
Access to Care for COPD
and Lung Cancer Patients
Under Current Essential
Health Benefit Standards

2
The Affordable Care Act (ACA) established 10 categories of essential health benefits
(EHBs) that health plans in the individual and small group markets and Medicaid
expansion plans must cover. EHBs are designed to ensure that patients have access to
comprehensive healthcare coverage that includes the emergency services, preventive
services, prescription drugs, and other critical treatments and services that they need. In
2013, the Secretary of Health and Human Services (HHS) issued regulations implementing
standards for EHB which included a process for each state to select their own
benchmark plan, supplemented by federal standards in a few specific coverage areas.
Over a decade later, changes to the benchmarking process and federal standards for
EHB have been limited. The Lung Association commissioned a review of EHB benchmark
plans and silver plans offered in the ACA marketplaces in five states to determine
whether those benchmark and silver plans provided access to the treatments and
services that patients with COPD and lung cancer would need to treat their conditions.
Key findings include:
• Lack of Transparency: In multiple areas, both benchmark plans and silver plans
lacked key details to determine whether they met the standard of care for COPD
and lung cancer.
• Failure to Keep Up with Medical Advancement: In the past decade, comprehensive
biomarker testing has connected patients with lung cancer with targeted therapies
that drastically improve their prognosis, yet none of the benchmark plans provided
guidance on biomarker testing.
Executive Summary

3
• Barriers to Accessing Recommended Treatments: Certain recommended
medications for both COPD and lung cancer were not covered by all plans and
included barriers like prior authorization, quantity limits, and placement on specialty
tiers. Additionally, some plans had visit limits for pulmonary rehabilitation that
compromised access to the standard of care.
• Lack of Oversight and Enforcement: Both the benchmark plans and all but one
state’s silver plans were not consistently covering tobacco cessation treatment, a
preventive service required to be covered under the current EHB standards.
These gaps demonstrate a clear need to update and better enforce current EHB
standards to ensure that patients have access to guidelines-based care. In 2022, the
Biden administration released a request for information on EHB. As the administration
continues to explore this issue, the Lung Association offers the following policy
recommendations to address the gaps found in this analysis:
• Conduct a comprehensive review of EHB standards. HHS should establish a
regular, evidence-based process that incorporates input from patients and other
stakeholders on gaps in the current EHB framework.
• Update coverage requirements in areas where there have been important
changes in science and medicine since 2013. This should include additional
guidance on biomarker testing under the laboratory services category of EHB.
• Strengthen the prescription drug standard. The EHB standard should require
coverage of a minimum of two drugs per US Pharmacopeia (USP) class and
category or the number covered by the benchmark plan, whichever is greater,
as well as “all or substantially all” drugs in certain specified classes, similar to the
approach adopted in Medicare Part D.
• Restrict limits on evidence-based care. Any utilization management or other limits
on treatments and services must be guidelines-based and not used to arbitrarily
restrict access to EHB treatments and services.
• Improve oversight and enforcement of existing EHB standards. Greater resources
are needed to ensure that plans meet existing coverage standards, especially for
preventive care like tobacco cessation.

4
Introduction
The Affordable Care Act (ACA) established 10 categories of essential health benefits
(EHBs) that health plans in the individual and small group markets and Medicaid
expansion plans must cover.
1
EHBs are vital for patients with and at risk for lung disease
to access the comprehensive care that they need. These standards have expanded
access to preventive services like lung cancer screening and tobacco cessation,
prescription medications, habilitative and rehabilitative care like pulmonary rehabilitation,
and many other important treatments and services (see below).
10 Essential Health Benefits
Ambulatory patient services Emergency services
Hospitalization
Mental health and substance
use disorder services including
behavioral health treatment
Maternity and newborn care
Prescription drugs
Rehabilitative and habilitative
services and devices
Laboratory services
Preventive and wellness
services and chronic disease
management
Pediatric services, including
oral and vision care
1 6
2 7
3 8
4 9
5 10
1. Certain health insurance policies purchased on or before March 23, 2010 that have “grandfathered” status do not have to comply
with these requirements.

