures (such as CAHPS, HRM, MTM, and Call
Center).
Proceed as proposed. CMS wants to
incentivize improvement for all
contracts while addressing the
challenges faced by contracts at
different levels of performance. We
continue to evaluate potential
enhancements to the improvement
methodology.
Appeals Timeliness/Reviewing
Appeals Decisions measures (Part
C) and Appeals Upheld (Part D)
All comments supported the change to allow reopenings completed by
May 1 to be incorporated into these two measures.
Proceed as proposed.
Contract Enrollment Data (Part C &
D)
The majority of commenters agreed that CMS should keep the current
enrollment methodology.
Proceed as proposed and make no
changes.
Transition from ICD-9 to ICD-10
(Part C & D)
There were only a few comments acknowledging the transition with one
suggesting CMS monitor the impact on Star Ratings measures.
Proceed as proposed as the ICD-10
codes have been implemented.
Appeals Upheld measure (Part D)
All comments supported no longer excluding cases for beneficiaries
enrolled in hospice.
Proceed as proposed.

241
Call Letter Section
Summary of Comments
CMS Final Course of Action
Medication Therapy Management
(MTM) Program Completion Rate
for Comprehensive Medication
Reviews (CMS) measure (Part D)
Most comments were submitted by sponsors, and were supportive of the
additional data to be provided during plan preview periods. Some
proposed specification changes, or additional MTM performance
measures.
Proceed as proposed. CMS shared
additional comments received with
the PQA.
Medication Adherence for
Hypertension (RAS Antagonists)
(Part D Star Ratings)
A small number of comments were received, but all supported the
specification change to exclude patients with one or more claims for
sacubitril/valsartan from the measure. Other commenters suggested
additional revisions to the measure specifications, which will be shared
with the PQA.
Proceed as proposed.
Removal of Measures from Star Ratings
Improving Bladder Control (Part C)
A small number of plans, associations and advocates commented on the
plans for this measure. All supported the move of the measure to the
display page, but a number requested the measure not return to Star
Ratings any time soon, in part from doubts about data from patient
surveys, but especially to give plans adequate time to respond when the
measure is returned to Star Ratings. One association argued that
treatment receipt should be retained as a focus, rather than shifting it
entirely to the discussion of treatment.
No change, except to state in the CY
2017 final Call Letter plan to leave
measure on display page for 2018 as
well as for 2017. Follow NCQA’s
lead as the HEDIS measure steward,
paying attention to how much notice
plans have.
High Risk Medication (Part D)
Support among sponsors, associations, PBMs, and other organizations
was split between moving the High Risk Medication (HRM) measure to
the display page for 2017 and keeping the measure in the Star Ratings.
Most commenters that opposed the change requested that the measure
remain in the Star Ratings for 2017 since this change was being made
after the measurement period in which efforts were invested. Other
commenters provided feedback including specification revisions which
will be shared with the measure developer, PQA.
Keep the HRM measure in the Star
Ratings for 2017 due to the
measurement period concerns raised
and move it to the display measures
for 2018. The measure will be
reconsidered for the Star Ratings
again in the future once analyses
and specification changes, if any,
are completed by the PQA.
Data Integrity

242
Call Letter Section
Summary of Comments
CMS Final Course of Action
Data Integrity
Commenters included sponsors, advocacy groups and trade
organizations, and all support that CMS Star Ratings only use accurate
data. Some sponsors requested the opportunity to correct erroneous data,
or that CMS only reduce scores when errors were intentionally made.
Others requested CMS provide detailed methodologies for data integrity
checks, or establish allowed thresholds for data errors.
Proceed as proposed. The Call
Letter provides examples of non-
compliance that would directly bias
measure-level data. We will add
links for more information about
these areas, for example CMS Data
Validation Standards and HEDIS
Technical Specifications.

