
1
EHP-PR1(4/24)
ARKANSAS DEPARTMENT OF HEALTH
RETAIL FOOD PLAN REVIEW SUBMISSION FORMS
GENERAL ESTABLISHMENT INFORMATION
Construction Type (please check one):
____ NEW ____ REMODEL ____ COMMERCIAL/INCUBATOR/CONTRACT OPERATOR KITCHEN
____ NEW OWNER EXISTING ESTABLISHMENT _____MOBILE /PUSHCART _____ CONVERSION
____PARTIAL REMODEL (FIRE/FLOOD) ____ RESUBMIT (Previous Submission Date) __________
Projected Start Date: _______________ Projected Date for Completion: ___________________
Name of Establishment / Project: __________________________________________________
Physical Address: ____________________ City: _______________ State: ________Zip: _______
County: _______________________ Phone Number: __________________________________
OWNER INFORMATION
Name of Owner: ________________________________________________________________
Owner’s Mailing / Billing Address: ______________________________ City: _______________
State: ________ Zip: _________ Contact Phone Number: _______________________________
Owner’s Email Address: _______________________ Gov. ID #: __________________ State: ___
TYPE OF ESTABLISHMENT (Please Check Only One Category)
____ Restaurant _____ Food Store _____ Kiosk ____Private School ____ Public / Charter School
_____ Private Food Service Contractor for Public Schools _____ Daycare / Childcare
_____ Food Mobile/Truck ______ Hotdog Cart / Pushcart ______ Food Salvage
_____ Summer Feeding/Afterschool _____ Food Pantry / Food Storage

2
EHP-PR1(4/24)
RETAIL PLAN REVIEW SUBMISSION DOCUMENTATION:
The items below have been included with the plans being submitted at this time. It is understood that
omission of any requested information will result in a delay in the plan approval. Once all required items
are received and any required fee paid, the plans will be reviewed within the time allotted by the
Arkansas Department of Health.
YES
NO
REQUIRED SUBMITTED INFORMATION
Proposed Menu
Completed set of plans drawn to scale or with drawing legend
List or Set of Manufacturer equipment specifications or list of equipment
Standard Operating Procedures
Plumbing plans showing hot and cold-water supply, sink locations, floor drains,
waste lines from fixtures, water heaters
Warewashing facilities and food prep sinks
Hand sinks and toilet facilities with soap and towel provisions
Restrooms / toilet facilities
Storage rooms / area for food storage
Service sink / cleaning facilities area
Chemical storage area
Employee storage area / changing room
*HACCP Plan and supporting documentation (if required for specialized process)
*Variance Request Form and Documentation (if required for specialized process)
Equipment plan and schedule showing location of equipment
SOURCE OF WATER: _____ Municipal ______ Well ______ Other: ________
SOURCE OF WASTEWATER: ______ Municipal Sewage _____ Septic System
ADDITIONAL REQUIREMENTS FOR FOOD TRUCKS – PUSH CARTS:
Size and location of Fresh Water Tank and material to construct
Size and location of Gray Water Tank and material to construct
Service Area Agreement and Commissary Prep location
*SPECIALIZED PROCESS: Check All That Applies
_____ Curing ____ Acidification (sushi, etc.) ____ Smoking _____ Live Molluscan Shellfish
____Reduced Oxygen Packaging ROP (eg: Vacuum packaging, sous vide, cook-chill etc.)
____ Custom Processing ____ Sprouting ____ Other, please describe and explain:

3
EHP-PR1(4/24)
OPERATION INFORMATION
HIGHLY SUSCEPTIBLE POPULATION: Will this facility cater to or serve any of the following:
(Check all that applies)
____ Assisted Living ____ Childcare ____ Health Care /Immunocompromised
______ Nursing Home _____ School with pre-school aged children
HOURS OF OPERATION
_____ This is a Mobile Unit/Food Truck, and my hours vary.
Day Of Week
Open Time
Closed Time
Sunday
Monday
Tuesday
Wednesday
Thursday
Friday
Saturday
Estimated Meals (provide number)
Buffet Service
Breakfast
Lunch
Dinner
Other
(snacks meals)
Total
anticipated daily
TYPE OF SERVICE (CHECK ALL THAT APPLY):
____ Sit Down Meals ____ Take Out/Delivery ____ Catering ____ Buffet/Self-Service
____ Outdoor Service Area ____ Full-Service Bar ____ Other
Number of Indoor Dining Seats: _____________
Number of Outdoor Dining Seats: ____________
Number of Staff (Maximum per shift): ____________
Total Square Footage of Facility: ____________
4
EHP-PR1(4/24)
STORAGE FOR OPERATION
COLD STORAGE
Anticipated frequency of frozen food delivery: ___________________ (example every Thursday)
Anticipated frequency of refrigerated food delivery: ________________
Provide information on the amount of space allocated:
Refrigerated Storage:
Frozen Storage:
DRY STORAGE
Anticipated frequency of dry storage and paper goods: ____________________
Identify the location and containers that will be used to store bulk food products like rice, flour,
sugar, etc.
Provide Information on the amount of space allocated for Dry Storage…
HOT AND COLD HOLDING
HOT HOLDING: List all foods that will be hot held prior to service:
COLD HOLDING: List all foods that will be held cold prior to service:

5
EHP-PR1(4/24)
Appe�zers
Desserts
Soup & Salads
Main / Meats
Sides
Drinks
MENU
Please include menu items being served. While a copy of your actual menu is preferred the following is a
template to assist you in this process if you do not have an official menu. Include additional pages if necessary.

6
EHP-PR1(4/24)
Standard Operating Procedures for Food Service Establishments
Who must have standard operating procedures?
• All new food establishments, including but not limited to Mobile/Pushcarts, Feeding Programs,
Cooking or Prep Kitchens, Concession Stands, Temporary Establishments and Food Trucks.
• Remodeled food establishments that change menu or operation must update and resubmit.
• Establishments using a HACCP Plan or Variance.
What are standard operating procedures?
• Procedures specific to your operation describing the activities necessary to complete
tasks in accordance with the food code and Arkansas food law. The procedures are
used to train the staff members responsible for the tasks.
• Three purposes for establishing SOPs for your operation are: (1) to protect your products
from contamination from microbial, chemical, and physical hazards; (2) to control microbial
growth that can result from temperature abuse or poor personal hygiene; and (3) to ensure
procedures are in place for maintaining equipment and assisting with Active Managerial
Controls within the food establishment.
Why must procedures be submitted?
• Arkansas Food Regulations requires standard operating procedures to be established prior to
opening or reopening. These procedures must be maintained in the facility and accessible to
the staff and regulatory authorities upon request.
How must procedures be developed?
• Procedures are mostly for use by managers and staff. Develop procedures in the
language, style, and format best for the establishment. An English copy of the procedures
is needed for the plan reviewer.
What procedures must all establishments submit?
• Handwashing.
• Personal hygiene, including cuts and sores.
• Preventing bare hand contact with ready-to-eat food (gloves, utensils, etc.).
• Employee/Staff illness.
• Purchasing food from approved sources.
• Cleaning and sanitizing food contact surfaces.
• Norovirus Cleanup (See Regulatory Authority for assistance with approved procedure)
What procedures must all establishments develop when applicable to their operation?
• Cross-contamination prevention within the establishment
• Warewashing manual dishwashing