5
In 2013, the Secretary of Health and Human Services (HHS) issued regulations
implementing standards for EHB which included a process for each state to select their
own benchmark plan.
1
States could choose from a number of options – the three largest
small group plans in their state, the three largest
state employee plans in their state, the three
largest federal employee health plans, or the health
maintenance organization plan in the state with the
largest commercial, non-Medicaid enrollment. The
state benchmark plan then served as a guide for
insurers in each state to design their plans for the
individual and small group markets, including those
sold through the ACA’s exchanges. Insurers also
had to design their plans to comply with additional
federal standards in certain coverage areas, such
as preventive services and prescription drugs.
Currently, the state benchmark process relies
on benefit designs that are more than five
years old. Additionally, lessons learned from the
implementation of these standards over the
past decade, as well as changes in science and
medicine, have highlighted areas of needed
improvement. In 2022, the Biden administration
released a request for information on EHB and the American Lung Association submitted
detailed comments identifying some of the gaps in the current EHB standards that make
it harder for patients with lung disease to access the care that they need.
2
In 2023, the Lung Association commissioned Avalere to assess whether there are gaps
in EHB benchmark plans, as well as in the individual market coverage sold through the
ACA’s exchanges based on those benchmark plans, that impede access to care for
individuals with COPD and lung cancer. Avalere conducted a comparative analysis of
EHB for 2023 silver plans on the ACA exchanges within the largest ZIP codes for five
states: Louisiana (70726), Maryland (20906), Michigan (48197), New Mexico (87121), and
Pennsylvania (19120). This study examined whether the selected states’ EHB benchmark
plans provided sufficient guidance and whether silver plans offered sufficient coverage to
meet the standard of care for individuals with lung cancer or COPD.
Currently, the state
benchmark process
relies on benefit
designs that are more
than five years old.

6
Methodology
Based on clinical expertise, national standards, and guidance to develop treatment protocols,
Avalere created a standard of care for COPD and lung cancer patients. The treatment
protocols included details on the severity of the condition, symptoms experienced, smoking
history, schedule of treatments, drug coverage, and services required (Table 1 and 2).
Table 1 – Standard of Care for COPD
Hypothetical Patient
Overview
A 59-year-old male was diagnosed with moderate to severe COPD
last year and a history of smoking (30 pack year). The patient is up to
date with routine vaccinations, including the COVID-19 vaccine.
Diagnostic Overview The patient would require hospitalization due to COPD exacerbation.
The discharge summary includes the following description: patient
arrived with a persistent, nonproductive cough; Chest computerized
tomography (CT) shows moderate consolidation constant with
chronic bronchitis.
Drug Utilization Overview The patient is currently prescribed varenicline, albuterol (rescue
inhaler), and a COPD maintenance therapy medication.
Service Utilization Frequency of Visit Schedule
Medical Services
Routine Primary Care
Provider Visits
4 Jan, June, July, Nov
Specialist Visit (Pulmonologist) 2 Feb, July
Hospitalization (5 days) 1 July
Pulmonary Rehab Visits 24 July–Dec
Diagnostic Services
Pulse Oximetry 5 Jan, Feb, June, July, Nov
Arterial Blood Gas Testing 1 (Additional tests as needed) July
Spirometry Testing 1 (Additional tests as needed) July
Chest X-Ray 1 (Additional tests as needed) July
Sputum Culture 1 (Additional tests as needed) July
Electrocardiogram (EKG) –
Annual
1 (Additional tests as needed) Jan
Preventive Services
Tobacco Cessation Services —
Continuing weeks: 1 mg twice
daily for a total of 24 weeks
COVID-19 Immunization — 2 doses
7
Table 2 – Standard of Care for Lung Cancer
Hypothetical Patient
Overview
A 60-year-old female and former smoker (20 pack year).
Diagnostic Overview The patient received a diagnostic computed tomography (CT)
scan following the low dose computed tomography (LDCT) scan,
revealing a large mass (4 cm) in the left lung with lymph node
involvement.
A needle biopsy confirmed non-squamous adenocarcinoma
of the lung, and her positron emission tomography (PET) scan
and CT was consistent with extensive bone metastases. The
patient was diagnosed with ROS1 fusion gene adenocarcinoma,
confirmed by next-generation sequencing (NGS) testing, also
known as biomarker testing.
Drug Utilization Overview The patient was placed on targeted oral therapy with crizotinib,
which resulted in disease stabilization through the end of the year.
Service Utilization Frequency of Visit Schedule
Medical Services
Routine Primary Care
Provider Visits
1 Jan
Specialist Visit (Oncologist) 14 Jan–Dec
Specialist Visit (Cardiologist) 6 Jan, Mar, May, July, Sept, Nov
Pulmonary Rehab Visits 24 July–Dec
Diagnostic Services – Labs
Bloodwork – Comprehensive
Metabolic Panel and Complete
Blood Count
12 Jan–Dec
Bloodwork – Liver Panel 2 Jan–Feb
Diagnostic Services – Scans
Electrocardiogram (EKG) 6 Jan, Mar, May, July, Sept, Nov
PET Scan 6 Jan, Mar, May, July, Sept, Nov
CT Scan 6 Jan, Mar, May, July, Sept, Nov
Needle Biopsy 1 Jan
NGS Test (including ROS1) 1 Jan
Preventive Services
LDCT Scan 1 Jan