243
Call Letter Section
Summary of Comments
CMS Final Course of Action
Impact of Socio-economic and Disability Status on Star Ratings
Interim Analytical Adjustments
The majority of the comments received for the draft Call Letter provided
feedback on the dual/LIS Star Ratings section of the draft Call Letter.
Almost all commenters supported moving forward with Categorical
Adjustment Index (CAI) as an interim solution. A few commenters
wanted to wait, but supported CAI if the Agency were to move forward
with an interim solution. Some commenters wanted additional measures
to be adjusted for an LIS/DE and/or disability effect, with a couple of
commenters not supporting CAI unless additional measures were added.
However, commenters did not suggest specific measures. Some
commenters wanted CMS not to move forward with an interim solution;
many of these commenters represented beneficiary advocacy groups and
were concerned about masking true disparities of care. Other
commenters who preferred to wait did not want a complex interim
solution implemented prior to ASPE and measure developers completing
their work. Some commenters, representing plans, requested a hold
harmless provision such that the CAI values would only be applied if it
resulted in a positive adjustment. A handful of commenters expressed
support for CMS efforts in this area, but did not express a preference on
the proposed approach. No comments were received that supported
Indirect Standardization (IS). There were some questions about the
duration of the interim fix and the process to update CAI values.
Proceed with the CAI as an interim
analytical adjustment for the 2017
Star Ratings Program and provide
additional clarifications in the CY
2017 final Call Letter to address
commenters’ questions. In the final
Call Letter we will reiterate that the
duration of the interim adjustment
will be dependent on the ASPE and
measure developers’ work coupled
with our work to simulate any
recommendations. We will also
provide additional information about
CMS’ commitment to update the
CAI values (measures and
differences in performance) on an
annual basis.
244
Call Letter Section
Summary of Comments
CMS Final Course of Action
Puerto Rico
The vast majority of the submissions expressed support for the estimated
LIS indicator and for the reduction in the weights for the three Part D
adherence measures. One of the commenters suggested modifications to
the methodology to estimate the LIS indicator, while another submitter
suggested using Census data. There was a single commenter that did not
support moving forward with the reduction in the adherence weights.
Proceed with using the LIS indicator
for PR in the interim analytical
adjustment and reducing the weights
of the three Part D adherence
measures in PR. We will add
additional language to the final Call
Letter that we hope to continue
discussions with PR stakeholders
about alternative data sources and
methodological enhancements for
2018 stars and beyond.
2017 CMS Display Measures
Timely Receipt of Case Files for
Appeals (Part D) & Timely
Effectuation of Appeals (Part D)
All commenters supported the change to match the measurement periods
of the Part D Appeals Star Ratings measures.
Proceed as proposed.
Medication Reconciliation Post
Discharge (Part C)
While some of the commenters supported the measure, others
recommended for the measure to remain on the display page until 2018
or 2019 for monitoring. Some had methodology or validity concerns and
they requested more time to address accurate data collection,
appropriateness of the population for the measure, and application to
Part D.
Proceed as proposed as this measure
has been collected by SNPs for
many years. CMS is planning to
include this measure on the 2017
display page and in the 2018 Star
Ratings to expand the focus on care
coordination.

245
Call Letter Section
Summary of Comments
CMS Final Course of Action
Hospitalizations for Potentially
Preventable Complications (Part C)
The majority of the comments requested the measure remain on the
display page longer and a few others had validity or methodology
concerns. Commenters recommended further testing and refinement for
the measure.
Proceed as proposed. CMS is
planning to include this measure on
the 2017 display page and in the
2018 Star Ratings to expand the
focus on care coordination. If there
are issues during the first year of
data collection and reporting, CMS
will re-consider this decision.
Statin Therapy for Patients with
Cardiovascular Disease (Part C)
The majority of the comments supported the measure and continuance of
it as a display measure through 2018. Others recommended continued
validation of the measure. Some provided recommendations, including
excluding those taking PCSK-9 inhibitors, patients with counter
indications, those unable to tolerate medication, and ESRD patients.
CMS plans to include this measure
on the 2017 and 2018 display pages
and consider it for inclusion in Star
Ratings in future years.
Asthma Measures (Part C)
The majority of comments were against the two measures. Commenters
expressed opinions that expanding the asthma measure to the age 65 and
older population was inappropriate due to the difficulty of distinguishing
asthma from COPD in this population; that asthma should not be
identified by medication but by diagnosis; and that the asthma
medication ratio measure is contrary to NIH recommendations. Support
for the measures was received from pharmaceutical companies.
CMS plans to include these two
measures on the 2017 and 2018
display pages and consider them for
potential inclusion in Star Ratings in
future years.
Statin Use in Persons with Diabetes
(SUPD) (Part D)
Substantially all of the comments received from sponsors and
organizations supported adding the SUPD measure to the 2017 display
page, where it will remain for two years before adding to the Star
Ratings. One sponsor commenter opposed. A few commenters
requested that the PQA revisit its decision not to exclude beneficiaries
who use PCSK-9 inhibitors from the measure calculation.
Proceed as proposed. We shared
comments regarding measure
specifications with the PQA.

