
1
February 7, 2024
Rolling Out the Changes to Medicare’s
Prescription Drug Benefit: How Cost Sharing Is
Becoming More Affordable
The Inflation Reduction Act (IRA), a sweeping federal law enacted in August 2022, included many provisions aimed
at making prescription drugs more affordable under Medicare Part D, the Medicare program that provides
prescription drug coverage (see a previous Health Care in Motion for an overview of these changes). Two major
changes to Medicare Part D went into effect in January 2024 and will significantly impact certain Medicare
enrollees. Read on for a discussion of how these provisions work, including how they could impact a person living
with HIV or other high-cost condition, as well as related policy issues that will play out over the next year and
beyond as the IRA’s changes begin to take effect.
Medicare Extra Help Expansion
Many low-income Medicare enrollees are eligible for a
program called “Extra Help” also known as the “low-
income subsidy” (LIS), which helps qualifying Medicare
Part D beneficiaries with their premiums, deductibles,
copayments, and coinsurance. Starting in January 2024,
full Extra Help is now available to individuals with income
less than 150% FPL (prior to 2024, individuals from 135-
150% FPL were only eligible for partial subsidies). This
change has significant potential to help lower income
individuals who rely on high-cost medications or who need
to fill many prescriptions at once. In 2024, those with full
Extra Help will pay a low or no premium for their drug
plan, will have no deductible, and will pay at most $4.50 in
copayments for generic drugs and $11.20 in copayments
for brand-name drugs.
HHS estimates that nearly 300,000 low-income people
with Medicare who were previously enrolled in the partial Extra Help program are newly eligible for the full
Medicare Beneficiaries Are Not Aware of These
New Changes
Kaiser Family Foundation polling indicates that only
about a quarter of Medicare beneficiaries are
aware of many of the IRA’s Medicare Part D
consumer protections. There may be more work to
do for CMS, assisters, and health care advocates
working with Medicare beneficiaries to ensure that
people are aware of the expansion of the Extra
Help program and new cost sharing reforms.