8
Selection of States & Approach to Selecting Plans
Avalere and the Lung
Association selected five
states (state-based and
federal exchanges) with
diverse and expansive
populations to offer
a range of variations
among state plan benefits
and descriptions. The
chosen states (Louisiana,
Maryland, Michigan, New Mexico
and Pennsylvania) vary in terms of
type of marketplace, population size, and
demographics. Next, Avalere researched and
categorized silver plans within the most populous ZIP codes of each state based on
the availability of services and treatments for COPD and lung cancer patients.
EHB Benchmark and Silver Plan Analysis
Avalere assessed whether the states’ EHB benchmark plans covered each treatment or
service outlined in the standard of care for each condition in the analysis. Avalere also
completed a separate and similar analysis to determine whether the state silver plans
met the state EHB benchmark plan and/or the standard of care. Avalere then evaluated
and categorized each treatment or service outlined in the standard of care into the
following groupings.
The state EHB benchmark plans included the following categories:
• Meets the Standard of Care
• Does Not Meet the Standard of Care
• Coverage Details Not Specified
The silver plans in each state included the following categories:
• Meets Benchmark
• Exceeds Benchmark
• Does Not Meet Benchmark
• Coverage Details Not Specified

9
Next, Avalere calculated the proportion of state EHB benchmark plans that met the
standard of care, did not meet the standard of care, or did not provide sufficient coverage
details (“benchmark details were not specified”). Avalere calculated the proportion of
silver plans in each state that met the benchmark plan, exceeded the benchmark plan,
did not meet the meet benchmark plan, or the coverage details were not specified. Lastly,
Avalere conducted a qualitative review of the silver plans that met the state benchmark
plan but did not meet the standard of care.
Formulary Analysis
Avalere evaluated the coverage, tiering and utilization management for each prescription
drug included in the standard of care for COPD and lung cancer.
2
There are Food and
Drug Administration (FDA) approved treatments for COPD and lung cancer that were not
listed in the standard of care and not included in this analysis. Avalere assessed brand
and generic coverage, limited to the availability of drugs within the formulary database.
Most health plans have a prescription drug formulary that indicates which brand and
generic drugs the health plan will cover and the cost sharing requirements for the patient.
Plan formularies assign prescription drugs to tiers, which designate each drug’s coverage,
commonly noted as preferred, non-preferred, or specialty. Preferred tiers are associated
with lower cost sharing for the patient compared to non-preferred and specialty tiers.
2. Avalere partners with Clarivate™ to obtain formulary data and pharmacy lives covered across all payer types. Specific data included
herein are derived from the Fingertip Analytics© of Clarivate. All rights reserved. Data current as of February 2023.