246
Call Letter Section
Summary of Comments
CMS Final Course of Action
Forecasting to 2018 and Beyond
New Measures:
Care Coordination Measures
(Part C)
Commenters were largely supportive of this work, but cautioned CMS to
consider burden on sponsors, coordinate with Medicaid, and consider
contributions of non-physician providers. They also requested that CMS
clarify the intent of this work as well as provide a working definition of
care coordination.
Proceed as proposed to develop care
coordination measures, taking into
account commenter concerns. CMS
will provide more information about
this work as it is available.
Depression Measures (Part C)
Commenters requested that CMS delay implementation of these
measures due to concerns about data and privacy issues, as well as the
use of other screening tools. Several suggested that CMS first
implement a depression screening measure before including a depression
outcome measure.
Proceed as proposed to monitor
development of these measures.
CMS shared additional comments
received with NCQA.
Appropriate Pain Management
(Part C)
Commenters were supportive of the development of appropriate pain
management measures but mentioned the need to develop screening
protocols for pain. Commenters requested to be kept informed of
measure development and to be provided detailed measure specifications
prior to inclusion in Star Ratings.
Proceed as proposed. CMS shared
comments received with NCQA.
Use of Opioids from Multiple
Providers or at High Dosage in
Persons without Cancer (Part D)
Most commenters supported adding new opioid overutilization measure
reports through the Patient Safety Analysis Website, and adding the
measures to the 2019 display page, and a few expressly supported not
moving to the Star Ratings (at least until consensus guidelines). A small
number of commenters opposed adding the new measures to the display
page or additional reporting outside of the OMS.
Proceed as proposed.

247
Call Letter Section
Summary of Comments
CMS Final Course of Action
Antipsychotic Use in Persons with
Dementia (APD) (Part D)
Most commenters supported adding new APD reports through the
Patient Safety Analysis Website, and adding the measures to the 2018
display page. A few commenters did not support adding the new
measure, or expressly supported not moving the measure to the Star
Ratings (or at least until certain conditions are met). Some commenters
recommended additional specification changes which will be shared with
the PQA.
Proceed as proposed.
Changes to Existing Star Ratings and Display Measures and Potential Future Changes:
Colorectal Cancer Screening (Part
C Star Ratings
Commenters requested to be kept informed of measure development and
to be provided detailed measure specifications prior to inclusion in Star
Ratings.
Proceed as proposed. CMS shared
comments received with NCQA.
Fall Risk Management (Part C Star
Ratings)
A small number of plans, associations, and advocates commented, and
almost all supported the changes proposed by CMS. There was some
distrust of the measure or its source being a patient survey, some concern
that Vitamin D should not be used as an example of a Fall Risk
Management intervention, and a wish that audiologists could have a
greater role in measures related to vestibular disorders. Some concerns
were raised about whether or not this measure should be included in the
subset of measures adjusted for SES/disability factors, especially that
adjustments could disincentivize plans from developing programs to
serve dual populations. However, most comments were supportive and
only asked that plans be given sufficient notice when the measure is
moved back into Star Ratings.
Proceed as proposed by following
NCQA’s lead as the HEDIS
measure steward. CMS will
monitor the potential unintended
consequences of adjusting for
SES/disability.
Pneumococcal Vaccination Status
for Older Adults (Part C Display)
Half the organizations demonstrated concern with recall bias and using
CAHPS for tracking clinical measures. Recommendations include
basing the measure on claims or keeping the measure as display.
Proceed as proposed.

248
Call Letter Section
Summary of Comments
CMS Final Course of Action
CAHPS Measures (Part C & D)
Commenters support the CAHPS 5.0 changes, and very few commented
on the sampling proposal. Several expressed general concerns about
CAHPS or requests for clarification, including the length of the survey,
sample size, use of proxy respondents, language translations, availability
of case-mix information, and duplication with Medicaid.
Proceed as proposed and provide
additional information about
CAHPS in the final Call Letter.
CMS will remove some CAHPS
questions not used in Star Ratings in
order to reduce the length of the
2017 MA CAHPS survey.
MPF Price Accuracy (Part D Star
Rating)
Commenters expressed concern with the timing and frequency of point-
of-sale (POS) price changes (PDE) versus the MPF price changes. This
is a standard comment that does not change the CMS approach as we
would not expect this limitation to keep plans from lowering their prices
at the POS. Other commenters discussed MA-PD cut-points and
performance.
Proceed as proposed.
Drug-Drug Interactions (DDI)
(Part D Display)
One commenter expressed support for the evaluation of the DDI
measure, while others provided technical suggestions.
Proceed as proposed.
Center for Medicare and Medicaid
Innovation Model Tests
Commenters support excluding participating plans from cut-points or
establishing separate cut-points for model participants in order to ensure
a level playing field. They also requested more details about CMS’ Star
Ratings approach for model participants.
The model tests will not be
implemented until 2017, so they will
not affect ratings until 2019 Star
Ratings. CMS will provide
additional details about our
approach for model participants’
Star Ratings in a future Call Letter.