CMS has put out a social media toolkit to raise
awareness. Medicare Rights Center has also
published a helpful guide of new Medicare
protections that will benefit consumers in 2024.
2
benefit. The expansion of Extra Help and the effort to get the word out about eligibility may also help to reach
the millions of Medicare enrollees that may be eligible for Extra Help but are not enrolled.
Medicare Part D Cost Sharing Changes
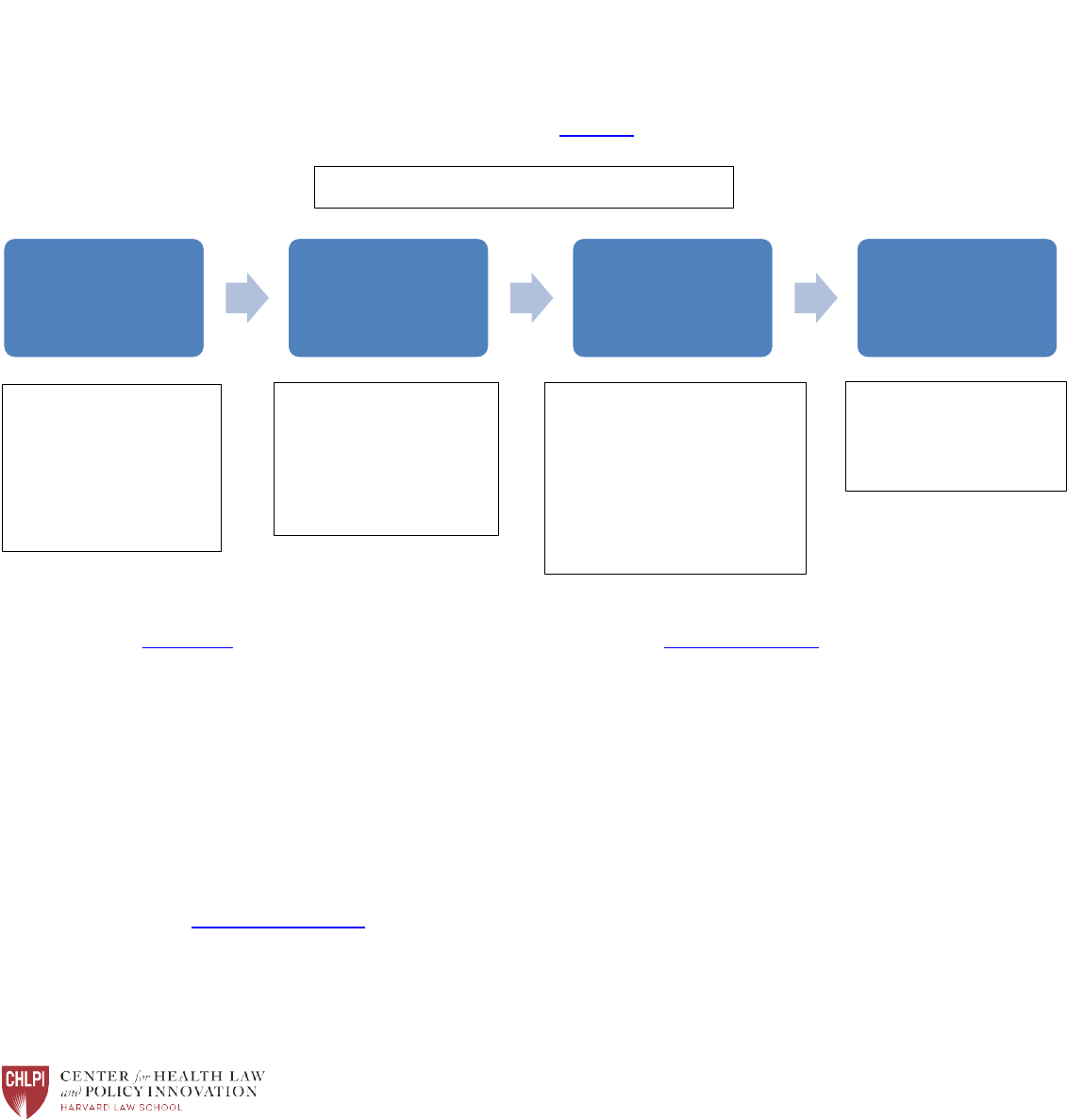
The IRA also made changes to cost sharing for Medicare Part D plan members. Cost sharing in Medicare Part D
changes throughout the year as beneficiaries move through the different phases of coverage as shown in the
chart below. Starting in January 2024, patients with high prescription drug costs will not have to pay any
additional cost sharing once they reach a certain level of out-of-pocket spending known as the catastrophic
coverage phase. Prior to 2024, consumers had to pay 5% coinsurance for their drugs once they reached this
phase. Researchers at Kaiser Family Foundation estimated that prior to the IRA’s cost-sharing reforms, for
some very high-cost drugs, consumers could pay as much as $12,000 in the catastrophic phase alone.
Because the $8,000 in out-of-pocket costs that Part D members need to hit to reach catastrophic coverage
phase includes payments that others have made on a member’s behalf, experts estimate that the amount a
beneficiary spends on cost sharing for brand-name drugs before hitting the catastrophic coverage is
approximately $3,300 in 2024. In other words, for brand-name drugs, Medicare Part D consumer cost sharing
is capped at approximately $3,300 in 2024. This could be a significant improvement for many Part D members
who rely on high-cost drugs.
Illustration: Sample Patient Living with HIV
To show how these changes could impact Medicare enrollees who require high-cost drugs and who do not get
Extra Help, below is a chart showing how drug cost sharing could change this year for a person living with HIV
and hypertension (a common condition among people with HIV who are aging). As the chart shows, the
Medicare Part D changes this year have the potential to help people living with HIV—and others who rely on
high-cost medications—save a significant amount.