10
Results
Avalere utilized the standard of care for COPD and lung cancer to
conduct research across the five states included in this analysis.
Avalere located state benchmark plans and identified coverage
based on the standard of care for both conditions. The standard
of care for COPD and lung cancer patients included inpatient and
outpatient care, specialist visits, diagnostic testing, prescription drug
coverage, and preventive services.
Avalere researched available plans in the most populous ZIP codes
across five states. Federal exchange plan summaries were more
accessible via internet searches in comparison to state-based
exchange plans. Additionally, a considerable number of complete
plan brochures were not available for download across all five states.
Most plan brochures that were available did not provide coverage
details on types of specialists or specific information on inpatient
services and treatments.

11
Table 3 – State EHB Benchmark Plans and Silver Plans
in Most Populous ZIP Codes of Five States
3
State
ZIP
Code
County/
Parish
Number
of Silver
Plans
Qualitative Assessment
Louisiana 70726 Livingston 18
The state benchmark plan did not meet the
standard of care for COPD due to gaps in
tobacco cessation.
The state benchmark plan did not provide
specific details to determine coverage of lung
cancer screening or biomarker testing.
Maryland 20906 Montgomery 10
The state benchmark plan did not meet the
standard of care for COPD because the plan
limited pulmonary rehabilitation benefits.
The state benchmark plan did not provide
specific details to determine coverage for
biomarker testing.
Michigan 48197 Washtenaw 36
The state benchmark plan included all services
and treatments included in the standard of care
for COPD.
The state benchmark plan did not include
specific details to determine coverage for
biomarker testing.
New Mexico 87121 Bernalillo 7
The state benchmark plan met the standard of
care for all services and treatments included in
the standard of care for COPD.
The state benchmark plan did not include
specific details to determine coverage for
biomarker testing.
Pennsylvania 19120 Philadelphia 26
The state benchmark plan met the standard of
care for all services and treatments included in
the standard of care for COPD.
The state benchmark plan did not meet the
standard of care for lung cancer because it did
not specify lung cancer screening or reference
the USPSTF. The state benchmark plan also
did not provide sufficient details to determine
coverage for biomarker testing.
3. EHB benchmark plan types varied across states, which included plans from the largest small group product to the largest health
maintenance organization plan in a state. Small group plans were either a preferred provider organization, health maintenance
organization, or point of service plan.

12
Evaluation of State EHB Benchmark Plans
to the Standard of Care
Table 3 provides an overview of the benchmark plan analysis for each state. The standard
of care for COPD included pulmonary rehabilitation, an evidence-based program of
education and exercise for patients with COPD and other lung diseases designed to
improve lung function, reduce symptom severity and improve quality of life. Maryland’s
benchmark plan did not meet the standard of care for pulmonary rehabilitation because
the plan limited the number of visits and did not cover maintenance programs. The
program limited members to “one program per lifetime.”
The standard of care for COPD also included tobacco cessation. The US Preventive
Services Task Force (USPSTF) recommends behavioral interventions (counseling) and
FDA-approved medications for adults who use tobacco
products, and plans are legally required to cover both.
Louisiana’s benchmark plan did not meet the standard
of care for tobacco cessation coverage, as the plan
excluded all tobacco cessation programs, supplies, and
drugs. The exception was bupropion, which was the only
covered drug for tobacco cessation. The benchmark plan
also included language indicating that tobacco cessation
programs and drugs are not considered medically
necessary. The benchmark plan did not mention tobacco
cessation counseling. Louisiana’s benchmark plan drug formulary provided contradictory
information and listed varenicline as a covered drug for tobacco cessation. Additionally,
benchmark plans in Maryland, Michigan, and Pennsylvania only specified coverage of
pharmacotherapy for tobacco cessation treatment. The plans did not provide additional
details to determine whether individual or group counseling services were covered.
The standard of care for lung cancer included biomarker testing, which allows doctors to
identify abnormalities in a cancer cell’s DNA and determine the best course of treatment
for patients with lung cancer. However, none of the states’ EHB benchmark plans provided
sufficient details to determine coverage of biomarker testing for lung cancer patients.
Additionally, USPSTF recommends annual lung cancer screening for individuals at high
risk for lung cancer based on their age and smoking history. Louisiana’s benchmark
plan did not provide sufficient detail to determine whether lung cancer screenings were
covered. The benchmark plan coverage document lists other cancer screenings but does
not specifically list lung cancer screening. Pennsylvania’s benchmark plan also did not
specify lung cancer screening, and there is no reference to the USPSTF guidelines.
4
4. Plans that included references to the USPSTF were considered to have met the standard of care.