• Date-marking ready-to-eat, and TCS (time/temperature control for safety food).
• Using time only (not time and temperature) as a method to control bacterial growth.
• Thawing TCS foods (time temperature control for safety food).
• Cooking TCS foods (time temperature control for safety food).
• Cooling TCS foods (time temperature control for safety food).
• Reheating foods.
• Hot holding foods.
• Cold holding foods.
Procedures can be sent with the plans at time of initial review and maintained on-site and used by the
person in charge and staff. Technically correct procedures must be in place by the pre-opening
inspection.
7
EHP-PR1(4/24)
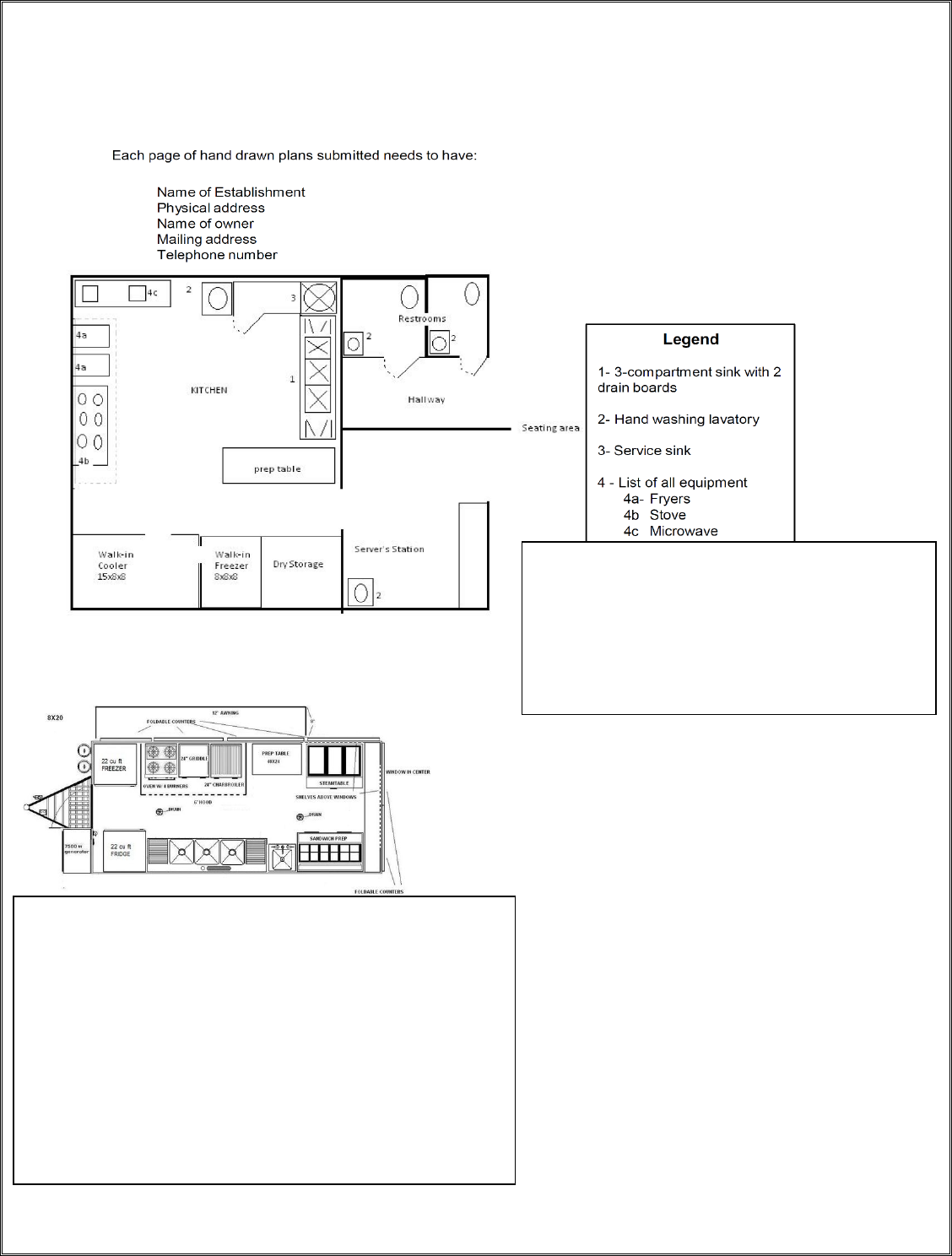
KITCHEN FLOOR PLAN
Please include the type of materials used for floors,
walls, and ceilings. Acceptable finishes would
include sealed concrete or tile for flooring; quarry
tile, fiberglass reinforced plastic (FRP) or stainless
steel for wall areas and coated tiled or other
smooth ceiling materials.
Photographs of the Facility/Mobile Units are encouraged.
Detailed images of the inside and outside of the food service
facility or mobile unit will be helpful and speed up the overall
review process for those already constructed facilities.
Example of Images to Take
• Kitchen layout, Equipment, Vent-hood, lighting
• Sinks, three-compartment, handwashing, mop sinks
• Buffet line, Dry Storage Unit, Hot Holding cabinets,
• Floors, Walls, Ceiling
• Walk-Ins, Freezers, Coolers
Plans should be remitted to:
Environmental Health Protection
Plan Review
Arkansas Department of Health
4815 W Markham St, Slot 46
Li
ttle Rock, AR 72205

8
EHP-PR1(4/24)
FOR AGENCY USE ONLY
FOR ESTABLISHMENTS NOT NEEDING RETAIL PLAN REVIEW
I have reviewed the paperwork submitted, have had conversations with the prospective new
operator related to their intended food preparation practices and menu, and/or have current
working knowledge of the condition of this facility. It is my recommendation that this facility
does not need to go through a Retail Plan Review.
EHS: ____________________________________ Signature: __________________________
DATE: ______________________________
RETAIL PLAN REVIEW COMMENT SECTION
Date Received Plans: ____________________ Date Completed: ________________
Final Approval Status: ________________ (Approval / Provisional Approval / Disapproval)
ACTION
DATE OF ACTION
BY WHOM
COMMENTS
Scanned PR Documents
Sent PR Letter
Put Plans On Hold
Plans Returned
Additional Documents
Rec’d
Payment Received
PLANS ON HOLD FOR THE FOLLOWING REASONS:
Reasons Plans Returned:

EHP-17 (4/24)
Page 1 of 2
Arkansas Department of Health
Project Cost Estimate Worksheet
As required by A.C.A. § 20-7-123, this worksheet must be completed and submitted with appropriate fee(s)
PROJECT NAME
COUNTY
PROJECT LO
CATION (911 if available)
CITY, STATE, ZIP
OWNER/SUBMITTER NAME PHONE
MAILING ADDRESS
CITY, STATE, ZIP CODE
EMAIL (if available)
COST ESTIMATE: ESTIMATED COST SHALL BE BASED ONLY ON THOSE IMPROVEMENTS THAT REQUIRE
A DEPARTMENT OF HEALTH REVIEW
1. WATER SYSTEM IMPROVEMENTS (non-plumbing)................................ $
For questions regarding water system improvements ENGINEERING (501) 661-2623
2. SEWER SYSTEM IMPROVEMENTS (non-plumbing) ................................ $
For questions regarding sewer system improvements ENGINEERING (501) 661-2623
3. PLUMBING…………………………………….……………….................. $
For questions regarding plumbing plans
(501) 661-2650
4. SWIMMING POOL (public)….………………............................................. $
For questions regarding swimming pool plans
(501) 661-2171
5.
FOOD SERVICE- Retail or Wholesale/Manufacturing (new/reno) .………......... $
For questions regarding food establishment plans
(501) 661-2171
TOTAL ESTIMATED COST ................................................................. $
A. PLAN REVIEW FEE .................................................................................. $
1% of total est. cost, not less than $50.00 and not to exceed $500.00 (See #1 on page 2)
TOTAL FEES SUBMITTED ................................................................... $
(Checks or money orders made payable to ADH)
PREPARED BY: DATE
PRINT NAME: __________________________________________________________
*For Individual Onsite Wastewater System permits and Subdivision, RV Parks, Mobile Home parks utilizing individual disposal systems
please continue to page 2 or contact Engineering (501) 661-2623.
PROJECT ID# (ADH Use Only)

EHP-17 (4/24)
Page 2 of 2
EXPLANATION OF PLAN REVIEW FEES
#1) A.C.A. § 20-7-123 establishing a fee for the review of plans and specifications which are
required by law or regulation to be reviewed by the Department (Line items #
1,2,3,4,5 on page 1). The fee is 1% of the estimated cost of improvements, with a minimum fee
of $50.00 and a maximum fee of $500.00. An Engineering estimate must accompany the plans
unless the maximum fee of $500.00 is paid.
IF TOTAL ESTIMATED COST IS $5,000.00 OR LESS, REVIEW FEE IS $50.00.
IF TOTAL ESTIMATED COST IS $50,000.00 OR MORE, REVIEW FEE IS $500.00.
IF TOTAL ESTIMATED COST IS BETW EEN $5,000.00 AND $50,000.00, CALCULATE AS FOLLOWS:
PLAN REVIEW FEE = (0.01) x (TOTAL ESTIMATED COST) = $
Complete Below Only for plans utilizing onsite wastewater systems including subdivisions
containing lots < 3 acres, mobile home and RV parks.
#2) A.C.A. § 14-236-116 establishing a fee for the review of plans for subdivisions containing lots
<3 acres utilizing individual onsite wastewater systems.
Subdivisions on Individual Onsite Wastewater :
FIRST LOT @ $100.00 $ 100___
ADDITIONAL LOTS @ $25.00/each .......................... $
TOTAL ........................................... $
(Maximum Fee = $1500.00)
#3) A
.C.A. § 20-27-1201 established a review fee for Mobile Home Parks and Recreational Vehicle
Parks utilizing onsite wastewater systems and is based on the number of spaces.
Mobile Home & RV Parks utilizing Onsite Wastewater Systems:
2-25 SPACES………………….
$25.00
26-50 SPACES………………..
$50.00
51-75 SPACES………………..
$75.00
76 OR MORE…..……………. $100.00
PLAN REVIEW FEE:
Total Submitted (#2 + #3) ___________________________________
(Checks or money orders payable to ADH)
For more information regarding Sections #2 and #3, please contact ADH Engineering 501-661-2623.

4815 W. Markham St., Slot 46
Little Rock, AR 72205
Yes No
Yes No
4-24

owner(s) or responsible representative(s)
Date
-4/24)