Deductible
Phase
Initial
Coverage
Coverage
Gap
Catastrophic
Coverage
Individual pays full
negotiated price for
covered drugs (up to
a maximum
deductible of $545)
Individual pays a
copay or coinsurance
until they have
reached $5,030 in
total drug costs
Individual pays 25%
coinsurance (plan and
manufacturer pay 75%)
until the individual
reaches $8,000 in out-of-
pocket drug costs
Individual pays $0
for the rest of the
year
Medicare Part D Cost Sharing in 2024

3
Consumer Cost Sharing for Biktarvy (brand-name drug used to treat HIV) and
lisinopril 5mg (generic medication used to treat hypertension)
• List price of Biktarvy = $3,000/30 day
• List price of lisinopril = $10/30 days
2023
• Enrollee hits deductible of $505 at first fill
• Enrollee pays $750 per fill for Biktarvy and $2 per fill for lisinopril during both the
initial and coverage gap phases
• After ~$3,100 in out-of-pocket costs, enrollee enters catastrophic coverage phase in
May, where cost sharing is $150 for Biktarvy and less than $1 for lisinopril for the
rest of the year
• This could add up to $1,050 just in the catastrophic coverage phase for a total of
$4,150
2024
• Enrollee hits deductible of $545 at first fill
• Enrollee pays $750 per fill for Biktarvy and $2 per fill for lisinopril during both the
initial and coverage gap phases
• Once enrollee spends ~$3,300 out-of-pocket, which will happen in May, $0 cost
sharing for the rest of the plan year
*Chart is for hypothetical purposes only and does not reflect actual costs for any individual consumer.
One wrinkle here is that many Medicare enrollees living with HIV already get assistance covering their
copayments through the Ryan White HIV/AIDS Program and state AIDS Drug Assistance Programs (ADAPs),
which help people with HIV afford their HIV-related medication costs. For Medicare enrollees who receive
assistance through ADAP, their out-of-pocket costs for HIV-related medications may change very little or not
at all because ADAP is paying their copayments or coinsurance. The payments that ADAP makes on behalf of a
Medicare Part D enrollee count as “true out-of-pocket” costs, or “TrOOP,” meaning that a client for whom
ADAP is making Part D copayments will still move through the coverage phases.
For their part, state ADAPs may have to assess how the changes to Medicare Part D will affect their financial
sustainability. Many ADAPs are able to generate savings, in the form of manufacturer rebates, on the cost
sharing assistance they provide for clients enrolled in Medicare Part D. However, if there is no cost sharing for
any given month – for instance, once a client reaches an out-of-pocket cap or maximum – the ADAP cannot
generate a rebate. While it is beneficial for the client to hit an out-of-pocket maximum early in the plan year,
fewer months in which there is a cost sharing charge for the ADAP to pay may reduce the savings an ADAP is
able to generate from manufacturer rebates, thereby reducing the amount the ADAP can reinvest back into
the program.
What’s Next?
More changes are coming to the Medicare prescription drug program. Starting in 2025, total out-of-pocket costs
for Medicare Part D will be capped at $2,000, and beneficiaries will be able to spread out their drug costs over the
course of the year through a new “smoothing” mechanism (for more discussion of these provisions, see a recent
Health Care in Motion). CMS is still working out the details of how the smoothing option will work, and there may
be opportunities for advocates to weigh in to ensure that this option is as accessible and understandable as
possible for those who stand to benefit from it.

4
The IRA’s drug pricing provisions are also still progressing. CMS is in the middle of the first round of negotiations for
the ten drugs announced last year. The first negotiated prices will go into effect until 2026. The drug pricing
provisions are still subject to ongoing litigation, but the law remains in place for now.
Medicare Part D is undergoing many reforms aimed at making the program more affordable and accessible for
enrollees. As these reforms are implemented, it will be critical for advocates and people living with complex and
chronic conditions to weigh in with CMS through listening sessions, notice and comment periods, and other
communication opportunities.
Health Care in Motion is written by Carmel Shachar, Health Law and Policy Clinic Faculty Director; Kevin Costello,
Litigation Director; Elizabeth Kaplan, Director of Health Care Access; Maryanne Tomazic, Clinical Instructor; Rachel
Landauer, Clinical Instructor; Johnathon Card, Staff Attorney; and Suzanne Davies, Clinical Fellow. This issue was
written with the assistance of Amy Killelea of Killelea Consulting.
For further questions or inquiries please contact us at [email protected].
Subscribe to all Health Care in Motion Updates