13
Evaluation of the State EHB Benchmark Plan
to Silver Plan Coverage
Avalere assessed silver plans compared to their state’s EHB benchmark plan. While silver
plan coverage may have equated to “meeting the benchmark,” their coverage details may
not have aligned with the standard of care. Table 4 shows coverage of select treatments
and services included in the standards of care for COPD and lung cancer across silver plans.
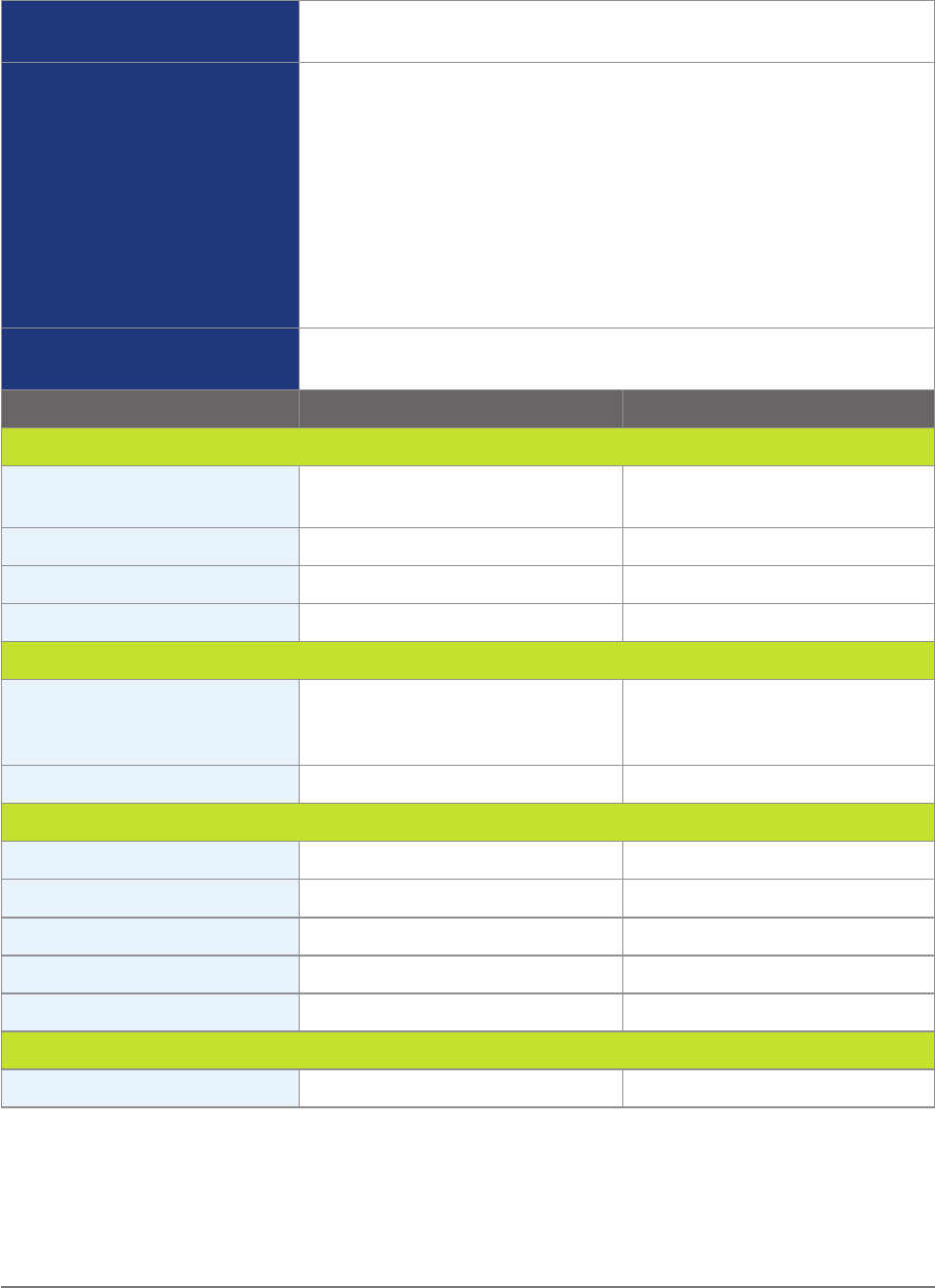
Table 4 – Percentage of Silver Plans in Most Populous ZIP Codes
in Five States that Met the Standard of Care for Select
Treatments and Services for COPD and Lung Cancer
Treatment or Service Louisiana Maryland Michigan New Mexico Pennsylvania
Albuterol 100% 100% 100% 100% 100%
Biomarker Testing 0% 0% 0% 0% 0%
COVID-19 Vaccine 100% 100% 100% 100% 100%
Crizotinib 72% 60% 78% 100% 100%
Fluticasone Furoate,
Umeclidinium &
Vilanterol
100% 100% 100% 71% 75%
Lung Cancer Screening 100% 100% 100% 100% 100%
Ondansetron 100% 100% 100% 100% 100%
Prednisone 100% 100% 100% 100% 100%
Pulmonary
Rehabilitation
89% 0% 100% 86% 100%
Varenicline 100% 60% 100% 100% 100%
Tobacco Cessation
Counseling
28% 0% 38% 100% 28%
Beginning with pulmonary rehabilitation, all silver plans in Maryland met the state
benchmark plan but did not meet the standard of care. Like the state’s EHB benchmark
plan, the silver plans limited pulmonary rehabilitation to “1 program per lifetime for an
enrollee diagnosed with significant pulmonary disease.” Additionally, four of the ten plans
did not provide maintenance programs for pulmonary rehabilitation. In the other states,
most silver plans met the state benchmark and either did not have quantitative visit
limits or had limits that exceeded the number of visits in the standard of care; however,
two silver plans reviewed in the largest ZIP code in Louisiana and one silver plan in the
largest ZIP code in New Mexico did not specify the details needed to determine whether
pulmonary rehabilitation services were covered.