249
Call Letter Section
Summary of Comments
CMS Final Course of Action
Measurement and Methodological Enhancements
Ad hoc Comments
Sanctions: In response to the draft CY 2017 Call Letter, we received
multiple comments suggesting that CMS revise its policy of
automatically reducing the Star Ratings of sanctioned contracts to 2.5
stars, or reducing by one star the ratings of those contracts already rated
at 2.5 stars or lower. Commenters raised several concerns, including one
noting that high-rated contracts can be subjected to a more severe
penalty than low-rated contracts as their rating can be reduced by
multiple stars to reach 2.5 stars, while low-rated contracts face a rating
reduction of only one star. Commenters stated that CMS should re-
evaluate the current policy given these concerns and the state of the Part
C and D Star Rating program today.
Assorted Comments: Comments ranged in topics from general to
measure-specific. They included questions and comments related to the
process, ideas for changes for other Star Rating or display measures, cut-
points, and the development of outcome measures.
As announced in the March 8, 2016
HPMS memo, CMS is suspending
the sanction deduction, while it re-
evaluates the impact of sanctions,
audits and CMPs on the Star
Ratings. CMS plans to include any
potential changes in the Request for
Comments in Fall 2016.
We are reviewing all comments as
we consider future enhancements to
the Star Ratings.

250
Appendix 5 – Adjusted Measure Selection Criteria
Variation Across MA and PDP Contracts of Within-Contract LIS/DE Differences
MA Measure
Minimum
Median
Maximum
Adult BMI Assessment
−0.133
0.009
0.231
Rheumatoid Arthritis Management
−0.098
−0.034
−0.008
Breast Cancer Screening
−0.236
−0.085
0.053
Controlling High Blood Pressure
−0.028
−0.005
0.028
Diabetes Care: Blood Sugar Controlled
−0.119
−0.064
0.006
Diabetes Care: Eye Exam Performed
−0.153
−0.045
0.125
Diabetes Care: Kidney Disease Monitoring
−0.057
−0.006
0.033
Colorectal Cancer Screening
−0.179
−0.061
0.095
Osteoporosis Management in Women Who had a Fracture
−0.077
−0.056
−0.029
No All-Cause Readmission
27
−0.036
−0.015
−0.003
Annual Flu Vaccine
−0.070
−0.035
0.020
Monitoring Physical Activity
−0.092
−0.006
0.099
Reducing the Risk of Falling
0.108
0.131
0.155
Medication Adherence for Diabetes
−0.066
−0.006
0.081
Medication Adherence for Hypertension
−0.081
−0.023
0.102
Medication Adherence for Cholesterol
−0.095
−0.002
0.112
PDP Measure
Medication Adherence for Diabetes
−0.106
−0.038
0.018
Medication Adherence for Hypertension
−0.139
−0.062
−0.018
Medication Adherence for Cholesterol
−0.103
−0.034
0.021
For PDPs, the research showed that the median absolute difference in performance between
LIS/DE and non-LIS/DE enrollees was greater than 5% for Medication Adherence for
Hypertension. It was slightly smaller for MA-PDs, but to apply consistent adjustments across
MA-PDs and PDPs it is included for both delivery systems.
The measures selected for adjustment included the following six Part C measures for MA (MA-
only, MA-PD) and 1876 contracts: Breast Cancer Screening, Colorectal Cancer Screening,
Diabetes Care – Blood Sugar Controlled, Osteoporosis Management in Women who had a
Fracture, Rheumatoid Arthritis Management, and Reducing the Risk of Falling. In addition,
Medication Adherence for Hypertension (RAS antagonists) was adjusted for MA-PDs and PDPs.
27
Readmissions was reverse coded in the analysis. Readmissions is excluded from the subset of measures for adjustment, since
the measure is already adjusted for factors associated with disability status. In addition, CMS is reviewing the measure.