14
The standards of care for both
COPD and lung cancer included
prescription drug coverage. Current
EHB standards require coverage of
only one drug per US Pharmacopeia
(USP) class or the number of
medications included in the USP
class in the state’s benchmark plan.
For COPD, all plans covered either
ProAir RespiClick® or albuterol
hydrofluoroalkanes, the generic
alternative, for rescue inhalers with
quantity limits. All plans also covered
prednisone without any utilization
management restrictions. However,
all plans did not cover fluticasone
furoate, umeclidinium & vilanterol
(Trelegy Ellipta®). This medication
was only covered in 71% of the
silver plans in New Mexico and 75%
of the silver plans in Pennsylvania.
Additionally, many plans covered this
maintenance therapy with quantity
limit restrictions, ranging from 54%
of the time in Pennsylvania to 89% of
the time in Louisiana.
For lung cancer, all silver plans covered
ondansetron, again with quantity limits.
As for the targeted therapy crizotinib
(Xalkori®), coverage varied across
states, and prior authorization was
required. Crizotinib was covered by
60% of the silver plans in Maryland,
72% in Louisiana, 78% in Michigan, and
100% in New Mexico and Pennsylvania.
Additionally, many silver plans across
all states listed crizotinib on the
specialty tier, ranging from 40% in
Maryland to 100% in New Mexico.
Patient Story
Renee is a patient with lung cancer
who received her healthcare through
the ACA marketplace for two years.
Renee had a positive experience with
the marketplace and eventually found
a suitable plan that facilitated the
continuation of her cancer treatments,
covering most medications and
treatments. However, Renee faced
significant difficulties in obtaining
coverage for a crucial medication
following her plan selection, a targeted
immunotherapy that is very expensive
when not covered through insurance.
She was very fortunate to be able
to afford this medication despite
insurance not covering it and continued
with her cancer treatment. Patients like
Renee need access to all guidelines-
based medications for successful
management of their conditions.

15
Continuing with lung cancer, Avalere found that 100% of silver plans across all five states
cover lung cancer screening by referencing the USPSTF, even though the state EHB
benchmark plans in Louisiana and Pennsylvania did not reference the USPSTF. However,
all silver plans failed to meet the standard of care based on diagnostic testing. No state
silver plans listed biomarker testing in diagnostic coverage.
Finally, for tobacco cessation, Avalere found 100% of silver plans in the most populous
ZIP codes in Louisiana, New Mexico, Michigan, and Pennsylvania listed varenicline in
formularies. In Maryland, only 60% of the plans in the most populous ZIP code listed
varenicline. The standard of care for tobacco cessation treatment for the COPD patient
included varenicline. The branded product for this drug is no longer being produced.
Some plan formularies continued to list the brand and others listed generic varenicline,
along with other tobacco cessation treatments.
5
The coverage of tobacco cessation counseling services was more limited. Only one
state, New Mexico, provided detailed coverage for tobacco cessation counseling for
all silver plans in the largest ZIP code. Only 38% of silver plans in the largest ZIP code
in Michigan and 28% of silver plans in the largest ZIP codes of both Louisiana and
Pennsylvania covered tobacco cessation counseling. No silver plan in the largest ZIP
code in Maryland covered tobacco cessation counseling.
5. This analysis focused on a specific set of drugs for review. The analysis did not include all drugs for the conditions included in this
review. The analysis does not reflect a lack of coverage for any FDA approved drugs used for these conditions.

16
Discussion
These results reveal a number of key gaps in the design and implementation of the
current EHB standards. First, a lack of transparency in both benchmark plans and silver
plans makes it difficult to determine whether patients have access to guidelines-based
care for COPD and lung cancer. For example, a substantial number of health plan
brochures did not specifically list or enumerate
coverage details for pulmonary rehabilitation
services, and the number of sessions covered
was not commonly listed. Similarly, preventive
healthcare coverage was not always readily
available in plan brochures. Details on tobacco
cessation coverage, vaccination coverage
and healthcare screenings required significant
research. Consumers should not be expected
to do extensive research to determine if critical
services are covered by their plan.
Second, EHB standards have failed to keep up
with changes in science and medicine over the
past decade, including biomarker testing. In the
past decade, comprehensive biomarker testing
has connected patients with targeted therapies
that drastically improve their prognosis. Studies
show that lung cancer patients that have
access to biomarker testing and are thus able
to receive targeted therapy treatments have
better overall chances of survival.
3
However, coverage details were not specified for
biomarker testing across all state EHB benchmark plans and across all silver plans within
the largest ZIP code within each state, jeopardizing patients’ access to these critical
medical advances.
A lack of transparency
makes it difficult to
determine whether
patients have access
to care.

17
Third, the results of this analysis indicate there are barriers to accessing certain
treatments recommended for COPD and lung cancer. Certain recommended medications
for both COPD and lung cancer were not covered by all plans. Additionally, many
medications included barriers like prior authorization, quantity limits, and placement
on specialty tiers, which typically have higher cost-sharing. Visit limits for pulmonary
rehabilitation were a barrier as well. These barriers have important implications for
patients. For example, research has shown that even relatively low levels of cost-sharing
limit the use of necessary healthcare services.
4
Similarly, prior authorization requirements
can delay patients’ access to care and even lead some patients to abandon treatment.
5
Finally, the results of this analysis suggest there are substantial gaps in the coverage
of tobacco cessation treatment, especially in terms of coverage of counseling. Despite
requirements to cover USPSTF-recommended preventive services, in three of the five
states, only a fraction of the silver plans covered tobacco cessation counseling and in one
state, there was no coverage of tobacco cessation counseling. This highlights the lack of
oversight and enforcement of current EHB standards for preventive services.
Overall, the lack of transparency and gaps in access to key treatments and services
across plans makes it more difficult for patients shopping for coverage to know with
any certainty what is covered and to choose the optimal plan for their health needs.
Ultimately, when plans do not cover these treatments and services, patients will either
be forced to choose between paying more to access the care that they need or delaying
recommended treatments and services, often resulting in more costly care in the future
and poorer health outcomes.

18
Policy Recommendations
These gaps demonstrate a clear need to update and enforce current EHB standards to
ensure that patients have access to evidence-based care. As policymakers continue to
explore this issue, the Lung Association offers the following recommendations to address
the gaps found in this analysis:
Improve oversight and enforcement of existing EHB standards.
Greater resources are needed to ensure that plans meet existing coverage
standards, especially for preventive care like tobacco cessation.
5
Restrict limits on evidence-based care. Any utilization management or
other limits on treatments and services must be guidelines-based and not
used to arbitrarily restrict access to EHB treatments and services.
4
Strengthen the prescription drug standard. The EHB standard should
require coverage of a minimum of two drugs per US Pharmacopeia
(USP) class and category or the number covered by the benchmark plan,
whichever is greater, as well as “all or substantially all” drugs in certain
specified classes, similar to the approach adopted in Medicare Part D.
3
Update coverage requirements in areas where there have been
important changes in science and medicine since 2013. This should
include additional guidance on biomarker testing under the laboratory
services category of EHB.
2
Conduct a comprehensive review of EHB standards. HHS should
establish a regular, evidence-based process that incorporates input from
patients and other stakeholders on gaps in the current EHB framework.
1

19
Acknowledgments
References
1. Centers for Medicare and Medicaid Services, Essential Health Benefits Standards: Ensuring Quality,
Affordable Coverage. Accessed July 2023. Available at https://www.cms.gov/cciio/resources/fact-
sheets-and-faqs/ehb-2-20-2013.
2. American Lung Association, Comments on Request for Information on Essential Health Benefits. January
30, 2023. Available at https:/
/www.lung.org/getmedia/fdd49013-1ac5-461d-b887-4ec0240df9a4/
American-Lung-Association-EHB-Comments-Final.pdf.
3. John A, Shah RA, Wong WB, Schneider CE, Alexander M. Value of Precision Medicine in Advanced Non-
Small Cell Lung Cancer: Real-World Outcomes Associated with the Use of Companion Diagnostics.
Oncologist. 2020 Nov; 25(11):e1743-e1752. Available at https://pubmed.ncbi.nlm.nih.gov/32627882/;
Howlader N, Forjaz G, Mooradian MJ, Meza R, Kong CY, Cronin KA, Mariotto AB, Lowy DR, Feuer EJ. The
Effect of Advances in Lung-Cancer Treatment on Population Mortality. N Engl J Med. 2020 Aug 13;
383(7):640-649. Available at https://pubmed.ncbi.nlm.nih.gov/32786189/.
4. Samantha Artiga, Petry Ubri, and Julia Zur, “The Effects of Premiums and Cost Sharing on Low-Income
Populations: Updated Review of Research Findings,” Kaiser Family Foundation, June 2017. Available at
https://www.kff.org/medicaid/issue-brief/the-effects-of-premiums-and-cost-sharing-on-low-income-
populations-updated-review-of-research-findings/.
5. American Medical Association, 2022 AMA Prior Authorization (PA) Physician Survey. Feb. Available at
https://www.ama-assn.org/system/files/prior-authorization-survey.pdf.
Avalere Health, LLC provided the analysis of the data depicted in this
American Lung Association publication. Avalere Health, LLC does not
expressly or implicitly endorse the American Lung Association’s or any
third-party’s products or services, and the deliverables provided by
Avalere to the American Lung Association were neutral in nature.

